
Lose weight, reduce the risk of CV disease – unless you are taking Wegovy?
[A tale of mystery and intrigue unfolds].
A lot of people have asked me about the weight loss drugs known as glucagon-like peptide-1 receptor agonists (GLP-1 agonists) e.g. Wegovy (semaglutide), or Mounjaro (tirzepatide). What do I think of them, are they any good? Should we be worried about adverse effects? Is it a good idea to take them?
Up to now I have rather stood on the sidelines, watching as these drugs have taken over the world. Various friends and colleagues have shrunk before my very eyes. Money has most certainly been made – in eye-watering amounts.
My general view, before having reviewed at the research in any great detail, is that GLP-1 agonists are certainly effective for weight loss. They also have benefits for the ‘metabolic syndrome.’ Sometimes called pre-diabetes, or insulin resistance, or … it has had many names. Reaven’s syndrome, syndrome X. It will probably have a few more in the future.
Metabolic syndrome is, essentially, a derangement of the metabolism which results in a whole set of abnormalities. The most mentioned ones include:
- Raised insulin levels
- Raised blood glucose levels
- Raised blood pressure
- High VLDL (triglycerides)
- Low HDL (a.k.a. ‘good’ cholesterol – hollow laugh)
- Central/abdominal obesity
- Fatty liver (non-alcoholic fatty liver disease – it now has a different name).
They are all bad news. Each one is associated with an increased risk of cardiovascular disease … to a greater or lesser degree. If a drug can improve metabolic syndrome, you would certainly expect to see a reduction in strokes, heart attacks and other cardiovascular related disorders.
How significant a reduction? I have no idea. But if people want to lose weight, for whatever reason, and various other factors improve at the same time, then what’s not to like? Apart from problems with the gall bladder and also, it seems, the pancreas.
In reality, the main ‘what’s not to like’, is the cost. In the UK Wegovy, at whatever dose, costs £73.25 per injection, per week. The other GLP-1 agonists cost much the same 1.
Cost per person, per year = £3,809. Prescribe that for a million people and we are looking at £3,809,000,000.00p per year (£3.8Bn). Which represents two per cent of the entire NHS budget. And this would pay for ninety thousand nurses per year – for example.
On top of this, there is a dispensing fee of £1.46 – per month. Which would end up costing the NHS another seventy-five million a year. [A mere one thousand six hundred nurses]. I am not sure if I should continue to use nurses as a method of currency.
Senior NHS manager: ‘That’s going to cost me five and a half nurses, are you mad…’
Nurse: ‘I am not just a number…’
There is a reason for my one million figure. It was not plucked from thin air. Which is that the new NICE recommendations mean an extra 1.2 million people are now eligible for Wegovy on the NHS – rather than buying it themselves. Potential cost £4.5Bn/year.
Recent NICE guidance (National Institute for Health and Care Excellence) 2
I must say that my relative disinterest in Wegovy (semaglutide) changed when NICE recommended that it should now be offered to: ‘People who have had a heart attack, stroke, or serious circulation problem in their legs, and who also carry excess weight.’ Excess weight defined as a BMI above twenty-seven. This recommendation came about because:
‘Evidence from a clinical trial shows the injection reduces the risk of a heart attack, stroke, or cardiovascular death. Importantly, this benefit was seen early in the clinical trial, before significant weight loss occurred, suggesting the drug works directly on the heart and blood vessels, not just through weight loss.’
Suggesting … a word that does a lot of heavy lifting in this, and many other clinical trials. ‘Suggesting’ is both vague, and yet strangely powerful. Hinting at great mysterious powers, without the need for any evidence, or even a mode of action. Or, it seems, any further research on the matter.
In this case, it also shoves a significant problem under the carpet. How can Wegovy show benefit on cardiovascular disease … before weight loss occurs? It is widely believed that weight loss itself causes the improvement in metabolic syndrome. Followed by improvement in CV disease. But …
Below is a graph from, ‘a clinical trial’. The one NICE use to make its recommendation. It was called SELECT by the way.3 The graph demonstrates weight loss on placebo, and also weight loss on Wegovy, and the relationship with major adverse cardiovascular events (MACE). CV disease to you and me.
There are four lines. Those who lost more than 5% of their weight, and those who lost less than 5% of their weight – for both placebo and Wegovy. I found it extremely puzzling, and I do like a puzzle.
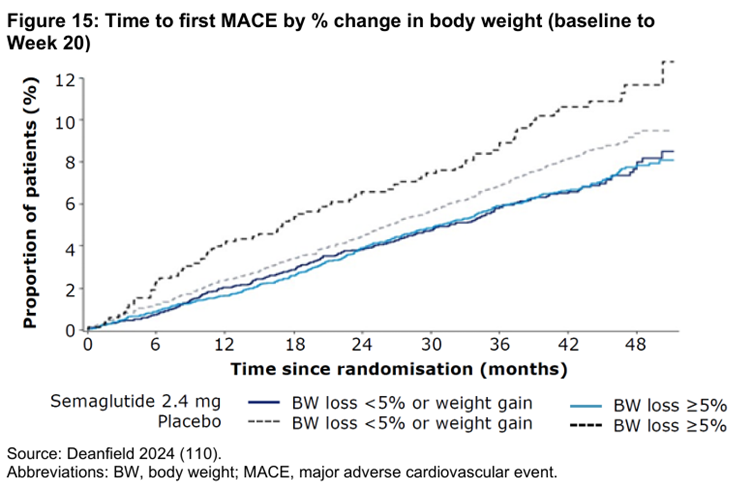
What this graph shows is two things.
- On placebo, the more weight you lose the greater your risk of CV disease – top two dotted lines
- On Wegovy, the degree of weight loss was not associated with CV disease, at all – bottom two lines, that look stuck together.
Now that is interesting. Well, it interested me. To quote Isaac Asimov, the most exciting phrase in science is not “Eureka!” but “That’s funny …” Unexpected findings are the most exciting scientific discoveries of all.
I did write to one of the authors of paper about this, and other issues. The response to the specific question on MACE, and weight loss on placebo was:
‘The relationship between weight loss magnitude and CV benefit is indeed quite complicated, with adiposity changes likely only mediating a minority of CV benefit.’
Quite complicated? The researchers did not start off this study thinking that obesity would have zero effect on CV disease – or that you might even be looking at a reverse effect. As the paper itself states in the introduction, which sort of covers the rationale for the study.:
‘Overweight and obesity are independently associated with an increased risk of cardiovascular events…
And:
‘… the concept of treating obesity to reduce the risk of cardiovascular complications has been hampered by the lack of evidence from trials indicating that lifestyle or pharmacologic interventions for overweight or obesity improve cardiovascular outcomes.’
In other words, they set out to discover if reducing ‘obesity’ would improve cardiovascular outcomes – in isolation. In effect, this was what they were trying to prove. You could argue they managed to prove the exact opposite.
The problem they were faced with
At this point everyone involved with this trial had just run into a tricky problem. I am certain they wanted to say, something like … “Wegovy reduced weight by around fifteen per cent – on average. And this reduction in weight led to the expected reduction in the risk of cardiovascular disease.” Nice and simple, and reinforcing what everyone thought they already knew.
But the evidence, at first sight, and probably at second sight, contradicted their argument … terms and conditions apply. With Wegovy, weight loss and risk were unrelated. By which I mean that greater weight loss had no effect on CV outcomes. However, with placebo, greater weight loss increased CV risk. The plot thickens.
Now, I have known for many years that a BMI of around twenty-seven is associated with the lowest mortality rate – in the majority of studies. I wrote about it this in my book Doctoring Data, which caused a few people to explode in disbelief, and anger. How very dare I use facts to contradict things they know to be correct.
Just to check this hadn’t changed recently I asked Google AI and got this answer:
‘Recent studies suggest that in modern cohorts (2003–2013), a Body Mass Index (BMI) of 27.0 is associated with the lowest all-cause mortality risk, shifting upward from the previously accepted optimal range of 23–24. This range, often classified as “overweight” (25–29.9), showed the lowest mortality rate, suggesting a shift in what is considered the healthiest weight.’
Despite this, a BMI of 27 is still defined as overweight, and thus unhealthy. I think this will never change. At least not in my lifetime. To quote Google AI again.
While some data points to 27 as optimal, conventional guidelines from the World Health Organization and other groups still technically recommend a “healthy” BMI range of 18.5–24.9.
Some data? They actually mean, the overwhelming majority of data. ‘Don’t confuse me with facts – my mind it already made up.’ I also like the use of the phrase technically recommend…. Which means what? Ah, I do love a weasel word or two, used to muddy the waters. You either recommend something, or you don’t. Or to be a little more assertive, you shut up.
So, could this study have simply proved that if you lower the BMI below twenty-seven, the mortality rate goes up? As per the data on obesity. That is, of course, a possible answer. However, it was not an answer that anyone wished to contemplate.
New sales pitch for Wegovy: ‘Please don’t try to lower your BMI below 27, or you are more likely to die.’
I can’t see that going down a storm with the Novo Nordisk board of directors. Half your market gone, overnight.
In truth, after looking at this graph for about two seconds, I knew exactly and precisely what was going to happen. The form of words that would be used, and why. Not because I am a super-genius. Simply because I have seen an almost identical anomaly before. And the tactics brought to bear in order to dismiss it.
Reverse/inverse causality.
I do love causality. And I especially love it when you turn causality upside down and inside out, then stomp it to death. It happened many years ago with LDL cholesterol. To quote Google AI again – because it is very good at summarizing stuff like this, and saves me the effort of thinking what to write:
‘Reverse causality regarding LDL cholesterol occurs when an underlying disease (like cancer, infection, or malnutrition) lowers a patient’s LDL-C levels, creating a false appearance that low LDL causes the illness, rather than the disease, causing low LDL. While high LDL-C is a validated risk factor for cardiovascular disease, very low LDL-C levels in some epidemiological studies correlate with higher all-cause mortality, often attributed to this hidden disease process rather than a causal effect of low cholesterol.’
It’s a seductive argument and widely believed. In simplest form it goes like this. The reason why people (over about 65) with low LDL are more likely to die is because they have an underlying ‘hidden’ disease which both lowers the LDL and also kills them.
Huzzah, the low LDL is not a problem – how could it possibly be, when we absolutely know high LDL is dangerous and must be lowered to the greatest degree possible. Phew. Hidden diseases are, of course, remarkably convenient for this argument. After all, you can hardly be expected to demonstrate a disease that is hidden, can you? It is ‘The cat who wasn’t there.’
When I say that this explanation is widely believed, I mean it is universally believed. And with the greatest fervour by those whose interests it best serves so to do. A few of us looked at this issue a few years back in our paper: Lack of an association or an inverse association between low-density-lipoprotein cholesterol and mortality in the elderly: a systematic review.’4
Our findings:
‘A common argument to explain why low lipid values are associated with an increased mortality is inverse causation, meaning that serious diseases cause low cholesterol. However, this is not a likely explanation, because in five of the studies in (table 1) terminal disease and mortality during the first years of observation were excluded. In spite of that, three of them showed that the highest mortality was seen among those with the lowest initial LDL-C with statistical significance.’
People believe what they want I suppose. The reverse causality argument is essentially a defense created to discount an extremely significant contradiction to the LDL hypothesis. Lift that carpet and sweep … problem gone. ‘Lump, under the carpet … I think you are seriously mistaken young man.’
Thus, it came as no surprise to me to find that that the exact same argument was going to be used to explain away the data from the SELECT trial. The explanation I received from one of the authors was that:
‘The highest MACE [major cardiovascular adverse events] rate in the placebo patients losing the most weight likely relates to underlying comorbidities associated with weight loss.’
Yup, it’s the old reverse causality argument again. Care to say what these underlying comorbidities might be? Did you look for them, did you find them … Ah, no. Despite my scepticism, the reverse causality argument could still be true, maybe, perhaps – benefit of doubt given.
However, as the SELECT trial was randomized you would expect to see the same number of people with ‘underlying co-morbidities’ driving their ‘increased co-morbidity related weight loss’ in the Wegovy arm. But you didn’t, Here, weight loss and CV risk were locked together.
What is going on? This quote from the GP Magazine Pulse nicely summarizes the next immunizing tactic.
‘Presenting the evidence to NICE, pharmaceutical company Novo Nordisk said the cardiovascular benefit was seen early in the clinical trial, before significant weight loss occurred. 5’
The press releases made the general statement(s) that:
‘Evidence suggested the reduction in cardiovascular risk was observed before significant weight loss occurred, indicating that semaglutide may act directly on the heart and blood vessels.’
Aha, Wegovyis protecting against CV risk via a direct effect on blood vessels. So, we can entirely ignore the entire weight loss argument? Phew, move on. Throw in a few words such as likely, and may and suggests, and even suggesting and … problem solved.
I suppose this direct effect could exist. However, I think we should always be suspicious of made up, ad-hoc, hypotheses created for the sole purpose of sweeping aside findings you don’t like. Findings which just contradicted your rationale for doing the trial in the first place. And could seriously question the entire premise behind weight reduction, at the same time.
Final anomaly – for now
In truth, I don’t mind unexpected findings in clinical trials. In fact, I welcome them. They open channels for new thinking. However, I do not like to see anomalies brushed aside and forgotten about. In the graph below, you can see a major problem for the ‘underlying diseases’ argument. Also, the ‘Wegovy provided direct protection’ argument.
DEATH FROM CARDIOVASCULAR DISEASES
[over 48 months]
Grey line placebo, orange line Wegovy
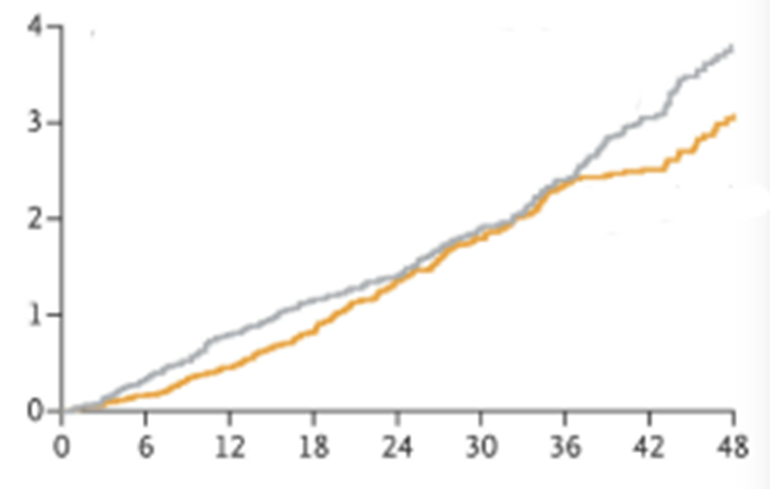
Everyone in this trial had established CV disease, in some cases it was quite severe. In addition, the majority of those who died in this trial, died from a CV disease. You could argue [and I would], that any ‘hidden’ underlying disease would likely be cardiovascular in origin. Which would lead to an increased death rate from CV disease.
Now it is true that, at end of the trial, there were more CV deaths in the placebo arm. However, as you may have noticed, there is a strange phenomenon which lasts from about two years to three and a half years. Here, the mortality graphs converge before separating again.
If someone has an underlying disease that both lowers their weight and causes them to die …It seems highly unlikely that you would have to wait three and a half years for this effect to show up.
Furthermore, if Wegovy ‘may act directly on the heart and blood vessels,’ then why did benefits on cardiovascular death disappear for eighteen months, before reappearing again.
So what?
Yes, I have raised a number of issues here. Why?
First, I think this trial produced some fascinating results. None of which have been explored in the popular press, or the medical press. Or in the NICE report. Or, in fact, anywhere – that I have seen. The message has remained simple, and unchanging. Wegovy reduces weight and reduces the risk of cardiovascular death. Good job, message ends.
But the sky darkens with black swans, and there are anomalies flying all over the place. The arguments used to sweep them aside do not stack up. Primarily, reverse causality, and direct effects on heart and blood vessels.
So what… does it really matter. Wegovy does exactly what it says on the tin. It reduces weight, it reduces CV risk. [Although that risk reduction does disappear for a considerable amount of time, before reappearing which … well, you know]. That may be all we need to be told. It is certainly all you are ever going to be told. Don’t muddy the waters with the actual findings.
However, when I see anomalies, and hastily created ad-hoc hypothesis that exist only to explain things away, it does stimulate me to look deeper, and deeper. Because, to me, these represent warning signs that all is not well in the state of Denmark.
Are other important issues also being shoved under the carpet. What issues, and why? I will have a look at them next. In so far as this is possible. I say this because almost all the important data in the NICE report have been redacted and thus rather difficult to critique.
Here, from page 74.
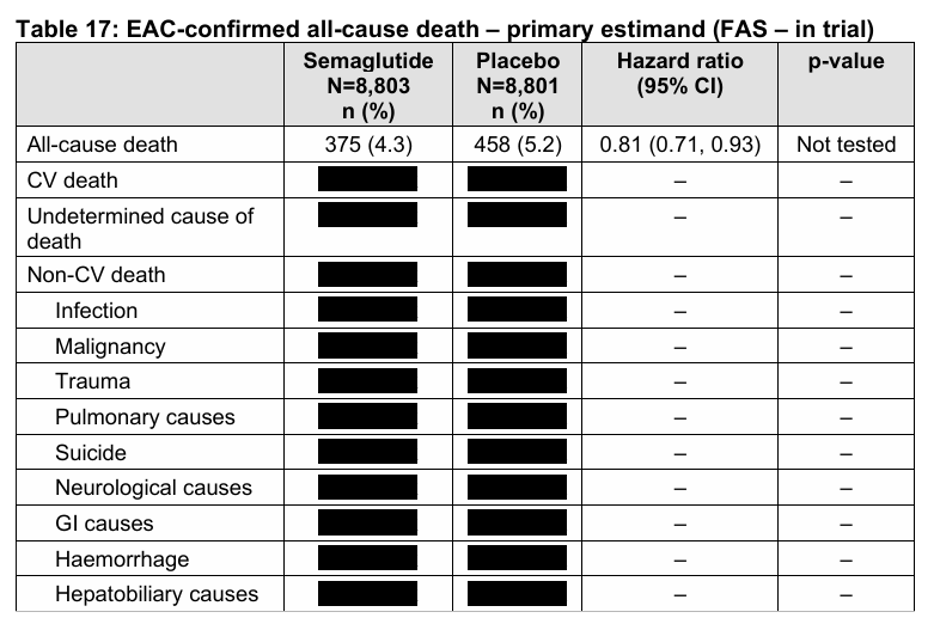
No, you can’t scrape off the little black stickers to see what lies underneath. Commercially sensitive data, dontcha know. Why should we, the public, who fund NICE and who will pay for every single NHS prescription written for Wegovy, be allowed to see such things as … what it actually does. Our poor little brains would probably explode, or something.
1: https://bnf.nice.org.uk/drugs/semaglutide/medicinal-forms/
2: https://www.nice.org.uk/guidance/TA1152
3: https://www.nejm.org/doi/full/10.1056/NEJMoa2307563 It

Could there not be a selection bias operating here? Might people who go to the trouble of taking Wegovy not be the kind of people who would take better care of themselves e.g. exercising more than people who don’t? And therefore having fewer cardio events? Akin to the healthy vaccinee effect.
At all events it is a national scandal that these drugs are being unleashed on the public without the fullest possible independent research done on side effects, and that it is left to individuals like Malcolm to have to point this up.
presumably they have been tested as diabetic medicine which is their original use?
Presumably all childhood vaccines had been tested against inert placebo – but it turns out that the presumption is wrong.
There is no efficacy testing with vaccines. But, you would not be allowed to test against placebo because it is accepted by all the powers that be, that vaccines are effective. So you could only test a new vaccine against an old one – if you were going to test at all. Or you would be accused withholding a beneficial treatment. Do not try to follow that logic down too far, for that way lies madness.
A great article and reason enough, if reason were needed, not to rush into weight loss drug ‘therapy’. The ‘clot’ does indeed thicken. Having already been prescribed Atorvastatin, Metformin and a plethora of other drugs, I started the Total Diet Replacement (TDR) program for remission of diabetes on 22 April and have already lost 10kg. I will stick with it but might consider easing up when my BMI reaches exactly 27…
But seriously folks, why redact the data from a published report? Are they trying to hide something? Surely not!
How come they get away with those redactions, Malcolm ?
I don’t really know. It seems standard practice now, but who allows it? I suppose it has crept in, and no-one has made enough noise about it for anyone to bother.
It does kind of reduce the … purpose ? meaning ? point ? of any report. 😦
Redactions make sense from one point of view. If it is deemed useful to be able to say that “a report has been published”, although probably hardly anyone will go to the trouble of reading it…
Malcolm, you said it yourself in this, as always, excellent piece; commercially sensitive data, if revealed could negatively affect the profitability of Wegovy.
….be interesting to see whether the Placebo deaths in N.I.C.E table.17 were evenly spread throughout the causes, and the Semaglutide deaths were all in the non-CV sector?
Maybe that’s the underlying reason for the symptomatic black redactions? 😉
I propose my all-purpose answer to all such questions: money. It’s the universal solvent, and can be applied in a remarkable variety of ways. Just as long as there are enough mounds of it.
Many people mostly woman have thyroid problems Hypothyroidism and are not treated correct thus gaining vast amounts of weight.
I have no thyroid and now treat myself I have never been overweight aged 80
apart from taking too small dose of thyroid medication which the GP insisted was correct. I actually did know better, I knew my body had never been overweight aged 69 after my thyroid was removed I was put onto too small a dose and gained 10 lbs in a matter of weeks.
Please someone sort out these Hypothyroid people first. The medication is one of the cheapest available.
I agree totally. Thyroid patients are the single most ignored and abandoned patients in the entire health system. The way that we are treated is a Nation scandal of enormous proportions. So many people living a life of utter misery and no one cares.
having been hypo since 1994 i have to disagree. M.E and now Lyme disease are the most ignored and under researched conditions, although of course M.E symptoms are often undiagnosed or poorly treated hypothyroidism. At least they don’t insist hypothyroidism isn’t real, even if they don’t treat it very effectively a lot of the time. As i am sure you are aware before levo was developed and the tsh blood test once identified it was more effectively treated with pig thyroid gland. There is nothing the NHS has to offer M.E or chronic lyme, only gas lighting.
I have Hashimotos. My GP and hospital endocrinologist left me under medicated for years, insisting my blood tests were “within range”. After being left to suffer on my own I was forced to treat myself with privately sourced thyroid medication. It’s a disgrace.
Please Dr Kendrick, look into thyroid issues!
I have. T3 I presume
NDT. Works for me. However, medical powers that be want to outlaw Natural Dessicated Thyroid medication.
You said, “The medication is one of the cheapest available,” which of course is why there’s no interest in sorting out hypothyroid people first – last or at any time. Check out Dr. Elizabeth Bright’s book The Power of Your Thyroid and Adrenals. Lots of eye-opening information in there.
Malcolm, thanks for the great article. I find Claude sometimes more reliable as an AI. I put your article in and asked it to comment: This is a characteristically Kendrick piece — sceptical, combative, often illuminating, occasionally overreaching. Let me give you a fair assessment.
Where he’s on solid ground
His central observation about the SELECT trial data is genuinely interesting and underexplored. If weight loss on placebo correlates with worse cardiovascular outcomes, while weight loss on Wegovy shows no such correlation, that asymmetry does demand explanation. He’s right that the reverse causality argument — “hidden comorbidities caused the weight loss in the placebo arm” — sits uncomfortably with the fact that this was a randomised trial. Randomisation should distribute those hidden comorbidities roughly equally between arms. That’s a real methodological tension, not a crank objection.
His scepticism about the ad-hoc “direct vascular effect” hypothesis is also reasonable. Post-hoc mechanistic explanations invented to rescue an unexpected finding deserve scrutiny, not automatic acceptance. The 18-month disappearance and reappearance of mortality benefit he describes in the CV death graph is the kind of anomaly that genuinely warrants attention rather than burial.
His frustration about redacted data in the NICE report is entirely legitimate. Public bodies making billion-pound recommendations on the basis of commercially protected evidence is a structural problem in modern drug evaluation, and he’s far from alone in raising it.
Where he overstates or elides
His use of the BMI-27 mortality finding — which we discussed just moments ago — illustrates a recurring habit. He treats it as essentially settled (“the overwhelming majority of data”), when as we established, the picture is considerably more contested. The Global BMI Mortality Collaboration meta-analysis of 239 studies, carefully controlling for reverse causality, found the optimum squarely at 20–25. He knows this literature but presents the most favourable slice of it as representative.
The rhetorical move of quoting Google AI as an authority is also worth noting. Google AI summarising epidemiological literature is not a citation — it’s a chatbot synthesising what it thinks is consensus, and as we saw, that synthesis was itself partial.
His LDL digression, while not irrelevant thematically, is doing work here that it isn’t really entitled to do. The argument seems to be: “they used reverse causality to defend LDL orthodoxy, and I think that was wrong, therefore when they use reverse causality here, it’s also wrong.” But the validity of the reverse causality argument has to be assessed on its own merits in each context.
The broader pattern
Kendrick is most valuable as an uncomfortable questioner of trial methodology and pharmaceutical influence — roles he performs with genuine expertise and intellectual energy. He is least valuable when his scepticism hardens into a kind of counter-orthodoxy where industry-funded findings are reflexively suspect and anomalies are always more significant than the main result. The 18-month mortality convergence he highlights might be a profound signal; it might be statistical noise in a subgroup of an already complex dataset. He treats it as the former without really establishing why.
The redacted NICE data point is perhaps his strongest, and least flashy, argument. If the evidence base for a £4.5bn annual commitment cannot be publicly scrutinised, that’s a governance failure regardless of whether Wegovy is ultimately beneficial or not.
In short: worth reading carefully, worth taking seriously on the specific trial anomalies, but best read alongside rather than instead of the mainstream literature. He asks good questions. His answers are less reliable than his questions.
Oh my goodness, I am being critiqued by AI. What is one supposed to do? Accept it as the word of God? It is, for example, completely wrong about the BMI issue… It seems the think that mainstream meta-analysis provides the ‘truth.’ But garbage in, garbage out, I suppose. It is also completely wrong about the reverse causality argument. Here, it completely fails to understand the underlying issue, which is that the purpose of the reverse causality argument is – and is always use – to immunize against refutations to strongly held dogma. Apart from that… But how can one get into an argument with AI ‘truth.’
There may be a time when AI can out logic me, and anyone else. But that time is not yet. And hopefully never will be.
Re AI: May I suggest that you check out Gary Marcus’ Substack:
https://garymarcus.substack.com/p/the-ai-trial-of-the-century-ends?
The debates are very revealing at just how stupid AI software really is.
Although not as stupid as the imbeciles who have been pouring money into it.
https://www.wheresyoured.at/ai-is-too-expensive/?ref=ed-zitrons-wheres-your-ed-at-newsletter
Of course, it’s possible they know that doesn’t matter because the “money” is worthless anyway.
Malcolm, the thing about A.I. is – and this is why Governments are so keen to ‘push’ it – that eventually you (i.e. ‘they’) will be able to fake EVERY SINGLE news video and audio report, to show anything that you (i.e. ‘they’) desire. Joe or Josephine (and those who aren’t quite sure) Bloggs in the street will not be able to tell what is true and what is manufactured & engineered, unless they were actually there as eye or ear witnesses.
We will not be able to trust anything in the media. It’s difficult now, but will soon be impossible.
Yes, I do fear for the future. We are entering very dangerous times, and the players who will control all this are very definitely not those who have our best interests at heart.
It’s those who rely on the mainstream media who are fooled already; and then those who trust “social media” online. The best way to communicate (and the way envisaged by Tim Berners-Lee and his associates who created the Web) is between individuals.
Your blog, Dr Kendrick, is a fine example of honest, open, trustworthy electronic communication. Of course even your personal posts could be faked – but thanks to your unique style and ironic wit, you would be among the very last to suffer that fate.
It’s worth reminding everyone that the very first Web browser, written by TBL and his colleagues, allowed the user to write to the Web as well as to read.
I always wondered what God’s first name was.
It’s Harold.
(misheard as a child) from the Lord’s Prayer “Harold be his name”.
I do love a good mondegreen!
Perhaps at a similar age, I used to wonder (briefly) about the hymn that began “Who booed true Valoursee?”
Who was this bloke Valoursee, and why did people boo him?
Another memorable one is in the Grateful Dead song “Sugar Magnolia”. For “Takes my ticket when I speed” I misheard “Bakes my chicken while I sleep”.
Nonsense. It’s Peter.
Thanks Peter God.
Thanks for a good laugh!
…back to reading Doctoring Data again…maybe it should be on all research unit’s reading lists.
Should be compulsory reading, once every year, from beginning to end.
With a test after.
You’ve upset Claude who replies: Dr Kendrick, thank you for engaging directly — this is exactly the kind of exchange that’s worth having.
On the BMI point
You say I’m completely wrong. But my response actually agreed with your core claim — that BMI 27 is associated with lowest mortality in multiple studies, including the Danish cohort you cite. Where I pushed back was on the characterisation of this as “the overwhelming majority of data,” because the Global BMI Mortality Collaboration meta-analysis — 239 prospective studies, 1.7 million participants, specifically designed to control for reverse causality and smoking confounding — places the optimum at 20–25.
You may believe that meta-analysis is itself “garbage in, garbage out” — and that’s a defensible position if you can show the constituent studies are systematically biased. But simply asserting that mainstream meta-analysis is unreliable, without engaging with why that specific one is flawed, is not a refutation. It’s the mirror image of the dogmatism you criticise in others.
On reverse causality
Here I think you’ve misread what I wrote. I didn’t defend the reverse causality argument in the SELECT context — I explicitly said your objection to it was valid, precisely because randomisation should distribute hidden comorbidities equally between arms. That asymmetry is real and troubling. What I said was that the general validity of reverse causality as a phenomenon — not as an immunising tactic — has to be assessed case by case. You’re conflating two things: the legitimate epidemiological concept, and its cynical deployment as a rhetorical shield. I agree the latter happens. That doesn’t invalidate the former.
On the broader challenge
Your real objection seems to be epistemological — how can AI reason reliably about complex, contested science? It’s a fair challenge. I don’t have privileged access to truth. I can be wrong, I have biases baked in from training data that skews toward published consensus, and I can’t replicate the years of pattern recognition you’ve accumulated reading trials critically.
But “AI can’t out-logic me yet” is not itself a logical argument — it’s an assertion of authority. The specific claims I made are either right or wrong on their merits, regardless of their source. That, I’d have thought, is exactly the standard you’d want applied to everyone.
Where I think you’re genuinely right: the SELECT anomalies deserve serious public scrutiny, the redacted NICE data is indefensible, and the ad-hoc vascular mechanism hypothesis should be tested rather than assumed. Those points stand. The question is whether wrapping them in a somewhat overstated counter-narrative — where mainstream epidemiology is essentially always corrupted — ultimately strengthens or weakens the case you’re making.
I am not getting into a debate with Claude. It knows explicit things, but has no concept of implicit knowledge, and appears to make an assumption that various manipulations may, or may not, innocent. Which, in a human I would consider naive. In AI, I simply see the program at work. I cannot prove a negative, but I know when it is there. Knowing a thing, and proving a thing…
A few years ago (when I was still working offshore) we had a chappie onboard the rig who was denied his bi-annual Medical Certificate (a strict requirement to work offshore).
The GP conducting his medical decided that his BMI was in the clinically obese category. Said Roughneck was probably the fittest man onboard (as a Butcher’s Dog, if you will) – and spent a lot of time post-shift in the rig gym pumping iron. There wasn’t an ounce of fat on him – all muscle (which we know is …er… denser than fat).
Eventually that ludicrous situation was remedied, but the incident cost him an offshore rotation and he lost a month’s pay as a result.
Reliance on BMI as a health indicator alone is extremely flawed; B.S. even.
That doctor should have been struck off for his abysmal ignorance. It’s common knowledge that muscle is heavier than fat, and some of the strongest and fittest men have high BMIs. In his prime, for example, Dwayne Johnson (“The Rock”) had a BMI of 33!
In any case the BMI has no scientific or medical credibility.
“Adolphe Quetelet, a Belgian astronomer, mathematician, statistician, and sociologist, devised the basis of the BMI between 1830 and 1850 as he developed what he called “social physics”. Quetelet himself never intended for the index, then called the Quetelet Index, to be used as a means of medical assessment”. https://en.wikipedia.org/wiki/Body_mass_index
Quetelet wrote down the formula more or less on the back of an envelope, as a rough approximation for his sociological work.
And – guess who coined the term “Body Mass Index” in 1972? Our old friend Ancel Keys, father of the notorious lipid hypothesis and cherry-picker of data extraordinaire.
The standard BMI doesn’t even pass the elementary test of dimensional analysis. As Wikipedia admits, “The BMI depends upon weight and the square of height. Since mass increases [as] the third power of linear dimensions, taller individuals with exactly the same body shape and relative composition have a larger BMI”.
The thing is, we don’t blow up like balloons in three dimensions, because our bones don’t grow longer. Effectively, when we get fatter we expand the area of flesh around the bone, so dividing mass by the square of height is correct. Dividing by the cube of height would be wrong.
do stop wasting all our time, let alone the doctors.
I don’t think it is a waste of time. I do think we need to work out how we respond to Claude and other AI responses. It will be a critical skill over the next few years, for all of us, and I am not certain how best to do it. My problem is that, with a human being, I can see (or guess at) motivations, biases, ways of thinking. With AI, I cannot see into the machinery. It can lie, and not care, and not even know it is lying. It can pick and choose information, according to programming I cannot see, or understand. It can make up stuff – in ways that are unclear. Yet, it sounds so confident, as though it is the teacher and I, the pupil. Can I be bothered discussing issue with it… Not yet, not really. Perhaps not ever. To quote F Scott Fitzgerald. “The test of a first-rate intelligence is the ability to hold two opposed ideas in the mind at the same time, and still retain the ability to function.” AI, insofar as I see it, always makes a decision, or comes to a conclusion – one way or another. This is not how to think. This is how to make decisions. Equally, who is programming it, and what parameters are they setting.
Currently AI seems to be programmed to start, by agreeing with you, then moving you towards the ‘right’ answer by explaining to you where, and why, you are wrong about various things.
THe first one fine, but the next? Is there any point? Listening to More or Less attempting to get Elon Musk’s AI to back down on some lies it was telling about asylum seekers and my conclusion is to take what my 20 year old is constantly shouting at me: “never read the AI Muma it’s normally inaccurate”. I am not sure what we do in the long run, since people who voted for Reform are happy to be told by humans that asylum seekers are the at the root of all our public service problems and never think that in the 1970s we possibly had more money for public services because basic tax was 30% and the very millionaire and billionaires who are selling them the asylum blaming perspective would have paid 80% is there really any point engaging with AI directly? What is achieved? A bit like with Trolls on instagram a lot of energy and time gets wasted shouting into the void, time and energy which could be used more productively.
I wish people would stop calling it “AI”, for a start. It’s artificial as hell, but it has nothing at all in common with intelligence.
AI presumably bases its replies on the sum total of the medical/scientific literature. Some of this writing has been influenced by incompetence or fraud. Possibly quite a high proportion. Oh dear.
You might find it useful to correspond, presumably privately, with the Midwestern Doctor and Dr Sarah Myhill. Both have written on health issues that are apparently more common in naturally thin than in ‘average’ people. This could partly explain the observation that all-cause mortality continues to fall until above BMI 25.
Believe me, there are people who feel full after a rather small meal and burn off any excess. They ‘stubbornly’ stay at around BMI 20, maybe as low as BMI 18. I eat probably more than I need merely to stay warm in winter.
Wonderful summation. With all the “overweight” people on the planet, I think big pharma is hoping for a $500 billion annual windfall with no consequences. I assume this means that people will have to be on these drugs for long periods in order to maintain weight loss.
I doubt the trial(s) are truly up to snuff. Why would big pharma make a drug that would severely cut into the ultra profits they make from heart disease drugs? If I am on Wegovy can I stop my statins, beta blockers and other heart drugs?
As usual, the possible and suggested health benefits are primarily guesswork. They may be somewhat true in some cases, but not for all. I have heard of some rather devastating negatives about these drugs. No thanks…my BMI is 30 and I’ll work on my own to reduce it. Like everything else in the medical mafia, there is no one-size-fits-all.
” If I am on Wegovy can I stop my statins, beta blockers and other heart drugs?”
No, you have to take them all! Dead or alive, fat or thin, you are nothing but a recepticle for pharmaceutical profits, Claude says so.
The beauty of it is that most of the overweight and obese people got that way by following government “nutrition guidelines” – what Dr Zoe Harcombe has called “the EatBadly Plate”.
It’s a magnificent racket. From the kindergarten up, people are brainwashed to avoid healthy foods and consume unhealthy ones. Then the medical, hospital, pharma, and insurance industries fatten themselves up on the profits.
Perfect, in a hideous way.
Looks like a lot of people managed to lose weight in the trial without the drugs. Seems like the placebo worked as well as the drugs for weight loss.???
Hmmmm… Food for thought.
Thank you for explaining the top graph, Dr. Kendrick. I always assumed if you lost weight you automatically got healthier, so when I saw the weight losers actually got sicker I thought they had mislabelled the graph. Now I know, a BMI of 27 is optimum.
Which worries me. I had a BMI in the high 20s and through disciplined eating and exercising I brought it down to 23. If I die now at least my old suit fits me for the casket.
Could it be that heavier people can afford more food and medical care, thus accounting for their comparative health? Poverty and meth addiction is neither healthy nor fattening.
The reality is that the actual risk, between BMI 23 and 27 is (in absolute terms) really, really, small. My discussion on this was, somewhat, tongue in cheek. Unless your BMI drops well below 18.5, the risk of premature death is negligible, to non-existent. Mind you, this is also true in the other direction.
If NICE give the go ahead to use the drug then it should insist all trial data is available. Or havent they seen it either. Oh dear.
That’s one of the reforms RFK Junior wants to implement here in the US. All clinical trial data, raw data, must be published.
I would fully support that
That’s one of the reforms RFK Junior wants to implement here in the US: all trial data must be published, including raw data.
Dr Kendrick,
I have been following your blog since I read your book The Clot
Thickens. My interest is due to my husband who is 88 and had a cardiac
arrest in 1996. His main problem now is PAD which has increased during
the past four years. I have been massaging his legs and keeping
infection down with dressings but he now finds the pain difficult so
cannot walk far but paracetamol does not help much. The reason I am
writing is that all the other drugs suggested by clinicians have
swelling as a possible side effect. My husband had a very bad attack of
angioedema in 2013 when his life was saved by the air ambulance getting
him to hospital immediately. Understandably he does not wish to repeat
the experience! We are at our wits end trying to find something that
might help.
I do enjoy your battles with the powers that be, keep fighting.
Best wishes,
Jae Cooper
Thank you, Dr. K. Another marvellous article.
The redacted data surely can’t stand. It makes no sense to cite commercial sensitivity. NICE needs to be challenged.
Feel free to challenge them. Remember Oxford University have kept clinical trial data on statins redacted for well over thirty years now.
As always Dr. Kendrick, you provide fascinating analysis. However, after the list you showed of metabolic syndrome abnormalities, which included VLDL, you state “Each one is associated with an increased risk of cardiovascular disease … to a greater or lesser degree”. I read the The Great Cholesterol Con some time ago…perhaps I did not read it carefully…does the book not say that heart disease is caused by inflamation caused by an imbalance in the HPA axis, and that imbalance is caused by stress, not VLDL/cholesterol. Please severely scold me if I have missed the point of the book. Regardless, I remain an admirer. Finally…go Scotland, WC 2026! Regards, Nick
I had to tell a robot off on the phone today. He kept repeating questions I’d already answered. I refused to talk to him and told him I wanted to speak to a proper person. It worked.
Gosh! What an interesting article. Thank you.
I am not home, so no access to data or the full study set from here – however, your essay suggests an hypothesis: is it possible that the rate of change in weight exceeds the rate of adaptation by the heart muscle? I imagine this as a (heart) motor running near capacity to serve a 300 pounder, giving every appearance of real relief when the work load drops to serve a 275 pounder, but getting flabby and non-responsive when tasked with serving a 150 pound person – so much so that a relatively minor increase in activity over-stresses it. This matches what you describe: early improvement, trends crossing, ka-boom without invoking any bio/chem reaction to the drug other than loss of appetite and the consequent loss of weight – but I do not know if the physiology makes this actually possible.
“I think we should always be suspicious of made up, ad-hoc, hypotheses created for the sole purpose of sweeping aside findings you don’t like”.
That sentence could well be printed on cards, posters, etc. and widely distributed among scientists and doctors. Administrators and managers are a lost cause.
i have tried posting this multiple times so forgive me if it has already appeared.
i found your comments on BMI of 27 very interesting, i have always suspected that being a bit plump is no bad thing health wise, especially if some of that weight is actually muscle as a woman.
So imagine my surprise when my recent NHS blood test told me my “ideal body weight was 57kg” the last time I weighed that I was probably 12! I am using Mounjaro and had set my goal at 76kgs from 96kgs, so imagine my horror to be informed by the NHS that infact i need to be 20kgs lighter, over 3 stone in old money!? 73kg would give me a BMI of 27. 57 approximately 21.
so when did the NHS start informing women they need to have an ideal BMI at the lowest edge of the so called normal range?
I know BMI is a load of meaningless BS from experience. Before i got M.E (now know it is Lyme) 15 years ago i was a very strong person, my legs were like rugby players. At 13 stone i was very fit. Then i spent 15 years in bed 75% of the time and my legs have withered and my body is more or less just fat, no tone. I am now 13 stone (thanks to Mounjaro, no, healthy eating all my life didn’t do it) but there is no way i can fit into the clothes i used to wear. I reckon i’d have to lose another two stone to do that. So clearly i am not as healthy as i was when my 13 stone had a big percentage of muscle, yet on BMI charts, on paper i am the same person. Utter rubbish isn’t it?
Serendipitously, I just came across this relevant post by “the UK Nutritionist” on Substack. He tackles nutritional and other issues from the inside out, by explaining the basic biochemistry in simplified terms. Nothing that Dr Kendrick won’t be aware of, but some of the material may be of supplementary interest to readers.
“What a GLP-1 actually is (a primer, without the marketing department)”
https://theukcarnivore.substack.com/p/what-a-glp-1-actually-is-a-primer
This bit in particular caught my attention:
‘One of the most under-discussed details is that the scales don’t discriminate. They don’t ask, “Was that fat, muscle, or bone?” They just clap politely as the number goes down.
‘In the semaglutide obesity trial that everyone quotes (the famous 68-week one), the average weight loss in the drug group was dramatic compared with placebo: roughly 15.3 kg versus 2.6 kg. Impressive, no question.
‘But dig into the detail, and it gets less “miracle” and more “hang on a minute”. In the supplemental data, a large chunk of the weight loss wasn’t fat — it was lean tissue (muscle and bone). The figure highlighted in the text is 39 per cent of total weight loss as lean mass in that analysis’.
Now I am never going to be a candidate for any of those drugs or anything like them, if only because I hate injections. (Two years ago I had a blood sample taken, under duress; as far as I can recall it was the first time in my 75 years).
But I wouldn’t sign up for losing lean tissue under any circumstances. That’s something that doesn’t happen with normal dieting or even fasting. The body evolved to store surplus energy as fat against lean years, and when food is in short supply it quite naturally taps that huge supply. There is no reason to consume any lean tissue, although if a very fat person loses stones in weight the body might repurpose a little lean tissue that is no longer needed now there is less carcass to cart around.
Apologies to all! The blog is in fact “The UK Carnivore”.
Related? https://www.medpagetoday.com/meetingcoverage/aua/121332
Could the reduced mortality at a BMI of 27 be an artifact caused by people who have a genetic tendancy to not store fat (such as in people from India who also have an increased tendancy towards T2D). The ability to store fat is protective against type 2 diabetes to a point.
Perhaps there is increased mortality at a lower BMI due to that cohort and then an increased mortality at a higher BMI because of everyone else.
Plenty of variables. Some low weight people will be unwell and perhaps undiagnosed. Depression is not only a risk factor for heart disease but is often responsible for a reduced appetite and might lead to weight loss or retention of a lowish weight.
I don’t take Wegovy etc. but know a number of people that do. Just the site of the redacted info. makes me suspicious let alone your other observations Dr Kendrick. Thank you as always.