
THE WAR
When I first heard the CTT at Oxford had published their latest analysis on statin adverse effects I must admit I sighed deeply. Do they never give up? This was the latest salvo in a long running war between the pro-statinators and the anti-statinators. Or, as I like to think of it, those who are wrong, and those who are right.
Why is there such a war? Because, and for reasons that I still find difficult to fully comprehend, statins have reached the position where they are believed to be the miracle cardiovascular drugs. With uniquely powerful lifesaving properties. ‘All hail the mighty statin’.
A friend was recently told to take atorvastatin. She was additionally told that if she did not, she would most likely die of a stroke or heart attack. Does anyone believe this is a reasonable thing for a doctor to tell a patient? So much for a therapeutic, non-paternalistic, healing partnership.
I cannot think of any other medical intervention where you get the added threat of oblivion thrown in for good measure. I suppose it happens with blood pressure lowering tablets from time to time. Maybe a few others. Chemotherapy? Vaccines, certainly, but that is a whole different ball game.
With most other drugs, if you think they are causing problems, the doctor will be reasonably happy to switch, or even stop. With statins there is a relentless pressure to keep on taking them. No matter what.
It is true that you may be allowed to move around between various statins, but as for stopping completely. You will be most likely be told this, or some version of it. ‘If you stop taking them, you will have a stroke or heart attack, and die!’
I have read countless e-mails from patients who have been told by their doctor that they will be thrown of the list if they refuse statins. Not from the UK, but in the US. Where it seems easier to fling people off your medical list. How nice it must be to have such, responsibility free, power. ‘I shall deign to treat you, so long as you do exactly as I command. Look upon my works, ye mighty, and despair.’
On a wider scale, if you talk to the media, or even write peer-reviewed articles suggesting that statins are anything other than miraculous life savers, you will be relentlessly attacked. I speak from personal experience, and a five year long libel trial.
Others have lost their jobs. Uffe Ravnskov, a long-time statin critic had his book The Cholesterol Myth burned, live, on air, in a TV studio. Dr Maryanne Demasi was booted off her job on the Australian Broadcasting Company. Then, for good measure, they tried to strip her of her PhD. Pour encourager les autres, I presume.
Kilmer McCully was flung out of Harvard for, in essence, pursuing ‘non-cholesterol related’ ideas on heart disease. His treatment was commented on by Thomas N James in a New York Times article. Kilmer was attacked in the 1970s, so this goes way back.
Thomas N. James, a cardiologist and president of the University of Texas Medical Branch who was also the president of the American Heart Association in 1979 and ’80, is even harsher [regarding the treatment of McCully]. ”It was worse than that you couldn’t get ideas funded that went in other directions than cholesterol,” he says. ”You were intentionally discouraged from pursuing alternative questions. I’ve never dealt with a subject in my life that elicited such an immediate hostile response.” 1
Just what the hell is it with statins and cholesterol lowering? I think I know this area as well as anyone, if not better than most. But I still find it difficult to work out where the level of conflict and aggression comes from. The polarisation of views.
It seems to go well beyond all rational behaviour. When two tribes go to war? Or maybe, to quote Cass Sunstein, author of Nudge. ‘To become an extremist, hang around with people you agree with.’
The benefits of statins – as I see them
I have studied the benefits of statins for many, many years. Probably too many, in truth. And, assuming the clinical trials were not entirely fabricated, I agree that they have some benefits. I do not think they are great, but they exist.
Can they be fully quantified? I could end up quoting paper after paper at this point, but I will restrict myself to two, and a bit. The first is a meta-analysis of twenty-one statin trials published in the Journal of the American Medical Association. It was pretty thorough, and one of the most recent – that I am aware of.
They found that statins led to a reduction of:
- 0.4% for stroke, fatal and non-fatal.
- 1.3% for myocardial infarction – fatal and non-fatal
- 0.8% reduction of dying (of anything)
These benefits accrued after about four years of taking a statin, on average. Sticking to overall mortality at this point, and using their 0.8% reduction figure, you could expect to see a reduced risk of death of around 0.2% a year. 2
Which is clearly important, but only in so far as it goes. I say this because the 0.2% figure certainly does not represent the end of the story. It is not enough to know how many more people were alive when the study ended. It is, in my opinion, far more important to establish what this means for an increase in life expectancy.
Reducing risk of death, and increasing life expectancy. No, they do not mean the same thing – at all. Even though they sound as though they probably should. And, while there is clearly a relationship between the two – it may not be what you think.
To use an extreme example. CPR may stop you dying of a heart attack on Tuesday, only for you to suffer a second heart attack, then die, on Wednesday. Or it could stop you dying on Tuesday, and then you live happily for another forty years. It is important to know which of these is most likely to happen – on average. One day, or forty years.
My view is that the effect on life expectancy is the single most important outcome we have. Especially when you are looking at an intervention designed to ‘prevent’ future events from occurring.
In cancer this is what used to be measured, and presented. The main reported outcome was, ‘increase in median life expectancy’. Which is not quite the same thing as average life expectancy, but … for the sake of this argument, it is close enough.
If a cancer drug is found to increase life expectancy by, say, around six months in a clinical trial, the patient will be told, something on the lines of…’if you take this drug it should give you another six months of life.’ [Cancer trials have now moved away from this endpoint, instead they look at other things, such as progression free survival (PFS). This has not been universally welcomed, other than by the pharmaceutical industry*]
Increase in life expectancy has never has been an outcome for cardiovascular trials. Why not? Well, there are valid statistical reasons. Median survival means the time it takes for fifty per cent of the trial population to die, in both arms. Drug vs. placebo, or new drug vs. standard management.
Sadly, this can happen rather quickly in cancer trials. But it could take twenty or thirty years to get to this point in a cardiovascular trial. And no-one is waiting that long. Apart from anything else, the patent protection for the drug would have run out before the trial finished.
Instead, in a cardiovascular trial, they (may) tell you the percentage reduction in death at the end of the trial – if there was one, which there often isn’t. But how does a reduction in death relate to life expectancy? Can a figure be established? Well it can, if you take a few more steps.
Below is a simplified graph from the Heart Protection Study (HPs), looking at the survival curves for statin or placebo. At the start everyone is alive, as you would expect. By year five, more people have died in the placebo arm than the statin arm. I think I should mention that this was one of the most positive statin trials ever done. This is me, giving them the benefit of the doubt.
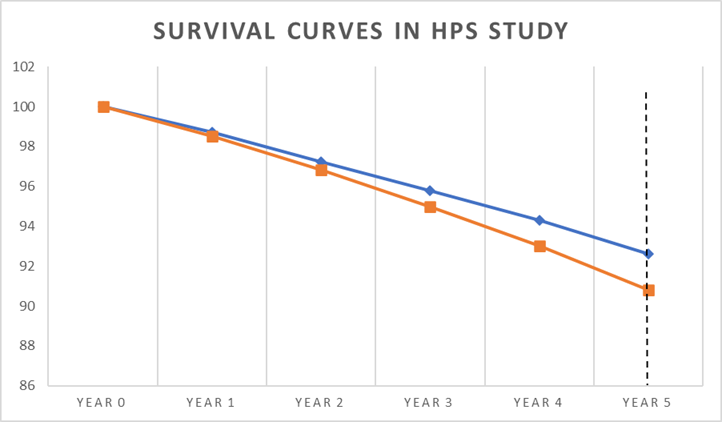
The vertical dotted line at year five represents the end point of the study, where you can see there is a clear difference in the percentage of deaths:
- 90.8% were alive on placebo
- 92.6% were alive on statin (simvastatin)
A difference of 1.8%.
The press release for this trial stated the following:
“In this trial, 10 thousand people were on a statin. If now, an extra 10 million high-risk people worldwide go onto statin treatment, this would save about 50,000 lives each year – that’s a thousand a week.”
Rule number one of medical research, you cannot save lives. Unless you succeed in making people immortal. The most you can possibly achieve is to increase life expectancy…by some amount.
Indeed, ‘life saving’ is a completely non-scientific term that should not be used to describe any clinical study. Although, obviously, it does sound rather good. Fifty thousand lives saved a year has a certain ring to it which, you could argue, 0.2% does not.
Moving on. In the HPS study 1.8% more people were alive after five years. But how much longer, on average, would they live. One day, or forty years? Well, you cannot calculate this precisely, due to the somewhat wobbly nature of survival curves, but you can get close enough.
The first step in doing this, and the most simple, is to draw a horizontal line through the survival curves, rather than using a vertical one at the end. This is effectively what they do, or did, with cancer trials. Although it is a little more scientific than that.
In the diagram below, I have drawn my horizontal line at four years, taking it from the placebo survival curve. If I drew it at five years, I would be drawing a line out into empty space.
After four years, 94.3% were alive in the statin arm, and 93% on placebo. A difference of 1.3%. How long did it take for those in the statin arm to reach the 93% survival point seen in the placebo arm? Well, as you can see from where the arrows are pointing it was less than a year. About nine months, give or take.
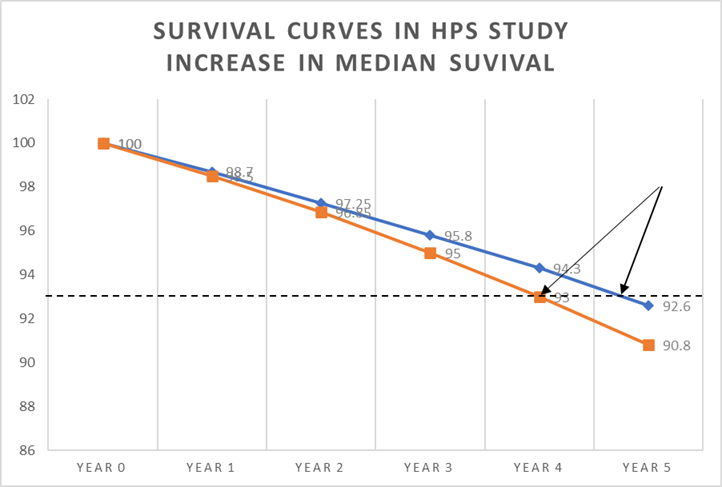
Moving on to the next step, we can now say that, on average, the extra 1.3% who were alive after four years would then live an extra nine months. Which allows us to make the following calculation.
Average increase in life expectancy after four years is nine months (274 days)
But this is not for the entire population, it is only for 1.3% of population.
So, to establish the average life extension for the entire population we need to multiply 274 days by 1.3%
274 x 1.3% = 3.5 days [274 x 0.013 = 3.5].
After five years, it is likely this figure would increase by five fourths. Divide by four and multiply by five.
3.5 days 4 x 5 = 4.4 days
Clearly these figures are not precise, but they are close. If you look at the HPS study in this way it means that if you take a statin for five years, you may expect to live for an extra 4.4 days.
There are other ways to do this calculation, but they all come to pretty much the same conclusion. I once did the calculation using a much more accurate method called Reduction in Mean Survival Time (RMST) where you calculate the area under the curve for the statin and placebo, then look at the difference, then do a bit of mathematics. But I could not get it published anywhere.
One study in the BMJ Open, and the only one to do this, as far as I know, did look at the life expectancy issue, taking data from a number of statin trials. They worked out the increase in life expectancy – if you take a statin for five years – which is how long many of the major statin trials lasted.
The researchers then split the results in two.
- In primary prevention the average life extension was 3.2 days
- In secondary prevention the average life extension was 4.1 days.
Which, as you can see, is pretty close to my simplified calculation. [The HPS study was a secondary prevention trial]. 3
This figure certainly caught the attention of the CTT at Oxford. Their response can be summed up by Professor Colin Baigent in the Mail on Sunday article – the article that I sued them for.
‘…the important thing is statins extend healthy life. They avoid both disabling events like heart attacks and strokes. Simply focusing attention on extra duration of life is to ignore the fact that these drugs reduce disability.’
At first sight this is a valid point. But there are a couple of major issues to consider here. The first is that a ‘non-fatal’ heart attack is not necessarily disabling, in the least. They can pass virtually unnoticed. As do many strokes.
Despite this, in the clinical reporting on statins trials, no distinction is made between a crippling stroke, and one that leaves no trace it ever took place. Same for heart attacks. A stroke is a stroke, a heart attack is a heart attack What about: mild, moderate, severe? Nope, they all get bundled up together under the same heading. Which is clearly, and most probably deliberately, misleading.
However, and more importantly, the Baigent argument is effectively negated by the data I presented in the previous blog. Which is that, while ‘serious cardiovascular events’, such as a stroke, are reduced, other Serious Adverse Events (SAEs) are increased – to the same degree. These can be equally damaging and dangerous.
If cardiovascular serious adverse events are viewed in isolation, 71 primary prevention patients with cardiovascular risk factors have to be treated with a statin for 3 to 5 years to prevent one myocardial infarction or stroke.
This cardiovascular benefit is not reflected in 2 measures of overall health impact, total mortality and total serious adverse events. Therefore, statins have not been shown to provide an overall health benefit in primary prevention trials.’
Their conclusion: unrecognized serious events are increased by statin therapy
This, then, is the lens through which I view the benefits of statins. They do not reduce ‘overall’ serious adverse events, and they increase life expectancy by around eighteen hours… a year.
Adverse effects vs efficacy – the interconnected battle
If you view statins through the lens that I do, then the rate of adverse effects is almost completely irrelevant. Why would anyone put up with any unpleasant effects to achieve such a limited benefit?
In addition, you could easily spend your extra eighteen hours a year getting your cholesterol level checked, picking up the prescription, taking the tablets, waiting to get the prescription filled at the chemist, visiting your doctor. Worrying about your cholesterol level.
Clearly, however, my position is not widely shared. Here are a couple of quotes from the researchers who did the CTT Oxford study on adverse effects.
‘Oxford University researchers said decades of misleading information may have put millions off taking the daily pills. They can slash the risk of heart attacks and strokes by up to half for those at the highest risk.
50% of patients who would benefit from these extraordinary drugs are not receiving them, for whatever reason.’ 4
These ‘extraordinary’ drugs.
Yes, here is the heart of the interconnected battle. Benefits vs. adverse effects. In truth, you can’t really talk about one without paying close attention to the other. If the benefits are great, people will be willing to put up with many more adverse effects, and vice-versa.
Before having read this article you may have wondered how an Oxford researcher can state ‘They (statins) can slash the risk of heart attacks and strokes by up to half.’ Yet, I am on record as saying that statins are really not that great. When you look closely, they increase life expectancy by eighteen hours a year, and that’s about it.
Do we live in a weird parallel Universe? Am I lying; are they lying? Nope, as I hope to have demonstrated, we live in the same universe, we simply choose to frame the data in a different way.
A few years ago I wrote a book called Doctoring Data – which looks at the games played with medical research. I quoted Professor Michael Baum on prostate screening.
‘Every year I play a game with the senior postgraduate students at a course for specialists in cancer run by the Royal College of Surgeons in England. I tell them that there are two potentially effective screening tools for prostate cancer. One of which will reduce their chances of dying from the disease by between 10 and 30 per cent, while the other will save one life after 10,000 years of screening.
As a consumer or as a public health official, which one would you buy into?
They all vote for the first; yet the programmes are the same, they were just packaged differently.’
So, yes, it is scientifically correct to claim a 10 to 30 per cent reduction in prostate cancer deaths from screening. This is not a lie. It is a statistical fact. However, precisely the same data tells us that you can save one life after 10,000 years of screening. Or, to be a pure pedant, delay one death. This is not a lie either, it is a statistical fact.
The pro-statinators claim that statins slash the risk of heart attacks and strokes by up to a half (in truth, this is really pushing it. One study, stopped short, somewhat dodgy gathering of data, but I shall let it pass). I say, take a statin for a year and live eighteen hours longer. We are both right. Or correct, or whatever word fits best here.
It is up to you, I suppose, to decide who you want to listen to. What you wish to believe. What you think is most important.
Perhaps all clinical trials should be mandated to report in the same way, using all possible forms of outcome measurement. Here is a selection that you could include from cardiovascular trials
- Relative reduction in primary outcome e.g. fatal heart attacks
- Absolute reduction in primary outcome e.g. fatal heart attacks
- Relative reduction in overall cardiovascular events, fatal and non-fatal
- Absolute reduction in overall cardiovascular events, fatal and non-fatal
- Reduction in overall mortality, relative and absolute
- Number needed to treat (NNT)
- Number needed to harm (NNH)
- Reduction in composite end points – many different outcomes added together
- Serious adverse events
- Serious cardiovascular adverse events
- Serious non-cardiovascular adverse events
- Drug related events
- Average increase in life expectancy etc. etc. and on and on ….
At present there is no standardised way to report data from a clinical trial. You can present it pretty much any way you want. And, to a great extent, also create any message you want. To quote the paper. ‘How statistical deception created the appearance that statins are safe and effective in primary and secondary prevention of cardiovascular disease.’ 5
- The almost exclusive presentation of data in the relative risk format by statin advocates has intentionally misled the public to exaggerate the miniscule benefits of statins.
- Primary-preventive cholesterol-lowering trials have not succeeded in reducing the rate of mortality.
- The absolute risk reduction of CVD mortality in secondary-preventive cholesterol-lowering trials is quite small, rarely exceeding two percentage points, and no primary-preventive trial has ever succeeded in prolonging the life of the participants.
- The rate of serious adverse effects of statin treatment is highly underestimated.
- Adverse effects of statins are extensive, including diabetes, cognitive impairments, cancer, cataracts and musculoskeletal disorders.
- The small benefit seen in the cholesterol-lowering trials is independent of the degree of cholesterol lowering
Next, and finally on this damned topic. Why the CTT Oxford paper was so horribly misleading. A true masterclass in statistical obfuscation.
* Oncologists and cancer patients generally agree that the primary goals of advanced cancer treatment are to lengthen and/or improve patient survival. Yet over the last two decades, clinical trials of new cancer treatments have moved away from measuring outcomes that matter to patients… Research has shown that when patients are fully informed about the meaning of PFS (progression free survival), about half would not choose additional treatment for any magnitude of gain in PFS in the absence of an overall survival improvement’ 6
1: https://www.nytimes.com/1997/08/10/magazine/the-fall-and-rise-of-kilmer-mccully.html
2: https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2790055
3: https://pubmed.ncbi.nlm.nih.gov/26408281/
4: https://www.express.co.uk/news/uk/2166863/statins-side-effects-new-report

This morning I read https://suavek1.substack.com/p/dr-mike-yeadon-its-funny-not-funny
To which I put a comment:
We are conspiracy theorists. There are conspiracies. Remember that Adam Smith classic: “People of the same trade seldom meet together, even for merriment and diversion, but the conversation ends in a conspiracy against the public, or in some contrivance to raise prices.” We have theories about such. Of course, not all theories will be correct. We can check the theories are honest by using the Popper falsifiability check. For example, I think that the mass prescription of Statins (even to children) is a conspiracy of drug companies to make huge profits (this is not to say that no group of people might benefit). This could be falsified by the Oxford Clinical Trials Unit allowing all the data they analyse to be available for anyone to check rather than keeping it secret. One of the characteristics of conspirators is secrecy. On Covid-19 consider all the data that government agencies have not released in order not to create ‘vaccine hesitancy’.
“Their conclusion: unrecognized serious events are increased by statin therapy“
By unrecognised, do you mean the trial or that the serious events are unrecognised? Furthermore, are saying that it’s the statins that cause these unrecognised serious events, the so-called side effects?
But how do we actually experience living an extra 18 hours a year if we take statins? It doesn’t make sense, in fact, it’s a nonsense statement, that’s not how we live, or die, for that matter, by adding or subtracting hours from our lives based on taking a pill.
I am not sure I understand what you are trying to say? Are you saying that increasing life expectancy is meaningless?
Well 18 hours – how do you quantify it. Okay,I’m 50 years old and I have heart attack and the damage is repaired and otherwise, my health is fine, so assuming I don’t get ill with something else, life threatening, what does the 18 hours mean? Do I simply add it on to my three score and ten? That’s why I say 18 hours is meaningless in real life just as statistics are meaningless in real life, so why bother to quantify it?
Maybe you need something like the weather report e.g. “There is a 30% chance of three millimeters of rain.”
Translated, it means there might be some drizzle, or there might not.
Thanks as ever. Trying to get a relatively to take a statin holiday, he’s got really bad skin issues. Might not be them but…. Linda
Excellent summation. The statin battle is the same as the vaccine battle. Everyone must take them, there can be no questions and the doctors know best (because big pharma trained them that way). Money is the KEY factor. Not health, longer living or anything else.
…”At present there is no standardised way to report data from a clinical trial.”…at least in the case of statins, there were clinical trials whereas for vaccines, the trials remain almost nonexistent never using a true placebo and never lasting more than a few days, weeks or months…never years.
After 4 decades of statins, are there fewer heart attacks, less stenting, less bypasses being done? I doubt it. Heart disease remains the number one cause of death right above cancer where they have failed also to “save lives”.
Statins, vaccines, cancer drugs…they are ALL toxic poisons with risks to the health of a body. These things are not inert. They can cause real damage to prisitine systems. Therefore, in my view, they are to be avoided like the plague they truly are. Sorry, no exceptions.
Having worked on the development of a statin in the late 1990s, I once believed they were the saviour… but despite their use over the last nearly forty years, we haven’t seen a massive decline in the rate of CVD… 1 in 2 of us in the UK will still succumb to some sort of event such as a stroke or heart attack. What I find fascinating is the fact that over all, CVD mortality is broadly similar to cancer deaths…and the great thing about CVD is that many of the risk factors are modifiable – stop smoking, manage your BP, don’t get diabetes (or reverse it if you can), keep your weight in healthy range, and your risks reduce considerably. Of course I could add… track (and manage) your homocysteine, hsCRP etc etc….
My GP and a cardio who saw me twice may well both be wondering how come I’ve been going about happily and well in my statinless state over the past 5 or so years. Possibly they’re expecting imminent death ? Both did their best to have me accept that taking some statin or other would save my life; and both gave up, with differing degrees of irritation.
Thanks, Malcolm. 🙂
On the slightly different but related issue of cardiac failure, what is the risk versus benefit of taking the latest ‘trend’ as per JAMA , 4 drug approach? It is considered the latest best treatment for those with reduced ejection fraction.
At least 2 of these drugs, to my knowledge have not been on the market for very long.
After following you for many years prior to retiring as an a 50 yr veteran of nursing, I am very grateful for your books etc in opening my eyes even further than others have and for the effort you put into enlightening the world.
Dr. Kendrick, thank you! In New Zealand, it is the same story. My wife was prescribed statins. After taking the drugs for some time, she developed muscle pain and dizziness. Her doctor acted very smug, stating that her liver was not damaged (yet) and she needed to accept the pain as part of the course. When she declined to continue with the statins, he gave her a lecture and practically accused her of suicide. He also made a note in her file that she refused treatment. Luckily, our new GP accepts our decision without trying to scare us into taking this horrible drug. Greetings from NZ! PeteC
I wonder how many patients just flush the pills down the loo. Presumably that is unknowable?
Dr. Kendrick, thank you! In New Zealand, it is the same story. After taking the prescribed statins for some time, my wife developed muscle pain and dizziness. Her doctor acted very smug, stating that her liver was not damaged and she needed to accept the pain as part of the course. When she declined to continue with the drug, he gave her a lecture and practically accused her of suicide. He also made a note in her file that she refused treatment. Luckily, our new GP accepts our decision without trying to scare us into taking this horrible medicine.
I think doctors should be reported for, essentially, trying to scare and bully people into taking any drug.
I’m just starting reading your book The Great Cholesterol Con. Got it second hand, so no publishing money( sorry) but the previous owner has underlined many passages. Thanks for daring to point out that the Emperor has no clothes.
Adverse effects are under reported.
Years ago, after being prescribed a statin, I asked my doctor to report my complaints of fatigue and sore muscles to the FDA. She refused, stating outright that, “they already know it”
That experience opened my eyes to see that statin drugs are just one part of the larger fraud that passes for medicine and public health, that includes germ theory, the existence of viruses, contagion, the covid era lockdowns, vaccines and vaccine mandates, fluoridation, and psychiatry to name a few.
Generally speaking, any system can be designed to achieve one specific result. Aiming for two or more separate outcomes is usually unsuccessful.
In theory the purpose of the medical system is to cure the sick and (if possible) keep the healthy that way.
In practice it has become much more oriented to earning money.
Once you understand that, it’s easy to see how in specific situations earning money squeezes out other goals. For instance, patients’ health can usually be improved by providing more, better trained, and more experienced doctors and nurses.
But that costs money, which harms the bottom line.
Many people would benefit far more from enough sleep, exercise, and sun; healthy food and drink; and a reduction of stress. But corporations want to squeeze more work from their employees in return for less payment; so none of those can be provided. Instead, drugs and operations are prescribed – each of which earns a profit.
In short, medicine has ceased to be a useful service to people, and has become a profit centre.
Thank you so much for your continuing work Dr Kendrick. I am eternally grateful firstly you plus your close collegues have saved me from the tyranny of statins. Massive big up for the doc!
Dear Dr. M:
Fabulous discussion. I have my sincere doubts about statins, but am always careful to give the devil his due. You are as well. It ainât much.
Three typos you might want to fix (maybe two – I am an American and so we speak a different language):
Steven C. Root sroot@tds.net
>
A peripheral friend was telling me his doctor told him he had slightly elevated cholesterol and prescribed statins… he is taking them even though he said he googled side effects and discovered that they can cause liver issues… he raised this with his doctor and will have regular tests to ensure his liver is not being damaged…
I mentioned your name and book to him … and suggested he might want to read it… he nodded but did not mark down your name for future reference
The thing is… most humans are barnyard animals.. they have no intelligence… they simply do what they are told by authorities… no questions asked
There is no point in trying to help them … it is a waste of time.
Look after NUMBER ONE. Let the others inject and pop pills and eat KFC for every meal. Who gives a shit
‘‘If you stop taking them, you will have a stroke or heart attack, and die!’
What amazes me is how Homo sapiens has survived for a quarter-million statin-free years.
In the past few years I have become aware of the role of fibrinogen in strokes and blood clotting in general. I did some testing at the advice of a naturopath and found my fibrinogen was quite elevated. The naturopath advised me to lower it in order to reduce the likelihood of cancer recurring, by taking a remedy of protiolytic enzymes. It includes nattokinaze, serrapeptase, pancreatin and lumbrokinase. As a result, my fibrinogen level has dropped to just above the normal range within less than a year. I did some research and found that fibrinogen causes clotting in the blood. Has anyone been advised by their cardiologist to use protiolytic enzymes? What they do is break up misfolded proteins which lead to clots. This may be a simplified explanation, but the evidence is in the pudding. I do not have heart problems but my GP never checked for fibrinogen until I asked for this blood test – I am 75. He now tracks it regularly and thinks that anyone over 55 should be tested for this regularly.
Thank you Dr Kendrick for another brilliant analysis. I’m fortunate I don’t take statins and would certainly be reluctant to do so if advised by my GP.
Your paper was excellent and presented the information in an easy-to-understand manner, to understand exactly what the tests are showing.
Charles Flowers, D.M.D.
I am 59 years old, and for the last 20 years I’ve been living with a total cholesterol of 400mg/dL.
I don’t take statins. I have made eco-dopplers through the years that show completely clean arteries.
I just keep my diet not high on carbs, I eat my salt and healthy fat.
That’s it!
I had an epiphany when I saw this Video, back in2014 of Dr Kendrick. It reassured, me for good, that my fears of the statins were right
https://rosemarycottageclinic.co.uk/blog/2014/10/12/autumn-seminar-2014-post-2-dr-malcolm-kendrick-video-pt1-ten-key-contradictions/
400mg/dl is 10.34 mmol/l, using the units used in most of the rest of the world – other than the US, and a couple of other places. I was in communication with a man from the US, who was 70, who had an LDL level of 18mmol/l. About six times the average level in the UK/US. He, too had perfectly clean arteries and no evidence of CV disease at all.
Yes, I remember you mentioning it on a post.
I read everything that you write; both for the information and your GREAT sense of humour!
In view of some of the things he reads about, Dr Kendrick needs a great sense of humour!
RE: ‘I shall deign to treat you, so long as you do exactly as I command. Look upon my works, ye mighty, and despair.’Seriously…what is going on with voluntary informed consent…particularly the lack thereof?I’ve been investigating this for years in regard to vaccination, where particularly in countries such as the US and Australia, coercive and mandatory vaccination is in force – e.g. for children’s vaccination, and more recently COVID-19 vaccination.It’s extraordinary!!! Are doctors and other practitioners even taught their personal obligation to obtain voluntary informed consent for vaccination?
This is the most important medical ethical principle – voluntary informed consent for vaccination, for statins, for any medical intervention.
When is this going to come under the spotlight? The astonishing fact that people are being press-ganged into medical interventions…and the practitioners actually administering those medical interventions are in the frame for violating consent.
I really enjoy your (too occasional!) posts. However in this case I am not too sure I agree with some of your analysis on increased life expectancy in the HPS study. The second graph suggests that for the first 7% to die in either arm, average survival time was around 4.5 months higher in the statin arm (ie the 9 months gap highlighted divided by 2). For the remaining 93% in both arms there is no information to be able to determine any difference in survival rates (as they have not died yet). To get the complete answer you would need to wait until everyone had actually died. By spreading the the increased life expectancy across the whole population there is an implicit assumption that there is no additional life expectancy for the survivors (which is true after 4 years but not necessarily for the years afterwards)
A relative and I have the same doctor. He’s put both of us on statins. My relative does everything the doctor tells her to, but I read Dr Kendrick and I never took a statin. One day I explained to my relative why I won’t take a statin.
She got a bit worried and went to our doctor and told him she was thinking of stopping statins because of what I said. He replied, “Oh, he’s one of those, is he? Well, my girl, you WILL not get a heart attack on my watch. TAKE YOUR STATINS!”
I like my doctor and he’s occasionally been a big help to me, but I don’t mention statins to him, nor will I ever get a cholesterol test again because I don’t want an argument.
“When I first heard the CTT at Oxford had published their latest analysis on statin adverse effects I must admit I sighed deeply. Do they never give up?”
No – and that is very important! It’s the same with everyone struggling against the powers that be. They don’t give up, because although the individual people resisting them must do so in their copious free time and with their own resources, those who work for the mighty governments and corporations do it as their day job – and get paid for it by the very people whom they are frustrating.
Exactly, that’s the problem, there are no repercussions for the establishment and their attack dogs. They can spend and waste literally billions pushing their false agendas in the knowledge that their corruption will not impact their lifestyles, their pensions or even their reputations.
‘We’, on the other hand, are assumed to be guilty until ‘we’ can prove, at our own cost, our innocence. How did we ever get in this state ?
Briefly put, those who have wound up on top are the ones who set out deliberately to wind up on top. The rest of us just got on with our work and our lives.
As one of my favourite writers put it, it is easy enough to acquire power or wealth if you are competent and that is the only thing you want or are interested in.
But what a ghastly, narrow way to live your life!
The pushback is very evident on social media in last 12 months after truths on many subjects coming to light…..
True; but the “pushback” (us writing comments or even articles) doesn’t inconvenience or stop them in any way.
Dear Dr. Kendrick,
Thank you so much for keeping me motivated by reminding me how much benefit I would get from Statins, so I can continue to keep away from it with a piece of mind and huge sigh of relief.
Dr Kendrick
I had a look at the HPS study and I don’t fully recognize the numbers you have stated above.
“All-cause mortality was significantly reduced (1328 [12·9%] deaths among 10 269 allocated simvastatin versus 1507 [14·7%] among 10 267 allocated placebo; p=0·0003),…”
Survival after 5 year on statins is 87.1% and 85.3% on placebo. The difference is still 1.8% so I don’t think it matters for your argumentation, but please comment on the numbers.
I had a look at the HPS study and I don’t fully recognize the numbers you have stated above.
“All-cause mortality was significantly reduced (1328 [12·9%] deaths among 10 269 allocated simvastatin versus 1507 [14·7%] among 10 267 allocated placebo; p=0·0003),…”
Survival after 5 year on statins is 87.1% and 85.3% on placebo. The difference is still 1.8% so I don’t think it matters for your argumentation, but please comment on the numbers.
I shall have a look, thanks for the comment.
I really like that you point out some of these statistical sleights of hand that are often used to make effects look bigger than they are. I will say though, I work on cancer trials and I have had regulators ask us to measure overall survival as they feel it is a better measure than PFS. This has actually happened on my trials in the EU in particular. In the US they are less concerned with the data presentation as the FDA has its own statistics department so you have to submit your raw data files to them. This does not mean however that the drug won’t be marketed in a deceptive way but it does demonstrate that the regulators are aware of this (at least in oncology) and some are working to prevent the use of less useful endpoints.
I think there needs to be a standardised way to present data – at least to the medical profession. Most doctors, like me, have little ability to understand the statistical models used, nor the statistical tests. I have taught myself a rough understanding of how things are done, but rapidly get lost in the mathematical complexities. I am good a logic, but less good at maths. The main issue is, generally, the assumptions the models are built on. If the assumptions are not valid, or maybe not clinically important e.g. progression free survival in cancer, then the statistical models applied become pointless.
In cardiovascular trials there is increased reliance on combined end-points. Where you add CV mortality to non-fatal MI, to non-fatal stroke to angina requiring hospitalisation to insertion of a stent…etc. But these are not equivalent end points. Deciding to insert a stent is a clinical decision, not a clinical outcome. Counting it in such as way that it carries the same weight as dying of a heart attack is, in my view, completely invalid. Equally, a non-fatal stroke can be highly disabling – long term. Or it can be an episode that last half an hour, leaving no trace it took place. Again, giving these the same weight is, in my view, completely invalid. There is much that is being allowed to slide and someone, somewhere, needs to get a grip on it.
“But these are not equivalent end points.”
Quelle délicatesse.
I might have said “these are obviously crooked manoeuvres by scoundrels”.
I believe there is a way to get to clear and defensible answer on the effectiveness of statins: use data mining tools and ideas.
The basic idea is simple: find a data source from which you can draw outcomes comparisons among people who were prescribed statins and either did, or did, refill the prescriptions over some considerable period. This approach reduces costs, uses historical data, side steps the placebo effect, lets you track the effects of demographics and many drug interactions, and lets you differentiate between drug use based on correct and incorrect diagnoses as determined after death.
To do this you need a data source that records dates, demographics, diagnoses, prescriptions, refills, and the eventual cause of death. Canada probably has this data but I doubt you can get it – and the NHS probably has too but may, I suspect, be equally reluctant to share it.
My suggestion would be Kaiser Pemanante – they have a research group, appropriate data covering hundred of thousands of patients for 30 or more years, and a commercial interest in the result. If you get Kaiser on side this will become, I expect, a team effort with their people handling the data – but if you want help vetting the techi side of the proposal please let me know.
I listen to Mandrola on Pub Med. Intended for clinical professionals, he does a good job in analysing trials including issues about combined end points and what he considers to be pointless trials. He also appears to be cautious about the motivation for trials that may sanction devices that may not support positive clinical outcomes.
I wonder if Dr Kendrick ia aware of this gentlemen’s work and whether he shares his views on clinical trials.
The point about doctors threatening to remove patients from their lists in the US for refusing statins is particularly alarming. It really highlights how this has moved beyond medicine into a form of coercion. That pressure makes an honest discussion about side effects almost impossible.
I received this info after an annual phone review with a Clinical Pharmacist. Interesting to see the other drugs now being pushed on you if you refuse statins.
Bempedoic Acid, Ezetimibe, Inclisiran, Alirocumab and Evolocumab. Maybe to the better informed they’re not so new but they’re new to me. Politely declined the kind offer of statins again. The listed side effects look lovely. Gout (Bempedoic Acid) and the usual stomach upsets headaches etc etc for some of the other alternatives.
How anyone could believe in the cholesterol hypothesis after viewing this video from Dr. Kendrick, published 12 years ago, I do not know. There is so much evidence refuting the hypothesis. I salute Dr. Kendrick for persisting in his efforts to combat disinformation despite the blind indifference or downright hostility from his fellow physicians.
Ten reasons the Cholesterol-Hypothesis is wrong (VIDEO) – Rosemary Cottage Clinic Blog
https://rosemarycottageclinic.co.uk/blog/2014/10/12/autumn-seminar-2014-post-2-dr-malcolm-kendrick-video-pt1-ten-key-contradictions/
How anyone could believe in the cholesterol hypothesis after viewing this video from Dr Kendrick, published 12 years ago, I do not know. There is so much evidence refuting the hypothesis. I salute Dr Kendrick for persisting in his efforts to combat disinformation despite the blind indifference or downright hostility from his fellow physicians.
Ten reasons the Cholesterol-Hypothesis is wrong (VIDEO) – Rosemary Cottage Clinic Blog
https://rosemarycottageclinic.co.uk/blog/2014/10/12/autumn-seminar-2014-post-2-dr-malcolm-kendrick-video-pt1-ten-key-contradictions/
Yes, that video was an epiphany to me. I am a nurse and it changed everything I thought about health
https://www.nytimes.com/2026/04/25/health/eugene-braunwald-dead.html
I’d be curious to hear how much of his work lined up or didn’t with your ideas.
Reading about your friend being told she’d “most likely die” without atorvastatin really struck a nerve. My own mother was given a similar ultimatum, but after she developed severe muscle pain, switching to a different class of drugs actually worked better for her. It makes you wonder how much of that rigid pressure is evidence-based versus just institutional habit.