7th September 2019
In the UK, it has been decided that high intensity statins can now be sold over the counter to people – no prescription required. The European Society of Cardiology has decreed that there is no normal level for cholesterol, the lower the better. It goes on, and on.
However, there are some glimmers of light, occasionally. Aseem Malhotra, and I, wrote a letter to Sir Norman Lamb MP. Chairman of the Science and Technology Select Committee – at his request – asking for a review of statins, and safety issues.
It was reported in the few news outlets that had any space left after Brexit. You can see the video on Sky with Aseem, here
(or here is the link to YouTube… https://www.youtube.com/watch?v=RxCO9iiJYDw)
The letter is below.
Sir Normal Lamb MP
Chairman, Science and Technology Select Committee
29/08/2019
Dear Norman,
Re: The need for an independent reappraisal of the effects of statins
Statins are the most widely prescribed class of drugs in the UK.[1] They were designed to lower the blood cholesterol (LDL) level and therefore prevent cardiovascular disease.
Publications based on clinical trials have reported reductions in cardiovascular disease in people at high and low risk, and also a very low rate of side effects (drug-related adverse events).
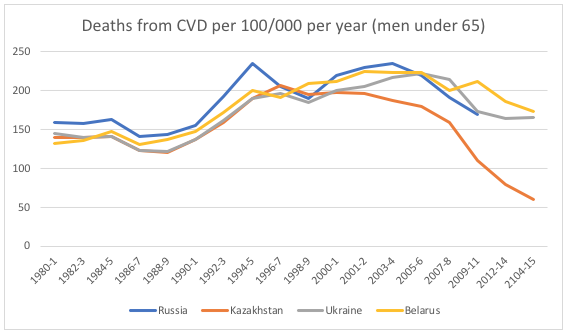
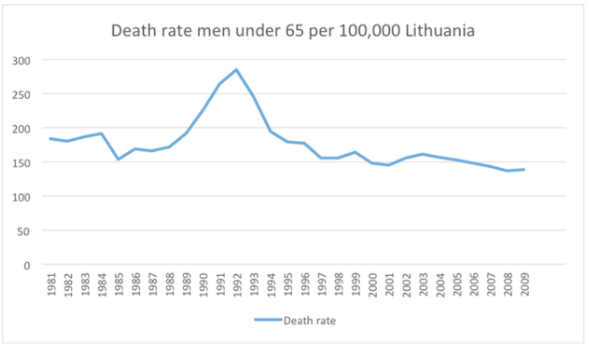
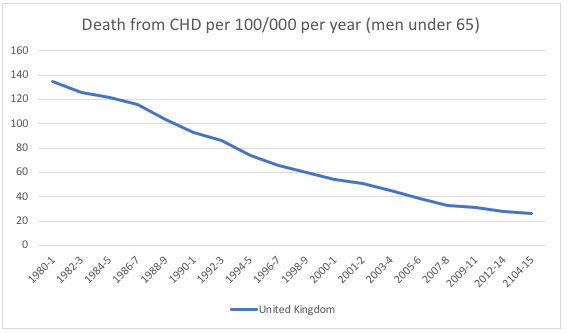
It has been widely claimed that statins have therefore been responsible for the considerable reduction in the cardiovascular disease seen over the past 30 years both in the UK and the rest of the Western World,[2] but there is evidence that refutes this claim. An ecological study using national databases of dispensed medicines and mortality rates, published in 2015, concluded: ‘Among the Western European countries studied, the large increase in statin utilisation between 2000 and 2012 was not associated with CHD mortality, nor with its rate of change over the years.[3] In the UK, despite far greater statin prescribing, the rate of cardiovascular disease has been rising for the past four years.[4]
In the absence of an analysis of the clinical trial data carried out by an independent group with full access to the raw data in the form of “clinical study reports”, there is good reason to believe that the benefits of statins have been ‘overhyped’ especially in those at low risk of cardiovascular disease, and the potential harms downplayed, unpublished, or uncollected.
Positive spin on the benefits of statins
It is well recognised that ‘positive spin’ is used to ‘hype’ the results from clinical trials. This should not happen but is widespread. According to one review: ‘Clinical researchers are obligated to present results objectively and accurately to ensure readers are not misled. In studies in which primary end points are not statistically significant, placing a spin, defined as the manipulation of language to potentially mislead readers from the likely truth of the results, can distract the reader and lead to misinterpretation and misapplication of the findings.’[5]
The authors continued: ‘This study suggests that in reports of cardiovascular RCTs with statistically nonsignificant primary outcomes, investigators often manipulate the language of the report to detract from the neutral primary outcomes. To best apply evidence to patient care, consumers of cardiovascular research should be aware that peer review does not always preclude the use of misleading language in scientific articles.’ [5]
As one example of such positive spin in relation to statins, the lead author of the JUPITER trial, Paul Ridker, writing in a commentary in the journal Circulation, summarised apparently statistically significant benefits between statin and placebo:
‘The JUPITER trial was stopped early at the recommendation of its Independent Data and Safety Monitoring Board after a median follow-up of 1.9 years (maximum follow-up 5 years) because of a 44% reduction in the trial primary end point of all vascular events (P<0.00001), a 54% reduction in myocardial infarction (P=0.0002), a 48% reduction in stroke (P=0.002), a 46% reduction in need for arterial revascularization (P<0.001), and a 20% reduction in all cause mortality (P=0.02).’ [6]
Picking up on these figures, another well-known cardiologist wrote in equally positive terms: ‘Data from the 2008 JUPITER Trial suggest a 54 percent heart attack risk reduction and a 48 percent stroke risk reduction in people at risk for heart disease who used statins as preventive medicine. I don’t think anyone doubts statins save lives.’[7]
In fact in the JUPITER trial there was no statistically significant difference in deaths from cardiovascular disease among those taking rosuvastatin compared with placebo. There were 12 deaths from stroke and myocardial infarction in both groups among those receiving placebo, exactly the same number as in the rosuvastatin arm.[8] So the results of this clinical trial do not support claims that statins save lives from cardiovascular disease. This dissonance between the actual results of statin trials and the way they are reported is widespread.[9]
Other studies, looking at whether statins increase in life expectancy have found that, in high risk patients, they may extend life by approximately four days, after five years of treatment.[10] Doubts have also been raised about the claims of benefit in otherwise healthy people aged over 75, in whom statins are now being actively promoted.[11]
An overview of systematic reviews that examined the benefits of statins using only data from patients at low risk of cardiovascular disease found that those taking statins had fewer events than those not taking statins. However, when the results were stratified by the patients’ baseline risk, there was no statistically significant benefit for the majority of outcomes.[12] In conclusion, the absolute benefits in people at low risk are relatively small. If the 2016 guidelines are implemented in full, large numbers of otherwise healthy people will be offered statins, it has been estimated that 400 will need to take statins for five years to prevent one person from suffering a cardiovascular event.[13]
This information is not routinely given to patients, or indeed doctors who prescribe statins, and both doctors and patients therefore tend to have false expectations of the benefits of statins. Clinical guidelines call for shared decision making, including informing patients of the actual likelihood of benefits and risks, but this rarely occurs. There are also obvious questions in relation to value-for-money and the efficient use of finite healthcare budgets.
Side effects/adverse effects underplayed
There has been a heated debate about the adverse effects of statins. On one side, it is claimed that the rate of adverse effects is extremely low, affecting fewer than one in a thousand people.[14] Other studies have suggested adverse events are common, with up to 45% of people reporting problems.[15]
Attempts to resolve this important controversy have been hampered by the fact that the data on adverse effects reported in the clinical trials are not available for scrutiny by independent researchers. The data from the major trials of statins are held by the Cholesterol Treatment Triallists Collaboration (CTT) in Oxford and they have agreed amongst themselves not to allow access by anyone else.[16] Many groups, have called for access to these data, but so far, this has not been granted.[17]
It is not even clear whether the CTT themselves have all the adverse effect data, since the relevant Cochrane Review Group does not seem to have had access to them. According to Professor Harriet Rosenberg of the Health and Society Program at York University: “It’s not clear if the AE (adverse events) data was withheld from the Cochrane reviewers (by CTT) or were not collected in the original trials.”[18]
When asked the lead author of the Cochrane review, Dr Shah Ebrahim, the CTT did not have the data. “Full disclosure of all the adverse events by type and allocation from the RCTs is now really needed, as the CTT does not seem to have these data.”[18]
Release of the data would undoubtedly help answer the question on how and whether the trials collected data on the most common side effects of muscle pain, weakness or cramps.
Summary
Rather than mass prescription based on incomplete and selective information, patients and the public deserve an objective account so that individuals can make their own informed decisions.
We believe there is now an urgent need for a full independent parliamentary investigation into statins:
- a class of drug prescribed to millions in the UK and tens of millions across the world.
- which, based on the publications available, have had their benefits subjected to significant positive spin, especially among people at low risk of cardiovascular disease, and their potential adverse effects downplayed
- where independence would mean review of the complete trial data by experts with no ties to industry and who have not previously undertaken or meta-analysed clinical trials of statins.
Among the signatories to this letter, there are a range of views: some of us are deeply sceptical of the benefits of statins, others are neutral or agnostic. But all are strongly of the view that such confusion, doubt and lack of transparency about the effects of a class of drug that is so widely prescribed is truly shocking and must be a matter of major public concern.
Yours Sincerely,
Dr Aseem Malhotra, NHS Consultant Cardiologist and Visiting Professor of Evidence Based Medicine, Bahiana School of Medicine and Public Health, Salvador, Brazil.
Dr John Abramson, Lecturer, Department of Healthcare Policy, Harvard Medical School
Dr JS Bamrah CBE, Chairman, British Association of Physicians of Indian Origin.
Dr Kailash Chand OBE, Honorary Vice President of the British Medical Association (signing in a personal capacity)
Professor Luis Correia, Cardiologist, Director of the Centre of Evidence Based Medicine, Bahiana School of Medicine and Public Health, Salvador Brazil. Editor in Chief, The Journal of Evidence Based Healthcare
Dr Michel De-Lorgeril, Cardiologist, TIMC-IMAG, School of Medicine, University of Grenoble-Alpes, Grenoble, France.
Dr David Diamond, Cardiovascular Research Scientist, Department of Molecular Pharmacology and Physiology, University of South Florida, Tampa, Florida, USA
Dr Jason Fung, Nephrologist and Chief of the Department of Medicine, The Scarborough Hospital, Toronto, Canada and Editor in Chief of the Journal of Insulin Resistance.
Dr Fiona Godlee, Editor in Chief, The BMJ
Dr Malcolm Kendrick, General Practitioner
Dr Campbell Murdoch, General Practitioner, NHS England Sustainable Improvement Team, Clinical Adviser
Professor Rita Redberg, Cardiologist, University of California, San-Francisco.
Professor Sherif Sultan, President, International Vascular Society
Sir Richard Thompson, Past President, The Royal College of Physicians
Professor Shahriar Zehtabchi, Editor in Chief, TheNNT.com, and Professor and Vice Chairman for Scientific Affairs Research, SUNY Downstate Health Science University, Brooklyn, New York
1: https://www.bhf.org.uk/informationsupport/treatments/statins
2: https://www.sciencedirect.com/science/article/pii/S1933287415004493
3: https://bmjopen.bmj.com/content/6/3/e010500
5: https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2732330
6: https://www.ahajournals.org/doi/full/10.1161/CIRCOUTCOMES.109.868299
7: https://utswmed.org/medblog/statins-debate/
8: https://www.nejm.org/doi/full/10.1056/NEJMoa0807646
10: https://bmjopen.bmj.com/content/5/9/e007118
- Armitage J, Baigent C, Barnes E, Betteridge DJ, Blackwell L, Blazing M, et al. Efficacy and safety of statin therapy in older people: a meta-analysis of individual participant data from 28 randomised controlled trials. The Lancet. 2019;393(10170):407-15.
- Byrne P, Cullinan J, Smith A, Smith SM. Statins for the primary prevention of cardiovascular disease: an overview of systematic reviews. BMJ Open. 2019; 9(4):[e023085 p.]. Available from: https://bmjopen.bmj.com/content/bmjopen/9/4/e023085.full.pdf.
- Byrne P, Cullinan J, Gillespie P, Perera R, Smith SM. Statins for primary prevention of cardiovascular disease: modelling guidelines and patient preferences based on an Irish cohort. Br J Gen Pract. 2019. Available from: https://doi.org/10.3399/bjgp19X702701.
14: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(16)31357-5/fulltext
15: https://www.lipid.org/nla/usage-survey
16: https://www.ctsu.ox.ac.uk/research/ctt
17: https://www.bmj.com/campaign/statins-open-data
18: http://healthinsightuk.org/2015/02/19/keep-statin-supremo-away-from-the-missing-side-effect-data/
Will this have any impact, on anything. We must keep bashing away, until the nonsense about cholesterol – has gone.