
Lose weight, reduce the risk of CV disease – unless you are taking Wegovy?
[A tale of mystery and intrigue unfolds].
A lot of people have asked me about the weight loss drugs known as glucagon-like peptide-1 receptor agonists (GLP-1 agonists) e.g. Wegovy (semaglutide), or Mounjaro (tirzepatide). What do I think of them, are they any good? Should we be worried about adverse effects? Is it a good idea to take them?
Up to now I have rather stood on the sidelines, watching as these drugs have taken over the world. Various friends and colleagues have shrunk before my very eyes. Money has most certainly been made – in eye-watering amounts.
My general view, before having reviewed at the research in any great detail, is that GLP-1 agonists are certainly effective for weight loss. They also have benefits for the ‘metabolic syndrome.’ Sometimes called pre-diabetes, or insulin resistance, or … it has had many names. Reaven’s syndrome, syndrome X. It will probably have a few more in the future.
Metabolic syndrome is, essentially, a derangement of the metabolism which results in a whole set of abnormalities. The most mentioned ones include:
- Raised insulin levels
- Raised blood glucose levels
- Raised blood pressure
- High VLDL (triglycerides)
- Low HDL (a.k.a. ‘good’ cholesterol – hollow laugh)
- Central/abdominal obesity
- Fatty liver (non-alcoholic fatty liver disease – it now has a different name).
They are all bad news. Each one is associated with an increased risk of cardiovascular disease … to a greater or lesser degree. If a drug can improve metabolic syndrome, you would certainly expect to see a reduction in strokes, heart attacks and other cardiovascular related disorders.
How significant a reduction? I have no idea. But if people want to lose weight, for whatever reason, and various other factors improve at the same time, then what’s not to like? Apart from problems with the gall bladder and also, it seems, the pancreas.
In reality, the main ‘what’s not to like’, is the cost. In the UK Wegovy, at whatever dose, costs £73.25 per injection, per week. The other GLP-1 agonists cost much the same 1.
Cost per person, per year = £3,809. Prescribe that for a million people and we are looking at £3,809,000,000.00p per year (£3.8Bn). Which represents two per cent of the entire NHS budget. And this would pay for ninety thousand nurses per year – for example.
On top of this, there is a dispensing fee of £1.46 – per month. Which would end up costing the NHS another seventy-five million a year. [A mere one thousand six hundred nurses]. I am not sure if I should continue to use nurses as a method of currency.
Senior NHS manager: ‘That’s going to cost me five and a half nurses, are you mad…’
Nurse: ‘I am not just a number…’
There is a reason for my one million figure. It was not plucked from thin air. Which is that the new NICE recommendations mean an extra 1.2 million people are now eligible for Wegovy on the NHS – rather than buying it themselves. Potential cost £4.5Bn/year.
Recent NICE guidance (National Institute for Health and Care Excellence) 2
I must say that my relative disinterest in Wegovy (semaglutide) changed when NICE recommended that it should now be offered to: ‘People who have had a heart attack, stroke, or serious circulation problem in their legs, and who also carry excess weight.’ Excess weight defined as a BMI above twenty-seven. This recommendation came about because:
‘Evidence from a clinical trial shows the injection reduces the risk of a heart attack, stroke, or cardiovascular death. Importantly, this benefit was seen early in the clinical trial, before significant weight loss occurred, suggesting the drug works directly on the heart and blood vessels, not just through weight loss.’
Suggesting … a word that does a lot of heavy lifting in this, and many other clinical trials. ‘Suggesting’ is both vague, and yet strangely powerful. Hinting at great mysterious powers, without the need for any evidence, or even a mode of action. Or, it seems, any further research on the matter.
In this case, it also shoves a significant problem under the carpet. How can Wegovy show benefit on cardiovascular disease … before weight loss occurs? It is widely believed that weight loss itself causes the improvement in metabolic syndrome. Followed by improvement in CV disease. But …
Below is a graph from, ‘a clinical trial’. The one NICE use to make its recommendation. It was called SELECT by the way.3 The graph demonstrates weight loss on placebo, and also weight loss on Wegovy, and the relationship with major adverse cardiovascular events (MACE). CV disease to you and me.
There are four lines. Those who lost more than 5% of their weight, and those who lost less than 5% of their weight – for both placebo and Wegovy. I found it extremely puzzling, and I do like a puzzle.
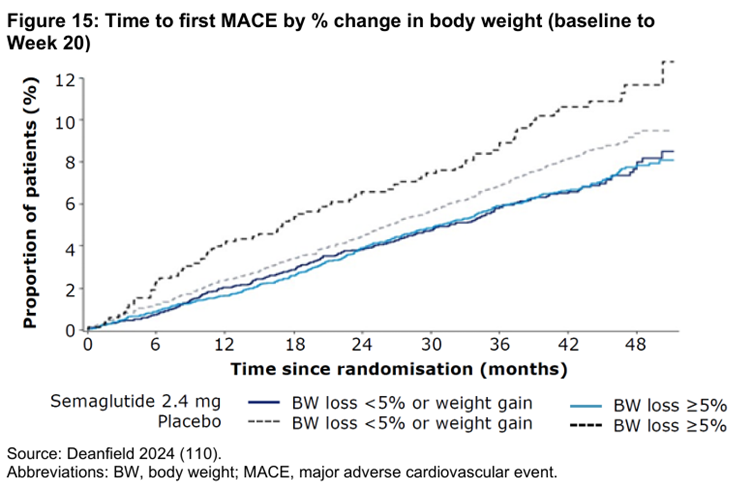
What this graph shows is two things.
- On placebo, the more weight you lose the greater your risk of CV disease – top two dotted lines
- On Wegovy, the degree of weight loss was not associated with CV disease, at all – bottom two lines, that look stuck together.
Now that is interesting. Well, it interested me. To quote Isaac Asimov, the most exciting phrase in science is not “Eureka!” but “That’s funny …” Unexpected findings are the most exciting scientific discoveries of all.
I did write to one of the authors of paper about this, and other issues. The response to the specific question on MACE, and weight loss on placebo was:
‘The relationship between weight loss magnitude and CV benefit is indeed quite complicated, with adiposity changes likely only mediating a minority of CV benefit.’
Quite complicated? The researchers did not start off this study thinking that obesity would have zero effect on CV disease – or that you might even be looking at a reverse effect. As the paper itself states in the introduction, which sort of covers the rationale for the study.:
‘Overweight and obesity are independently associated with an increased risk of cardiovascular events…
And:
‘… the concept of treating obesity to reduce the risk of cardiovascular complications has been hampered by the lack of evidence from trials indicating that lifestyle or pharmacologic interventions for overweight or obesity improve cardiovascular outcomes.’
In other words, they set out to discover if reducing ‘obesity’ would improve cardiovascular outcomes – in isolation. In effect, this was what they were trying to prove. You could argue they managed to prove the exact opposite.
The problem they were faced with
At this point everyone involved with this trial had just run into a tricky problem. I am certain they wanted to say, something like … “Wegovy reduced weight by around fifteen per cent – on average. And this reduction in weight led to the expected reduction in the risk of cardiovascular disease.” Nice and simple, and reinforcing what everyone thought they already knew.
But the evidence, at first sight, and probably at second sight, contradicted their argument … terms and conditions apply. With Wegovy, weight loss and risk were unrelated. By which I mean that greater weight loss had no effect on CV outcomes. However, with placebo, greater weight loss increased CV risk. The plot thickens.
Now, I have known for many years that a BMI of around twenty-seven is associated with the lowest mortality rate – in the majority of studies. I wrote about it this in my book Doctoring Data, which caused a few people to explode in disbelief, and anger. How very dare I use facts to contradict things they know to be correct.
Just to check this hadn’t changed recently I asked Google AI and got this answer:
‘Recent studies suggest that in modern cohorts (2003–2013), a Body Mass Index (BMI) of 27.0 is associated with the lowest all-cause mortality risk, shifting upward from the previously accepted optimal range of 23–24. This range, often classified as “overweight” (25–29.9), showed the lowest mortality rate, suggesting a shift in what is considered the healthiest weight.’
Despite this, a BMI of 27 is still defined as overweight, and thus unhealthy. I think this will never change. At least not in my lifetime. To quote Google AI again.
While some data points to 27 as optimal, conventional guidelines from the World Health Organization and other groups still technically recommend a “healthy” BMI range of 18.5–24.9.
Some data? They actually mean, the overwhelming majority of data. ‘Don’t confuse me with facts – my mind it already made up.’ I also like the use of the phrase technically recommend…. Which means what? Ah, I do love a weasel word or two, used to muddy the waters. You either recommend something, or you don’t. Or to be a little more assertive, you shut up.
So, could this study have simply proved that if you lower the BMI below twenty-seven, the mortality rate goes up? As per the data on obesity. That is, of course, a possible answer. However, it was not an answer that anyone wished to contemplate.
New sales pitch for Wegovy: ‘Please don’t try to lower your BMI below 27, or you are more likely to die.’
I can’t see that going down a storm with the Novo Nordisk board of directors. Half your market gone, overnight.
In truth, after looking at this graph for about two seconds, I knew exactly and precisely what was going to happen. The form of words that would be used, and why. Not because I am a super-genius. Simply because I have seen an almost identical anomaly before. And the tactics brought to bear in order to dismiss it.
Reverse/inverse causality.
I do love causality. And I especially love it when you turn causality upside down and inside out, then stomp it to death. It happened many years ago with LDL cholesterol. To quote Google AI again – because it is very good at summarizing stuff like this, and saves me the effort of thinking what to write:
‘Reverse causality regarding LDL cholesterol occurs when an underlying disease (like cancer, infection, or malnutrition) lowers a patient’s LDL-C levels, creating a false appearance that low LDL causes the illness, rather than the disease, causing low LDL. While high LDL-C is a validated risk factor for cardiovascular disease, very low LDL-C levels in some epidemiological studies correlate with higher all-cause mortality, often attributed to this hidden disease process rather than a causal effect of low cholesterol.’
It’s a seductive argument and widely believed. In simplest form it goes like this. The reason why people (over about 65) with low LDL are more likely to die is because they have an underlying ‘hidden’ disease which both lowers the LDL and also kills them.
Huzzah, the low LDL is not a problem – how could it possibly be, when we absolutely know high LDL is dangerous and must be lowered to the greatest degree possible. Phew. Hidden diseases are, of course, remarkably convenient for this argument. After all, you can hardly be expected to demonstrate a disease that is hidden, can you? It is ‘The cat who wasn’t there.’
When I say that this explanation is widely believed, I mean it is universally believed. And with the greatest fervour by those whose interests it best serves so to do. A few of us looked at this issue a few years back in our paper: Lack of an association or an inverse association between low-density-lipoprotein cholesterol and mortality in the elderly: a systematic review.’4
Our findings:
‘A common argument to explain why low lipid values are associated with an increased mortality is inverse causation, meaning that serious diseases cause low cholesterol. However, this is not a likely explanation, because in five of the studies in (table 1) terminal disease and mortality during the first years of observation were excluded. In spite of that, three of them showed that the highest mortality was seen among those with the lowest initial LDL-C with statistical significance.’
People believe what they want I suppose. The reverse causality argument is essentially a defense created to discount an extremely significant contradiction to the LDL hypothesis. Lift that carpet and sweep … problem gone. ‘Lump, under the carpet … I think you are seriously mistaken young man.’
Thus, it came as no surprise to me to find that that the exact same argument was going to be used to explain away the data from the SELECT trial. The explanation I received from one of the authors was that:
‘The highest MACE [major cardiovascular adverse events] rate in the placebo patients losing the most weight likely relates to underlying comorbidities associated with weight loss.’
Yup, it’s the old reverse causality argument again. Care to say what these underlying comorbidities might be? Did you look for them, did you find them … Ah, no. Despite my scepticism, the reverse causality argument could still be true, maybe, perhaps – benefit of doubt given.
However, as the SELECT trial was randomized you would expect to see the same number of people with ‘underlying co-morbidities’ driving their ‘increased co-morbidity related weight loss’ in the Wegovy arm. But you didn’t, Here, weight loss and CV risk were locked together.
What is going on? This quote from the GP Magazine Pulse nicely summarizes the next immunizing tactic.
‘Presenting the evidence to NICE, pharmaceutical company Novo Nordisk said the cardiovascular benefit was seen early in the clinical trial, before significant weight loss occurred. 5’
The press releases made the general statement(s) that:
‘Evidence suggested the reduction in cardiovascular risk was observed before significant weight loss occurred, indicating that semaglutide may act directly on the heart and blood vessels.’
Aha, Wegovyis protecting against CV risk via a direct effect on blood vessels. So, we can entirely ignore the entire weight loss argument? Phew, move on. Throw in a few words such as likely, and may and suggests, and even suggesting and … problem solved.
I suppose this direct effect could exist. However, I think we should always be suspicious of made up, ad-hoc, hypotheses created for the sole purpose of sweeping aside findings you don’t like. Findings which just contradicted your rationale for doing the trial in the first place. And could seriously question the entire premise behind weight reduction, at the same time.
Final anomaly – for now
In truth, I don’t mind unexpected findings in clinical trials. In fact, I welcome them. They open channels for new thinking. However, I do not like to see anomalies brushed aside and forgotten about. In the graph below, you can see a major problem for the ‘underlying diseases’ argument. Also, the ‘Wegovy provided direct protection’ argument.
DEATH FROM CARDIOVASCULAR DISEASES
[over 48 months]
Grey line placebo, orange line Wegovy
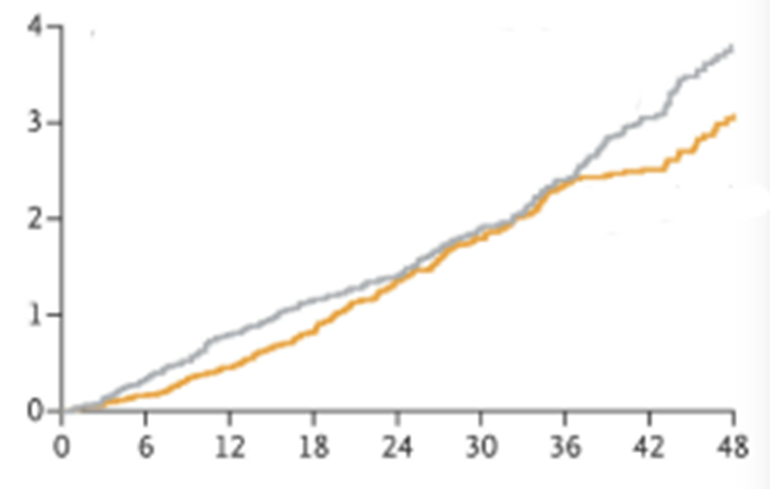
Everyone in this trial had established CV disease, in some cases it was quite severe. In addition, the majority of those who died in this trial, died from a CV disease. You could argue [and I would], that any ‘hidden’ underlying disease would likely be cardiovascular in origin. Which would lead to an increased death rate from CV disease.
Now it is true that, at end of the trial, there were more CV deaths in the placebo arm. However, as you may have noticed, there is a strange phenomenon which lasts from about two years to three and a half years. Here, the mortality graphs converge before separating again.
If someone has an underlying disease that both lowers their weight and causes them to die …It seems highly unlikely that you would have to wait three and a half years for this effect to show up.
Furthermore, if Wegovy ‘may act directly on the heart and blood vessels,’ then why did benefits on cardiovascular death disappear for eighteen months, before reappearing again.
So what?
Yes, I have raised a number of issues here. Why?
First, I think this trial produced some fascinating results. None of which have been explored in the popular press, or the medical press. Or in the NICE report. Or, in fact, anywhere – that I have seen. The message has remained simple, and unchanging. Wegovy reduces weight and reduces the risk of cardiovascular death. Good job, message ends.
But the sky darkens with black swans, and there are anomalies flying all over the place. The arguments used to sweep them aside do not stack up. Primarily, reverse causality, and direct effects on heart and blood vessels.
So what… does it really matter. Wegovy does exactly what it says on the tin. It reduces weight, it reduces CV risk. [Although that risk reduction does disappear for a considerable amount of time, before reappearing which … well, you know]. That may be all we need to be told. It is certainly all you are ever going to be told. Don’t muddy the waters with the actual findings.
However, when I see anomalies, and hastily created ad-hoc hypothesis that exist only to explain things away, it does stimulate me to look deeper, and deeper. Because, to me, these represent warning signs that all is not well in the state of Denmark.
Are other important issues also being shoved under the carpet. What issues, and why? I will have a look at them next. In so far as this is possible. I say this because almost all the important data in the NICE report have been redacted and thus rather difficult to critique.
Here, from page 74.
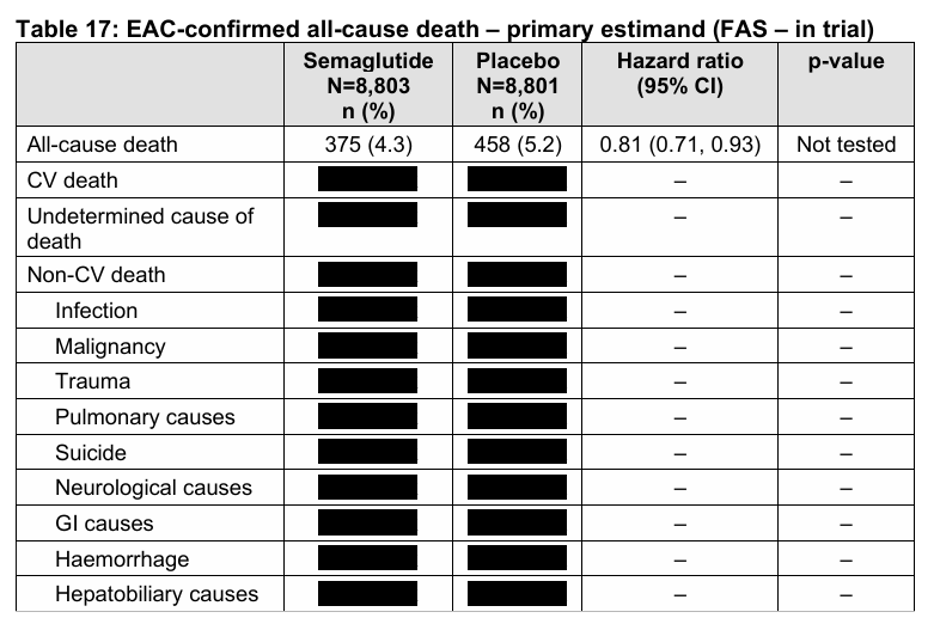
No, you can’t scrape off the little black stickers to see what lies underneath. Commercially sensitive data, dontcha know. Why should we, the public, who fund NICE and who will pay for every single NHS prescription written for Wegovy, be allowed to see such things as … what it actually does. Our poor little brains would probably explode, or something.
1: https://bnf.nice.org.uk/drugs/semaglutide/medicinal-forms/
2: https://www.nice.org.uk/guidance/TA1152
3: https://www.nejm.org/doi/full/10.1056/NEJMoa2307563 It

Could there not be a selection bias operating here? Might people who go to the trouble of taking Wegovy not be the kind of people who would take better care of themselves e.g. exercising more than people who don’t? And therefore having fewer cardio events? Akin to the healthy vaccinee effect.
At all events it is a national scandal that these drugs are being unleashed on the public without the fullest possible independent research done on side effects, and that it is left to individuals like Malcolm to have to point this up.
A great article and reason enough, if reason were needed, not to rush into weight loss drug ‘therapy’. The ‘clot’ does indeed thicken. Having already been prescribed Atorvastatin, Metformin and a plethora of other drugs, I started the Total Diet Replacement (TDR) program for remission of diabetes on 22 April and have already lost 10kg. I will stick with it but might consider easing up when my BMI reaches exactly 27…
But seriously folks, why redact the data from a published report? Are they trying to hide something? Surely not!