
[Part two of a review on the National Institute for Health and Care Excellence (NICE). Which approved Wegovy (semaglutide) for use in preventing CV disease].
Stripping it down to basics, the key messages from the NICE report were:


You may have noticed three little black boxes. Yes, redacted, redacted, and … yes, well, redacted once more. We minions are not allowed to know the [newly negotiated] cost of Wegovy for the NHS. Nor the number of QALYs (Quality Adjusted Life Years) it provides. Nor the number of added life years. And very little else either.
[A QALY represents one, additional, year of perfect health. Or two years of additional health at 50% perfect health etc. NICE dodges and dives to ensure no-one really knows the exact figure. But normally, they will recommend a healthcare intervention that cost less than (approx.) £30K. per QALY. Range £25 – 35K (~$30 – 40K). These figures were plucked from thin air in the first place, in case you are wondering].
The only important thing we are allowed to know it seems, is that the cost per additional QALY is £14,702. This is within the range that NICE consider acceptable for approval. The lower the better. I find this to be an incredibly precise figure. Are they sure it was £14,702 and not, perhaps, £14,703?
You know what I think. I think it is impossible to be this precise. In fact, I don’t think… I know. When I see a figure like this, my antennae start to twitch. ‘Dr Watson, things are not what they may seem. The game is afoot’
The first problem to confront here is that NICE won’t let anyone see the data they are using to calculate a QALY. Which does make it rather tricky to check their homework.
[—] x [—] ÷ [—]/ [—] = £14,702 per QALY
Is this correct? Well, it could be. If you would allow me to see what [—] or [—] or [—] or [—] might be. [My redacted equation used for illustrative purposed only]
Yes, I did look up the cost of Wegovy on the BNF (British National Formulary) website. Which usually has all has information you need on medications, formulations, indications….and cost. However, it is made clear in the NICE document that a completely different price was used their calculation. What price?
The closest I could get to a possible answer was on page eighteen, where they talk about a maintenance dose of Wegovy at £175.80 per pack. In this case, a pack consists of four pre-filled pens. A one-month supply.
My immediate problem is that this formulation does not appear to exist in the British National Formulary BNF, and it does not appear to represent anything like the negotiated price either? I am unsure where this maintenance dose, and cost, comes from. But this was stated in the NICE document:
List price and average course of treatment – maintenance: ‘2.4 mg presentation: £175.80 per pack. Each pack contains 1 pre-filled pen of 4 x 0.75 ml doses. Each dose contains 2.4 mg of semaglutide.’
Which is considerably cheaper than the BNF listed price of £73.25 a week. But I am not entirely sure why £175.80 was even mentioned. If it is not the figure being used to calculate cost per QALY.
In their defence, if this can be considered a defence, NICE states that Novo-Nordisk have done a deal with the NHS to provide Wegovy at a discount. And, as you can see on pages 425/6 of the report, this price has been decreed to be utterly confidential. On pain of death? 1
It is important to ensure that the current net price remains confidential in all documentation until such a time that price confidentiality is formally removed.’
Formally removed …. by whom, exactly? Hmmmm …. This is commercially sensitive data dontcha know. I imagine the very gates of hell would be opened if a pharmaceutical company allowed the lumpen proletariat to know how much they were being charged. Cry havoc and let loose the dogs of war.
And yet, what is that noise, in the distance? I think I hear pitiful cries and wailing, as tens of billions of dollars in profit slips between their bony fingers. The CEO’s bonus drops from fifty million to twenty-five million. My heart bleeds for them. Or maybe not.
Looking at this from a different direction we, the people, do actually pay for the drugs out of our taxes. Would the world of pharmaceutical marketing really implode if we were ever to learn how much they were charging us.
Moving on. If you do try to find out about the clinical outcomes, such as causes of death, you cannot see them either. See table 17. Which I mentioned in the last blog.
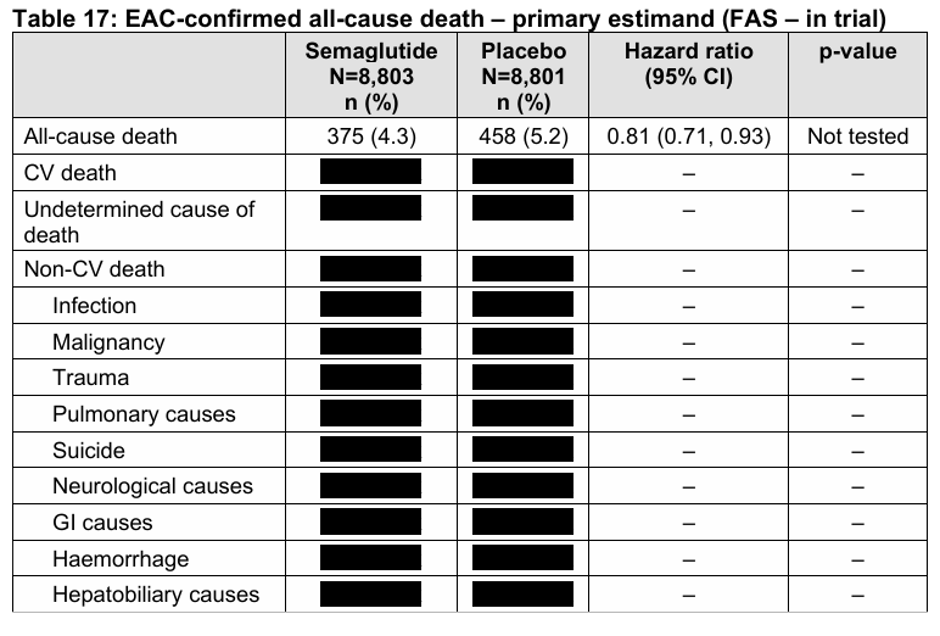
I really would like to know what is in these black boxes. Including the information on what, for example, is an ‘undetermined’ cause of death. And who decides if it can be considered undetermined, or not?
As a GP I would never be allowed to write ‘undetermined cause’ on a death certificate. Had I done so, the coroner would have given me a right earful. ‘Cause of death, um let me think … sorry. Beats me. I’ll let you decide.’ Bong! How many of these mysterious undetermined causes of death were there? No idea.
Although, the report does confirm that in SELECT, the one trial they used to create their report, they did say the following.
‘..in SELECT, deaths of undetermined cause were presumed to be CV deaths.’
Say what … You may wish to read that statement again and wonder at how this approach can possibly be justified. And if you do find some way of justifying it, please let me know.
Currently, I see it purely and simply as a way of inflating cardiovascular death figures, in order to reach statistical significance for CV deaths. I wouldn’t, of course, dream of using the word fraud …. but you know. Not sure what other word best fits. Suggestions welcome.
Why the data are hidden
I can understand why a pharmaceutical company would work hard to ensure their competitors don’t know about any financial deal they struck with the NHS. Perish the thought there might be some competition allowed. A bit of market forces at work.
Company B: ‘Novo Nordisk are selling drug x, for Y. We’ll sell ours for less.’
NICE: ‘How very dare you. There will be no grubby competition in our world. It might save the taxpayers money.’ [As would getting rid of NICE – just a little daydream of mine]
But keeping clinical outcomes a secret? That’s a different level. How can it be justified? One possible answer although, once again, I feel this represents a feeble excuse rather than any sort of justification, is as follows. If you have the time and inclination, you could reverse calculate the cost per QALY figure from the information in the report. Then you would know the discounted price.
And a long and thankless task that would be. Although I am sure company B would throw the necessary time and resources to throw at it. Pharma companies employ entire departments to do this sort of stuff. But you are not going to get very far if you can’t see the data they used. As NICE confirmed, on page something or other:
The use of the list price in the EAG report, when paired with the results reported in the CS allows back calculation of the confidential discount used in the CS.
And so, we must, just, trust … NICE? Why bother to produce a report at all, if it going to be as pointless and uninformative as this. They might as well have just stamped ‘Top Secret’ on it. ‘Contents not to be made public for thirty years, by order of HM Govt.’
In case you think page 74 was the only one with redactions. Below is figure 13. Page 88. [There are hundreds of redactions all over the place, but showing black box after black box may not be terribly interesting].
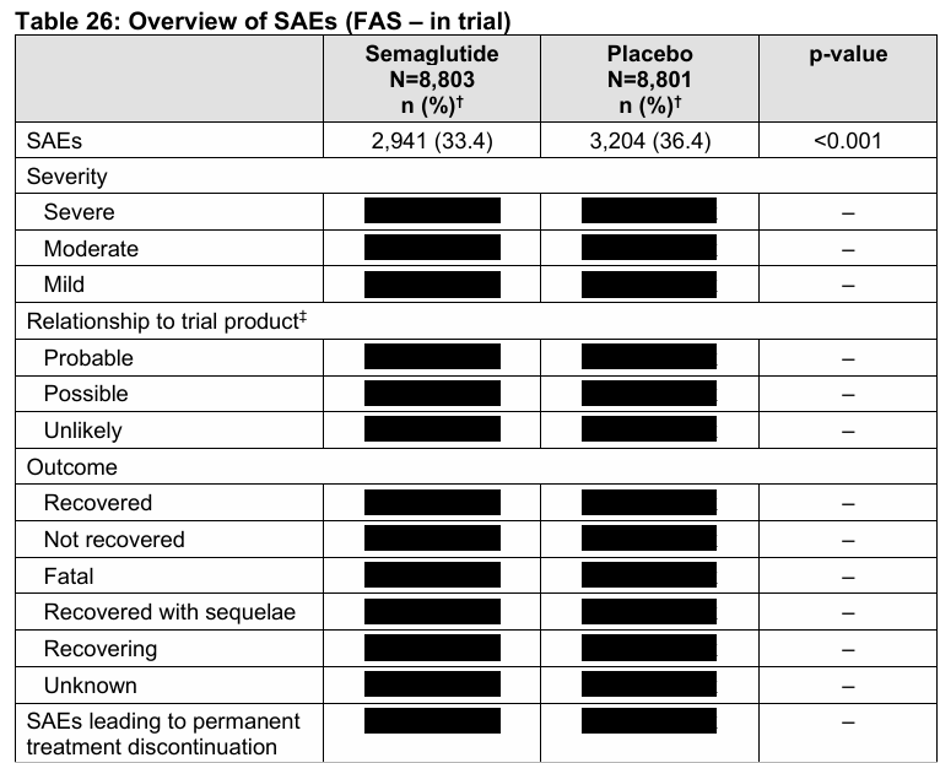
And if you want to know about Serious Adverse events (SAEs). Here you go. Page 109.
The company wrote the damned report anyway.
And, just in case you think NICE did the grunt work on this. Think again. The main report was put together by Novo Nordisk all by their clever little selves. It was called the Company Submission (CS).
It is not until you reach page 191 of the NICE report that you get anything that is actually written by NICE. Sadly, it is rather disappointing. Eighteen pages of guff which are all about process, and nothing to do with anything of interest, or importance.
Then some more guff about various stakeholders and conflicts of interest, blah, blah.
So, what did NICE actually do? You could say they simply reached for a great big rubber stamp, with the word ‘approved’ written on it. Bosh! Job done. £4.5Bn down the drain? Maybe, maybe not. I am leaning towards … certainly.
As far as I can see, they made a few ineffectual noises about a few issues, then scuttled off into the night. The cost per QALY in the NICE report remained exactly as calculated by Novo Nordisk. Not a penny more, not a penny less.
Below is one of the questions asked by NICE, and includes the answer – if that is what it can be called – from Novo Nordisk. You may, or may not, enjoy this. To do so, you will probably have to read it several times to work out what the bleeding hell they are saying.
C3. Priority question. Please clarify whether the deaths described as “CV death” and “undetermined cause of death” in CS, Table 17 are all cardiovascular deaths (as in the SELECT clinical trial report, Tables 11-14).
In the SELECT CSR, a distinction is made between “CV death” (including both “cardiovascular death” and “death of undetermined causes”) and “cardiovascular death” (written out fully). The former is also the definition for confirmatory endpoints. The CS used the abbreviation “CV” for “cardiovascular” throughout, therefore the distinction between “CV death” and “cardiovascular death”, e.g. in Tables 15 and 17 of the CS, was not as clear as in the SELECT CSR. Analyses of CV death in the economic evaluation are also aligned to the CSR definition of “EAC*-confirmed CV death”. Please note that further details on Deaths of undetermined cause are provided in Section 11.2.3 of the SELECT CSR.
*An EAC, by the way, is an endpoint adjudication committee (perhaps more on this ridiculousness later) and a CSR is a Clinical Study Report.
You may wonder why I find clinical trial reports unintentionally hilarious. In a grim sort of, banging my head against the desk, sort of a way.
Somehow or another, CV …which is shorthand for ‘cardiovascular’ (in every paper I have ever read in this area) does not mean the same as cardiovascular when the word is written out in full. Thus, a CV death and cardiovascular death are not remotely the same thing. ‘Oh, no, not at all. How silly of you to think they might be.’
‘Contrariwise,’ continued Tweedledee, “if it was so, it might be; and if it were so, it would be; but as it isn’t, it ain’t. That’s logic.”
You know, people actually write this stuff down on paper and don’t shrivel up into a little desiccated ball of burning shame. They also manage the mental gymnastics that allow them to decide that an undetermined cause of death is the same thing as a CV death. Or would that be a cardiovascular death. Or is an undetermined CV death a completely different thing altogether. Who, bloody, knows.
Why is a raven like a writing desk?
Their main protection against any criticism is that no-one, other than a masochistic madman will ever, ever … ever read the entire NICE report. Certainly not any journalist – or doctor. Or any fully functioning human being – with a life.
Even if they do, it is highly unlikely they will have any idea what it is they just read. Four hundred and sixty-six pages of [please insert insult of choice here]. I blame no-one for avoiding this report like the plague. Life is too short.
If anyone did read the report, they may inadvertently stumble across lines like this
‘The company included non-statistically significant results in the economic model.’
To be found on page 337 – of 466. If you can be bothered reading that far.
At which point I pretty much gave up. A man can only be expected to review so much of this before losing his ever-weakening grip on reality. Yes, gentle reader, they included non-significant results in their economic model. They might as well have added in hopes, dreams and aspirations and stuck on a little a meme for Hello Kitty at the side. And breathe.
As a compete coincidence, the choir I am in decided to rehearse The Boxer the other night. It contains these classic lines:
I have squandered my resistance
For a pocketful of mumbles
Such are promises
All lies and jest
Still a man hears what he wants to hear
And disregards the rest
It seemed to strike a chord for some reason. Although, to be frank, I wasn’t sure what a ‘mumble’ was. Google AI explains the line pretty well – I think.
This is a metaphor for empty, vague, and meaningless talk. “Mumbles” refers to words spoken so unclearly they are hard to understand. The narrator gave up his life’s energy, only to be paid in meaningless, deceitful words.
I need to stop here before I wander into territory that would definitely be considered libellous. If I haven’t already done so.
I will content myself with Drummond Rennie’s famous quote on clinical papers.
“There are scarcely any bars to eventual publication. There seems to be no study too fragmented, no hypothesis too trivial, no literature citation too biased or too egotistical, no design too warped, no methodology too bungled, no presentation of results too inaccurate, too obscure, and too contradictory, no analysis too self-serving, no argument too circular, no conclusions too trifling or too unjustified, and no grammar and syntax too offensive for a paper to end up in print.”
Next. What is an EAC and why…oh why.
