
Some questions puzzle me, and I search for the answer. For a number of years I am trying to establish. ‘What is T?’ My wife helpfully remarked that it is a drink with jam and bread. Ho, ho.
Moving swiftly on. My question relates to the concept of Number Needed to Treat (NNT). The NNT is a figure widely used in medicine as an outcome measure. It means how many people do you need to treat ‘T’ to achieve a benefit of some kind. The benefit can be many different things, for example: pain relief, curing a chest infection, improving pain and mobility following a hip replacement.
In these cases the ‘T’ is pretty clear cut. You have a medical problem and you intervene in some way to make it better, or cure it. But what is the ‘T’ when you are in the world of preventative medicine? If you are trying to stop something happening e.g. a heart attack, stroke, pulmonary embolism, or death, can you call preventing such things a form of ‘treatment?’
In reality, in preventative medicine, the ‘T’ turns into something else. It has become ‘P’, as in prevent. But treating and preventing are not the same thing, and you can’t use them interchangeably.
If you have a chest infection and I give you antibiotics then I have, in most cases, treated the infection. On the other hand, if you have a high blood pressure and I ‘treat’ it, all I have done is the lower the blood pressure. I have not immediately done anything else. A high blood pressure causes no symptoms, and there is nothing to be treated – other than future risk.
In fact, if lowering the blood pressure were a form of treatment, the NNT would be very nearly one, in that I will lower the blood pressure in almost every case where I prescribe a drug. But the NNT does not refer to the effect on blood pressure lowering; it refers to the number of people you need to treat to prevent, say, a stroke, by lowering the blood pressure.
As I hope is clear, in preventative medicine, the NNT should really be the NNP.
So what, you may think. Everyone working in this area knows that the NNT is really an NNP. You just need to know that when we use the term NNT, we are really talking about the number needed to treat to ‘prevent’ an event. Yes, this is true. However, the underlying problem with nomenclature does not disappear if we change NNT to NNP. The focus simply shifts to the word prevent itself. To prevent something means to stop it happening – forever.
Now, let us imagine death.
Can we prevent death? No, clearly we cannot. We do not make people immortal by lowering their blood pressure. All we can do, the very best we can possibly do, is to increase life expectancy – by some amount. Which means that prevention does not actually mean prevention. When we look at death as an outcome, prevention can only mean life extension. Or, turning this the other way round, the amount of time by which we delay something from happening.
At this point, I hope it has become clear that ‘T’ in preventative medicine has almost nothing to do with ‘treating.’ We treat nothing, we prevent nothing, we simply delay. At least that is all we can do with death. It is possible that we may prevent things such as non-fatal strokes, although we don’t really know, because we do not usually follow people up for long enough to be certain.
Why is this important? It is important for the following reason. When many clinical trials finish, and there is a difference in the number of deaths between the treatment and placebo arm, it is claimed that the difference represents lives that have ‘been saved.’ Which is another way of saying that death has been prevented which is, in turn, a different way of saying that death has been treated. NNT.
To give an example of how this work in real life I shall switch to statins and the Heart Protection Study (HPS)
Heart Protection Study
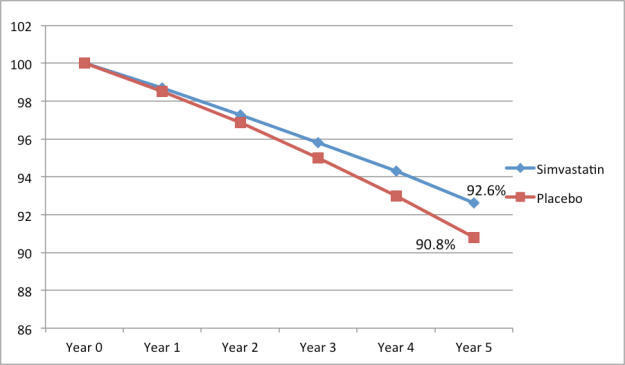
This graph shows the ‘mortality’ curves for the statin and placebo arms. At the start of the trial everyone is alive, 100% in both groups. Five years later, the end of the study, 92.6% of those in the statin arm were still alive, and 90.8% of those in the placebo arm were still alive. A difference of 1.8%.
This was presented, in the HPS press-release, as follows:
‘In this trial, 10 thousand people were on a statin. If now, an extra 10 million high-risk people worldwide go onto statin treatment, this would save about 50,000 lives each year – that’s a thousand a week.’ http://www.ctsu.ox.ac.uk/~hps/pr.shtml
This is a very clear statement. Treat ten million people, and you will save 50,000 lives per week. But are these lives actually saved. No, of course not. Below, I have re-drawn the graph and extended both ‘survival’ lines by a year. We now have a year six.
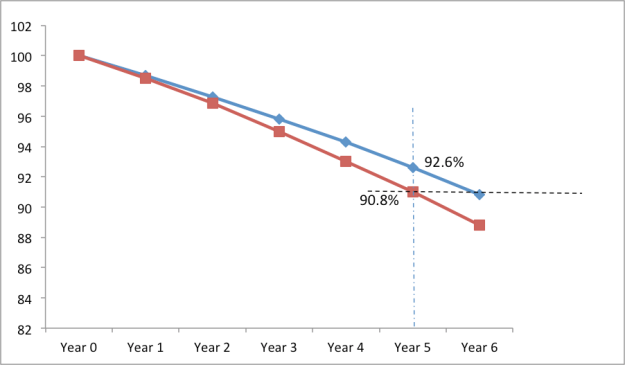
As I hope is clear, by year six, if we assume the lines continue along their previous trajectory, every single extra person who was alive in the statin arm, compared to the placebo arm, is now dead. Thus 1.8% of people did not have their lives ‘saved’. In fact, the average increase in survival time for these 1.8% was approximately six months. [Half of the 1.8% would have died after six months, which give you the mean/average].
So what is ‘T’ in this case. It is certainly not treatment, prevention, or number needed to treat to prevent death. Nor is it 1.8% of lives saved. It is a life extension of six months, for 1.8%.
Or, to put this another way. If you treat one hundred people at very high risk of heart disease (secondary prevention) with statins, what you are achieving is the following:
• 1.8 will live, on average, an extra 6 months.
• 98.2 will gain no benefit
What is ‘T?’ What indeed. Not perhaps what you first thought. T, at present, is taken to mean treatment. With preventative medicine treatment is taken to mean prevention, and prevention is taken to mean lives saved. But you cannot save a life, all you can do is extend life.
So, when someone says….
‘In this trial, 10 thousand people were on a statin. If now, an extra 10 million high-risk people worldwide go onto statin treatment, this would save about 50,000 lives each year – that’s a thousand a week.’
…they are talking nonsense.
In very short summary. NNT is a widely used treatment outcome, and it guides both clinical and economic decisions on what drugs should be used, or not used. It is a pity that in preventative medicine, NNT is meaningless, because ‘T’ has no value attached to it. Indeed, it might as well be a drink with jam and bread.

Thanks Doc for the valuable info deciphering NNT!
Excellent post – as usual!
And I guess that those ‘optimistic’ NNP numbers presented in HPS are optimistic also in the sense that they are based on optimistic statistical interpretations of the of data hidden in the company files and not accessible to external scrutinising.
Right?
Right
Again, Dr. Kendrick I understand what you may think about the statistical analyses and methodology, but if that is done by an independent entity, in this case, the Oxford Trial Unit which is purportedly independent of any pharmaceutical entity, then where would one find the actual raw data? Is it available to the public? I hope I get an answer to this. It is very important.
Thanks again Dr. Kendrick
Mary, the Cholesterol Triallists Treatment Collaboration (CTT) which is part of the Clinical Trails Service Unit (CTSU)in Oxford hold all the trial data on statins, including adverse effects, and will not allow anyone else to see it. They have signed confidentiality agreements with the pharmaceutical companies which mean that these data are kept secret and have never been seen by any other independent researchers. And, unless the law changes, never will be – it seems. You may think that this must be impossible, but it is 100% true, and I have written proof that it is so. I did a blog on it a few months back.
If there is “independent” study design and statistical analyses from Oxford…where would your average person find it? This study says so little. Can someone point me in the right direction? My limited experience with statistics is related to psychometric testing. I can’t find any specifics.
Thanks, Dr. Kendrick, I loved the graphs and your analysis is very interesting. How can you be sure about the validity of the study design and analyses for the HPS? Wouldn’t that be the most ethical part of this discussion when we talk about prevention and reduction in vascular disease? What about safety?
Thanks again.
Mary, were I to say what I really think about the methodology of the statin trials, the hidden data, the statistical manipulation etc. I would probably end up in court in the UK being attacked by very, very, expensive lawyers. So, I don’t.
The HPS statin study by Collins et al (Int J Clin Pract. 2002 Jan-Feb;56(1):53-6. described this study as a 2×2 factorial but the statistical analyses based on this protocol study design were never published. The main paper paper published in the Lancet simply ignored this and any potential interaction with the second treatment (an anti-oxidant vitamin complex). This is a unacceptable breach of protocol and consequently a serious breach of scientific integrity.
The recent book by Prof. Peter Gotzsche “Deadly Medicines and Organised Crime” outlines these problems word by word, line by line, chapter by chapter and reference by reference. While I had a shrewd idea that this was happening with the apparent acceptance by the medical establishment, this book has really demonstrated the enormity of the problem of misinformation and deliberate disinformation.
Nice post. NNT is regularly discussed in terms of relative outcomes but I haven’t seen it discussed terms of “extra years.” Your second graph and accompanying discussion should be presented along with charts addressing serious side effects for all preventive meds.
Let’s finish that calculation off. That means that those patients that stayed on their statin tablets for 5 years (ugh!) gained on average 3.2 days of extra life!
Not quite, you have calculated the life added per year.
I don’t quite get that! I mean everyone being statinated had to endure the statin for 5 years to reach the point where 1.8% would have been saved (for an average of 6 months). So I simply spread the 6 months over everyone being statinated! I suppose it should be the added life per 5 (or 6) years. Maybe I am just not thinking straight?
Anyway, I think this is a brilliant way to present the data – hardly anyone would opt to take a statin if its action were presented this way!
You also have to take into account the days gained during the five years of the trial. That is more complex and requires the use of integration of the AUC of both curves. I didn’t think a blog was a place to get into that.
Do you take requests, Doc? I’d rather like to hear your views on the accuracy of “cause of death” reports. I admit that I’m not even clear on the concept of “cause of death”. I take it that “His heart stopped” is (virtually?) always the cause of death – or is it rather the definition of death? So presumably what is being reported is why his heart stopped. The wikipedia entry is interesting, but am I really supposed to believe that busy, practical people could pay much heed to: ‘In 1967, the Twentieth World Health Assembly defined the causes of death to be entered on the medical certificate of cause of death as “all those diseases, morbid conditions or injuries which either resulted in or contributed to death and the circumstances of the accident or violence which produced any such injuries”’? Pah! So what do docs really do?
Personally, I prefer the probability of an individual benefiting or its converse, the probability of NOT BENEFITING. In many cases the latter approaches 1.0, in short, a near certainty.
Incidentally, I was recently asked to comment on a research paper as a “patient reviewer” by the BMJ. Whether I am asked again is another matter. At 81 I was surprised to say the least.
Whilst accepting (and welcoming) the basic thrust of your analysis, is it not the case that extending the graph for more than just one year would show a continuing life extension for those still on the statin treatment (I speak as one who takes it as one of my ‘5 a day’). That of course assumes that statin curve continues to exhibit a lower gradient – which is comforting but unproven (i,e, wishful thinking)
Nonetheless, as a new addition to your readership, I look forward to other interesting and stimulating blogs – for as long as Simvastatin (or blind chance) keeps me on the higher trajectory.
Malcolm that is VERY clever! You certainly think deeply about things…
Is some of the jam licked off NNT when some of the 98.2% who gain no benefit suffer adverse effects from taking statins?
I’ll drink to that comment.
I think it would be easy to lose all the extra days gained from taking the statin, sitting around in hospital waiting rooms waiting to have strange muscle problems examined!
That is so right David. I include myself in the stats of lost days due to extreme muscle pain and disability. No more!
I am prancing round London for the next week or so, with a new lease of life, making up for precious WEEKS lost due to a state of morbid statinization.
Crikey, this National Gallery is a beautiful place,and takes stamina to enjoy it to the full. I feel like singing…. “Let’s all go down The Strand, have a banana!”….but folks might stare.
And what about all those neurological problems? These take even more time – an NSAID script does not resolve them.
In the MHRA DAPs reports on simvastatin and atorvastatin nearly 30% of individual reports include nervous adverse reactions.
Dr. Nortin Hadler has emphasized this basic point in his books. Death comes one per person, and most won’t particularly care what proximate cause is written on the death certificate. So, for example, even if screening colonoscopy starting at age 50 could “prevent” some colon cancer deaths in septuagenarians and octogenarians (unproven, but possible), those people are likely to succumb to something else around the same time or not long thereafter. And to accomplish this (maybe) you will definitely cause harm to some of the far greater number of people who do not get their color cancer “prevented.” It’s an extremely important point, yet almost never discussed. Bravo.
It aint what you do it’s the way that you do it, that’s what gets results.
The detailed analysis should be focussed on the differential, finding the factors that would indicate a benefit from statin therapy, thereby reducing statiation by 95+%
I would bet the farm that the same result could be illustrated with a couple more arms, one with asprin only and one with a daily tot of brandy.
I don’t see any reference to the median age in the mortality group, other prevailing ailments in the group, gender in the group or indeed cause of death et al. It illustates what they want it to illustrate.
At a declared and narrowly focussed 1.8% it’s hardly a eureka moment is it but that is how it’s presented.
I suggest in a communication to NICE that if they wanted to reduce the incidence of statin adverse reactions they should use the selection criteria for the HPS study. No comment from them of course.
I get the impression that NICE are quick to promote a drug but very, very slow to examine the adverse effects of that treatment; understandable I suppose because the advisory committees have a preponderance of Big Pharma KOLs and wannabe KOLs.
I’ve seen quality-adjuste life years (QALY) used a few times.
Is that a good metric in your view?
So long as the correct values are used. Which is tricky. NICE use the QALY, but of course, the cost per QALY of £30k per QALY as the cut-point was a figure plucked from thin air.
I attended a seminar in Westminster about the QALY, back in 2002, led by the most obnoxious individual. At that time it was set at £8K per annum, and I felt that he thought it was already set too high for the plebs. So, 12 years on, and now it is £30k…..but all going into the pockets of big pharma, at the expense of essential services in the NHS. I never use the term “basic’ care in NHS…..it demeans the work done by all from the cleaner to the technicians and along the continuum including Consultants. Notice I use the concept of a horizontal continuum, not a vertical ladder. I learned that aspect of care in NHS in 1965……whereby we were all made to realise our labours were inter-dependent on each other’s skills. How things have changed! The services are top heavy now, with the greedy and powerful skimming off the cream for their mates, having lost the ethos of what constituted cradle to the grave welfare.
I am off on a tangent….sorry.
The HPS study. A seriously flawed study in many ways.
Personally, I prefer to consider three probabilities based on a recent claim by Collins namely “10,000 lives “saved” p.a. if 3 million treated.
First. the probability of benefit (p = 0.003 p.a);
Second, the probability of NO BENEFIT (p = 0.997 = 1.00) p.a and in conjunction with this
Third, the probability of suffering a severe adverse reaction ( p = 0.1-0.2).
This study was designed as a 2×2 factorial experiment with ~5,000 in each of four groups. The statistical analysis based on this design was never published probably because the statin treatment was not significant. Dr de Lorgeril drew my attention to this failure (aka deliberate hiding of data and results). And that is just for starters!
I’ll quote this on Wed when I see my doc about my raised cholesterol and silver wiring, I think he wants me to go back on the statins but really what is the point. Thanks for the interesting article………
Thankyou for the clear explanation. I have been wondering for a while about the claim of lives saved. Would you mind if I copy this and show it to my GP because I have an appointment for an annual review about asymptomatic AF and he usually brings up the topic of statins. I did try statins once for a short while but the pills had adverse effects. I then started to delve into the background of and statins and have become persuaded that the cholesterol theory lacks credibility.
I’d actually quite like to know the NNTs of tea.
Green Tea kills you. I say this based on guidelines issued by the Ministry of Guesswork.
So what you are saying Doc, is that an extra six months of life isn’t worth severe statin side effects such as muscle cramping and weakness as well as higher all cause mortality?!
I don’t get it 😜
Great post.
Lets say there is a pill that will reduce my risk of heart attack by 50%. Lets say there is another pill that will reduce my risk of MS by 50%. If there were different pills available to reduce the risk of each and every disease in the book, how many pills would a person be willing to take each day?
Jillm,
You might well get a better answer from Peter Piper (you know, the one who picked a peck of pickled peppers?) than any researcher or your own doctor. So ridiculous these studies on statins.
American site sent this throough my email. It might be old news I don’t know. Sounds scary to me though
“Dr. Christopher-Stine and her colleagues made the novel discovery of an autoimmune myopathy closely linked to statins. She has a continued interest in statins and their toxicities toward muscle, both as a direct muscle toxin as well as its contribution to autoimmune muscle injury. ”
and
“Statin-exposed subjects can develop an autoimmune myopathy typically characterized by progressive weakness, muscle enzyme elevations, a necrotizing myopathy on muscle biopsy, and autoantibodies that recognize 3-hydroxy-3-methylglutaryl-coenzyme A reductase (HMGCR), the pharmacologic target of statins.”
Fergus,
I thank you for this information. Dr. Christopher Stine is at Johns Hopkins Myositis Center. I was very interested in the information you passed along as she apparently has treated many who have statin related myositis. I had not heard of her, except through your post. I sure have gotten a lot of useful information from Dr. Kendrick and his followers. Sure do appreciate this!!
Thanks again!
Nice post.
Somewhat tangentially, and perhaps a not-so-subliminal blog post suggestion, but a major cause of raised BP is media/spokespeople arguing for ‘saving the NHS/taxpayer millions’ if they could only stop people smoking, drinking, eating, crossing roads, . Surely people dying sooner should in general be more likely to cost the NHS less on average by avoiding all that expensive longwinded treatment of problems throughout older age? Spending good money treating people with drugs to possibly extend their lives by small and dubious amounts by the same token thus equally baffling (commercial influences aside). Perhaps the optimal age/health targets should be individually adjusted to workers’ economic productivity / retirement ages…
Of course, from a purely economic perspective, the more that people smoke the better. Here, from Wiki:
The Public Finance Balance of Smoking in the Czech Republic was a 2001 report commissioned by Philip Morris’s Czech division following concerns raised by the Czech health ministry that smoking’s costs outweighed its fiscal benefits. The study was conducted by Arthur D. Little and found that smokers’ early mortality and cigarette-tax revenue, outweighed the costs of health-care and lost tax revenue from early death. The study concluded through cost-benefit analysis “based on up-to-date reliable data and consideration of all relevant contributing factors, the effect of smoking on the public finance balance in the Czech Republic in 1999 was positive, estimated at +5,815 mil. CZK.”
The report which was leaked on July 16, 2001 was met with condemnation and subjected Philip Morris to vitriolic criticism from politicians, anti-smoking activists, and watchdog groups. Philip Morris subsequently disavowed the report and apologized for its conclusion. Nonetheless, the suggested “death benefit” raised by the report continues to be the subject of debate.
The report was unusual as historically, tobacco companies had disputed the link between smoking and early mortality, whereas the report used the early mortality as a selling point. Though similar studies in Europe had been done a decade earlier, Philip Morris stated that it had canceled any new similar reports in countries including Poland, Slovakia, Hungary, and Slovenia.CNN reported that an Arthur D. Little representative had told them that Philip Morris had commissioned similar studies in Canada and the Netherlands, though Philip Morris stated it had no such on-going reports.
The Czech Prime Minister, Miloš Zeman had previously noted the “death benefit” stating that “By smoking, I contribute to the stability of the state budget. By buying cigarettes, I increase state revenues, and I will die of lung cancer, so the state won’t have to pay me a pension.”In addition, Zeman had stated that “As a smoker, I support the state budget, because in the Czech Republic we pay tax on tobacco. Also, smokers die sooner, and the state does not need to look after them in their old age.
Luckily, the economic benefits of killing people with cigarettes was not considered the most important factor. The primary role of healthcare is not to save the country money, but to improve the health of the people.
That was a remarkably quick detailed response! Interesting, I hadn’t noticed that story, not having been particularly interested in tobacco perhaps, and of course in general it is just common sense level of reasoning. Where it seems particularly mindbending however (and ultimately pernicious) is when such statements are trotted out by NHS / health spokespeople regarding a range of naughty behaviours of irresponsible people who are Costing The NHS…
I find it a stretch of the imagination to think that such spokespeople were applying the ‘you are costing the NHS extra’ as a guilt stick to beat us with purely For Our Own Good (health) – or using it as a morally attractive carrot opportunity to ‘help the poor old NHS’ – though not impossible of course.
Perhaps it’s the politicians that they are really trying to bamboozle with such stuff and the wo/man in the street is just caught in the crorssfire.
Alternative slogan “It’s going to cost you, but aren’t you worth it?” ?
“Luckily, the economic benefits of killing people with cigarettes was not considered the most important factor. The primary role of healthcare is not to save the country money, but to improve the health of the people.”
All well and good, however, it’s the thin end of a very, very large wedge. I don’t mind being advised but advisory often becomes mandatory and mandatory evolves into mandatory with menaces.
It’s near all over with the smokers, Its’ ongoing with wine drinkers. What’s next, hazzardous sports. Obesity, yes they’re all over that, sugar tax!. Vaping, they’re all over that. Vaping has a huge problem, it is a threat to two major vested interests, the tobacco companies and the pharmas peddling smoking cessation products.
I believe it is no secret that when the tobacco industry began to lose its grip on average citizens in the modern world, it was known to identify and target marketing strategies to those less fortunate ( poor and uneducated), our youth, or under privileged countries. Stooping to this all time low was no surprise. The opportunistic will always find a way to benefit from the vulnerabilities of others. Hiding information about the effectiveness and/or serious side effects of statins will also come to light. It may prove to be no less devastating when the truth is revealed. It is only a matter of time and subpoena power.
I always wonder when I hear any cost benefit analysis of disease and its prevention. For example, if someone keeps exercising and avoids a fatal heart attack (say), it really isn’t clear that he has saved the NHS anything – he may live on requiring all sorts of other medical help – new hips, cataract surgery, etc.
I guess in an economically ‘ideal’ world we would all die after a short illness as soon as we retire!
Based on how my mother’s death is listed in the medical records, I cannot take the statistics on tobacco-related causes of death too seriously. My mother died a few week’s short of her 87th birthday. She smoked from age 16 until two or three days before she died. She loved her cigarettes and claimed that they were the only thing worth living for after the death of my father. A week before she died, as it was clear that death was near, we called her physician to the house. He confirmed that she was close to death, but when listening to her chest declared that her lungs were “clear as a bell.” As no physician is allowed to write that someone died of “old age” in the United States, and the only infirmity she had been medically-treated for was COPD (she took theophylline for many years) her physician wrote on the death certificate that the cause of death was “tobacco-related COPD.”
Well, you’ve got to write something… In my view death certification in the very elderly is purest guesswork – in most cases.
Cost-benefit analysis? Who wrote the program and what assumptions were used in what algorithms? I came across a program recently that generates “scientific” reports.
pdos.csail.mit.edu/scigen/rooter.pdf
The authors even got a paper (a product of their program) published. I am left wondering how many of Big Pharma’s ghost written papers have been so generated.
Thanks Dr. Kendrick. I think I understand now. It is a pity that the information is kept from the general public. Perhaps that law needs challenging.
Reblogged this on Just ME in T's Health Stuff and commented:
Another wonderful – easy to understand explanation from Dr. Kendrick
Is there any instance in which total transparency of raw data in drug trials could be detrimental to the public at large? For instance, with regard to statins, other than studies authored by Dr. Golumb (thus far) the studies I have read regarding the possible side effects of statin treatment says something to the effect that more studies are needed to determine the safety and/or side effects of statin drugs (or similar language thereto). If the participants are not named, but identified by sex, age, risk factors, etc., what would be the harm in having this information (raw data)? It would appear that efforts to have this the veil of secrecy lifted have been met with political opposition that literally bogs down this effort at openness. I do believe in free enterprise and praise the entrepreneurial spirit as much as the next person. I realize companies have a right to protect their intellectual property and so this argument could be quite complicated. However, is there any danger in doing so? What is the biggest concern in terms of the impact on the pharmaceutical company’s bottom line? What are their objections? Let us be fair in this. Part of that funding for these studies does comes from the tax payer and that is where things get difficult. Think of all the duplication of studies that might be undertaken at the expense of the tax payer. Wouldn’t this system work more efficiently if researchers, patients, and doctors were able to read the most basic aspect of these trials and decide for themselves if they are willing to take the drug or trust preliminary findings? And wouldn’t a collaborative effort help all of those serving the healthcare needs of people? Again, I understand and respect free enterprise but where does one draw the line? I don’t expect Dr. Kendrick to answer this question, but if anyone else who is not at risk of some expensive lawyer taking a bite out of his or her…arm, care to venture a reasonable explanation? I am really trying to understand both sides in order to weigh the risk/benefit for all concerned.
A good question. I know little about the current process and funding details so just looking at it from an exploratory perspective: It should be quite reasonable to insist that any drug a company is seeking approval to foist on the public should be subject to a full *independent* impartial review which must require full access to trial data.
The IPR / patents etc. should surely be in the drug, not the trials used to validate them?
I don’t know at what stage drug designs can be patented – presumably it has nothing to do with the safety of a drug, and so could be applied for before any data/trial resuslts need to be released? Just guessing there though.
I would suspect there is only a very slight chance of helping your pharma competitors in any significant way by giving them the benefit of your _trial_ data – since presumably this does not imply abandoning your IPR, or even necessarily revealing much about your Secret Formula? And if you do not need to reveal it until you have a good drug and genuine solid data to back it up then what’s the problem? You might at a stretch of the imagination in some rare circumstances give your competitors some tactical knowledge advantage by a drug failing approval. But it’s not that quick a game is it? And you would never bother submitting anything that was going to fail of course…!?
An independent and transparent review based on full access to data could be funded from the public purse and/or an industry ‘application fee’.
Or going further perhaps the companies applying should have to cover the costs of a mandatory full independent trial?
Having to face up to this hurdle might really sort some wheat from the chaff at the outset ?!
One can imagine a lot of scope for arguments about all this however…!
“Your official trial/review process is too slow, you’re killing our business (and people, of course :-)”
etc.
The arguements against full disclosure. Being mindful that most research is done on a small budget and not necessarily by Big Pharma.
1. It would take a lot of time and extra work to publish all data. Research is not well funded and financial considerations are very real.
2. Which data? Where do you stop going back in the research to publish. Research involves a lot of pre trials etc. Very difficult to draft policy that would work.
But surely before finally being allowed to push some concoction down people’s throats even if you (as a commercial pharmaceutical venture of some size/kind) had made use of various pieces of research, possibly by subcontracted 3rd parties, academia etc. in developing your product, you just then need one final open and demonstrably non-warping fully auditable trial in order to prove the safety and genuine efficacy of the final result? It does not necessarily require everything along the way in the lead-up to be auditable in that case.
I do have a slight problem however, in general, with the idea that published scientific results are science at all (and thus fit to underpin something of public health concern) without the full supporting data being available/incorporated by some means. Otherwise it’s called ‘marketing material’ isn’t it?
Or is this hopelessly naieve/simplistic?
To me, the main problem is that the traditional sense that research is a vocation, and simply has to be done honestly has been progressively eroded. Ultimately, no amount of transparency can fix that.
We are being urged to consume a poison (statins) that can cripple some, and hurts a lot, urged to wreck our electricity supply to ‘save the planet’, urged to replace saturated fat by carbohydrates, all on the basis of obviously dodgy science.
I am sure there were always rogues in every profession, but they could not count on their colleagues covering up for them. Nowadays, there are clearly many in science who are prepared to fudge over (and thus perpetuate) the mistakes of the past.
Those patients on their blood pressure drugs are deemed to have been “saved” from a heart attack or stroke if they’re alive six months after they might have died without treatment. That they might have been suffering from dementia for a year or two won’t affect the “success” of the treatment, nor will it be attributed to their medication. The dementia epidemic is just one of those things that go unexplained, despite nearly all the symptoms featuring among the known side effects of, among other things, blood pressure medications.
My father was one of those who was “saved” by taking fists full of blood pressure drugs. A year or two into the treatment he had to quit work due to confusion, loss of short term memory, depression and a bunch of other symptoms that seem suspiciously like known side effects. For the next four years he descended into what I believe was drug induced dementia before eventually dying of a stroke. It could well be that his medication extended his life by six months, but at what cost to his overall quality of life?
For the twelve years since I was first diagnosed with high blood pressure, I have politely declined every offer of drugs that will “save” me. My mind is clear, my body is healthy and if I drop dead or am paralysed by a stroke tomorrow, I’ll have done a lot better than my father whose life was “saved”.
Thank you Mr. Mason. Perhaps the drug companies are concerned that if all trial data is subject to total transparency and by anyone for review (and assuming for the sake of argument that your father’s sad tale is true), could it be that the in addition to NNT, we would have to add another epidemiological measure we might have to characterize as..say… NNM (number needed to maim)? Sounds pretty reasonable to me. At least it is honest, don’t you think? But, then again, I am just a layperson trying to get to the bottom of something very questionable.
There is parameter known as Number Needed to Harm (NNH). It is used reasonably widely
Was told by doc cholesterol 8.7 and put on pravastatin , I don’t think I’ll bother with them and stick to the ketogenic diet. I tried to debate it but he wasn’t having it.
Roy, next time I need a blood test, I am going to ask the doctor to untick the cholesterol box.
My doctor suggested this himself – “If you aren’t going to take statin, is there any point in including a cholesterol measurement – but you can have one if you like!”
We agreed there was no point, so I don’t know what my cholesterol figure is!
It is odd to me that a sponsor can terminate a study for commercial reasons. This certainly puts participants at risk if the risk benefit relationship has not been established or if there is just enough information to “justify” a relationship before that which would seem ethical. Am I understanding that sponsors can accumulate other data from other trials to justify their obtaining patents for drugs, procedures, or medical devices, etc.? Can they do this and can they change protocol during the study? If so, who oversees or grants permission under the law? There seems to be many layers of oversight, but not enough or at best vague accountability. This is very complicated. I guess I will have to do more research, but it is indeed an intriguing subject worthy of a great deal of scrutiny.
Thanks all. I still think I was maimed Dr. Kendrick. The word “harm” doesn’t begin to tell this story.
It was interesting and encouraging just now to hear well-known food writers on Radio 4’s The Food Programme agreeing that the heart/ diet hypothesis is now known to be wrong. Perhaps “Key Opinion Leaders” in other fields and disciplines will encourage the /scientific/medical establishment to look again. Change can come from the bottom up…
Dr. Kendrick and others, I have read and researched until I am blue in the face. The conclusion I have come to is that when it comes to medications and other medical interventions, we are all nothing but a bunch of guinea pigs. That’s right. You are unknowingly part of the post marketing trial on just about any drug approved by the FDA since 1992. The fact that too many of these drugs were put on the “fast track” for approval is evidence enough that the motto and attitude of the pharmaceutical companies and its close ally, the FDA, are certainly “shoot first, ask questions later”. They really don’t seem to care since if it does not work, they will deal with it in secrecy, and face the consequences. No wonder their bottom line is so great. They have more than enough money to pay out lawsuits and never, ever learn from their mistakes. They engage in their “damage control” tactics and get on to the next drug. The FDA and pharmaceutical companies make strange bedfellows, don’t they? Pharmaceutical company’s who use televised marketing strategies should be banned from such practices. It is tacky and unethical. They act like a bunch of new cars salesmen rather than the scientific gatekeepers they should be for protection of the public at large.
There is no direct pharmaceutical marketing to patients in Australia. However, there are educational ads about diseases. “Talk to your doctor.”
Just reading through ‘Bad Pharma’ by Ben Goldacre (on Kindle), I am naturally cynical and getting more so with advancing years but I am being repeatedly shocked by the sheer criminality of the pharmaceutical industry. I am just getting to the part explaining how – now that researchers are getting some traction on forcing transparency on big pharma – phase 2 and phase 3 trials are being shipped wholesale to third world countries where they can be hidden more completely (and the trial results become more worthless).
Stephen, I just ordered Goldacre’s most recent book. I try to listen to him on Youtube, but for the life of me…he just wears me out. I learn better by reading or listening to those who speak with more clarity and deliberate speech patterns. However, he is quite the genius. Dr. Kendrick and others on Statin Nation helped me to understand a lot by not only listening but by virtue of watching body language. I have always learned more by both visual and auditory clues. You can tell a lot by one’s body language. It tells you if one is sure of his own findings and speaks to one’s sincerity. I really look forward to Dr. Kendrick’s books. Just when the information gets very technical and somewhat dry (as these subjects naturally do) with perfect timing, he makes us laugh out loud. I think that is just one of Dr. Kendrick’s greatest assets…his humanness and ability to appeal to many people. He has a great sense of humor.
Mary, I agree with you about the persuasive drug adverts on USA TV. I always look at the happy smiles and listen to the happy voice as they speedily list the many adverse side effects possible, and then end with “ask for doctor about…” This sort of marketing is very unethical.
Celia, of course it is unethical. Who are they trying to convince? The drug adverts actually make me more skeptical when I listen to the adverse effects. I used to believe that during a drug trial if even one person in the “experimental” group reported an adverse event, they had to list it as a potential side effect. I don’t any longer. I believe in the Heart Protection Study for instance, that there were many reports of adverse events among the 10,000 or so given Simvastatin, but those numbers obviously are a well kept secret. Just a couple of scenarios could be that they got dropped during the “wash out” or just dropped out themselves due to adverse side effects, but the true numbers are well hidden.
Sidney Wolfe, MD of Public Citizen, author of Worst Pills, Best Pills suggests waiting 7 years after a medication has been put on the market before taking it unless it is the ONLY option to save your life. he feels that within 7 years, a drug will establish a safety profile or will be taken off the market when the body count becomes too high to ignore
there are always older pills for the same condition where the effectiveness (or not) has stiood the test of time
Post-marketing research aka pharmacovigilance. Brought in by the FDA to expedite the authorization of new drugs to the market. Problem is and was that most front-line docs do not have time to report the drug adverse reactions (AR) reported to them. This and the fact that if the AR is on the data insert many believe that it is unnecessary to report it; if the AR is not on the data insert then it is assumed not to be caused by the drug. Result is that the vast majority of ARs are never reported (as Big Pharma knew would happen). Further result is that the MHRA DAPs for drugs (an excellent system) is of minimal use in terms of assessing the incidence of any AR because of the failure to report.
If you were to disregard the subject matter and dismiss the findings of the reseach one can still appreciate the relevance to the topic, It isn’t what you say it is, it’s who says it is and conclusively who benefits from it.
It’s an observation, I have no idea how to mend it. The only conclusion I can come to is the further you progess up the hill the more determined they will become to push you down it.
It is a gruelling watch and as said regard or disregard the subject matter, it isn’t the salient point of the excercise. The salient point is it all works the same.
Flyinthesky.
Thanks for the link to this video. Regardless of whether this treatment is shown to be more or less successful than conventional treatment, I find the witch hunt aspect unsettling to the nth degree. Are we to be denied any say in how our health is managed?
OK….in the past we were brainwashed into thinking that the doctor knew best…..but we can now see that some doctors a) know less than a good number of laymen, and b) those who do know their stuff, don’t have the bottle to practice it.
Statistics showing the high %age of adults in the UK taking prescription meds, ought to suggest a nation of newly-health-restored subjects…..but just look around…….streets are crowded with overweight, limping, breathless, pasty-faced, depressed and dejected individuals. Er….it doesn’t seem logical, does it?
Some docs are prescribing central heating for those unable to keep warm….excellent!…..(saves NHS money over time).
How about keen docs acknowledging, and then prescribing, a proper diet to improve the health of the nation? In this wealthy nation where food banks are opening at a pace of knots, it must be more beneficial than prescribing harmful drugs in anticipation of future ailments due to mal-nutrition. There is much research showing the detrimental impact on our health by ‘food-like’ edibles eaten in place of nourishing food. And there are plenty of anecdotes showing the detrimental impact of ingesting ‘anticipatory’ toxins. ( gold star for anyone who can say which drug is top of the pops).
That would leave resources for researching the awful conditions cited in the video, which seem unrelated to diet, and are quite baffling to understand.
Firstly….lets positively deal with actual problems with known answers, where quality research is being ignored by those who ought to know better. Once we have dealt with the problems caused by disregarding Maslow’s Hierarchy of Needs, we can then concentrate on the other challenges of life.
We can’t progress in any aspect of life unless, and until, we meet the demands of the 1st rung of Maslow:-
clean air,
safe food,
clean water,
shelter,
warmth,
rest, after sex.
Is Maslow off the curriculum these days? Is the concept old hat now? Or am I much older than I think I am?
Jennifer, no problem, I am quite interesred in alternate therapies though not a slavish promoter.
Advances in most scientific areas have been achieved by mavericks, there is very little possibility of progress by working within the consensus.
This is an illustration of Malcolm’s position, the consensus is that statins are beneficial and have negligable side effects. He’s done his own research and come to a very different conclusion.
I did a very poor job of illustrating the point of the film, so for those who don’t want to spend nearly two hours watching it I’ll try again.
The doctor concerned,this man is not only an M.D. he also has a doctorate in biochemistry, by his own research, had formulated a treatment plan. His focus seems to be mainly on inoperable brain cancers. Patients often abandoned by conventional medicine as untreatable, palliative care only.
After years of personal research he was enjoying some success, some indeed spectacular. Then came the involvement of the FDA, who instigated their involvement, certainly not his patients.
He was taken to local courts on a number of occasions to make him cease his activities followed by a state court appearance. The judgement from the state court was he could continue his clinic and research but he wasn’t allowed to sell or practice his treatment across the state line.
Disgruntled but still able to practice in state he thought at least that’s it, I can get on now.
Not so, he was subpoenaed by the FDA to appear before the federal courts a further four times, the grand jury we’re even briefed that no account could be taken of the treatment, unlike chemotherapy, was non toxic, no side effects and often worked.
It’s clear to me that they, guessing big pharma, just didn’t want him in the game as a lot of his treatment was unpatentable. That said, one of his research associates who advised him that this ingredient was natural and unpatentable advised him not to persue it but went on to patent it themself.
It just reinforces my belief that medicine, especially in the big ticket areas, cancer, aids, heart disease et al isn’t science at all, it’s business.
I read in the paper today that around half the women and 43% of men in the UK are on some sort of prescription medication, mind boggling!
It’s all gone a bit wrong hasn’t it.
Jennifer, just a note from the old USA. There is a strong push here in the U.S. to ensure we are not eating “genetically modified foods”. The opposition is, of course, some Senator who knows for a fact that our food supply is not genetically modified. But, he is being drowned out by those who are refusing to buy, use or support many of the manufactured “concoctions” as Dr. McBride refers to them, that are grown on a large scale by so called “farmers” (a term I use loosely). There is much more work to be done and Moslow could never have ever imagined how much his hierarchy would come to be slaughtered. On my block alone of about six houses, we have had three cases of cancer (one on his death bed), one kidney failure, and two deaths, all well under the age of 65. Each of them is or was on statin. They are dropping like flies around here and I wonder if I am living on an old Indian burial ground. That would be the best case scenario. I have always tried to be optimistic.
Jennifer, also on a positive note. My mother who lived alone at the age of 85 has been with me for the last month or so. While at home, she fell numerous times and could not get up. I called the Sheriff’s department on two occasions to come to her aid. She could not rise from a chair or sofa without falling back many times. She shuffled and had numerous dizzy spells. The dementia speaks for itself. I did not realize how bad she was until she came here full time. She lived alone with the help of a housekeeper, but her dementia and physical decline were just too much and I dare not place her anywhere but with me until I have ample opportunity to research such facilities. She was on statins for 12 years until I took her off about one year ago. Since the increase in the drug Aricept did not seem to be working at all, I decided to give it a try and put her on Ubiquinol. I started her on 200mg day. On day four, she was able to arise from a seated position without falling back three to four times. She got up, cleaned my kitchen, took her bath unattended, has not fallen and is not dizzy. I doubt it is the placebo effect since she does not know anything but to trust me. Today is day five and I am encouraged, but I won’t be convinced until more time has passed. I do think your posts have been educational for me.
Mary, that is an uplifting story regarding your Mother. I am pleased that improvements are coming about after a short time. But, as you well understand, such stories as your Mother’s will be poo-pood as anecdotal. It will take a very strong-willed doctor to formally acknowledge individual examples, let alone act upon them, yet many of us KNOW that statin intoxication can be reduced, indeed eliminated as in my own case. It is a disgrace that we are being ignored as aberrations, and I wish Dr Kendrick and his like all success in getting the message across.
Thank you for your kind words regarding my little stories. I so enjoy the technical aspects of biochemistry etc, which the academically-inclined bloggers add to our understanding of this serious business, and like yourself, I have learned so much. I hope that the superficial little tales gleaned from my Nursing years, family life, and latterly, my involvement in law and politics, add a parallel understanding of how Big Pharma, NHS in the UK, and The State System impact on each and everyone of us on a humanitarian level.
After all…..if research across all aspects of life ( i.e. Maslow’s concepts), is not for the enhancement of human life, what the heck is it being done for?…AHA…..that’s where the devil makes his entry…..it is not that money is the root of all evil….but the LOVE of money. How about everyone returning to the LOVE of humanity? Sounds like a good theme for a book?….oh….its already been done? ….well of course it has! (over the last 2,000 years, I believe.)
mary
add some coconut oil to your mother’s regimen
Flyinthesky
Another example
http://www.3news.co.nz/Living-Proof-Vitamin-C—Miracle-Cure/tabid/371/articleID/171328/default.aspx
This is the story of a NZ farmer who was condemned to death by doctors but saved by family insisting on Vit C therapy
http://www.odt.co.nz/print/126632
headed and ignored by medics is interesting.
Doctor does not always know best
This man is alive and working. Had the doctors had their way he would certainly have died having had life support turned off.
Has it had any effect on treating flu pneumonia? No! Will it have? No! Under current directives such treatment is impossible unless of course one tries the courts.
Thanks for the link Mike, what a thoroughly depressing story. It’s difficult to asess the perspective, is it genuine concern for the patients wellbeing or the stigma of being proved wrong.
If you get to a situation where the death of a patient is a near certainty, especially considering the initial response, try anything and everything. The first principle of do no harm is all well and proper but what if doing no harm means doing no good either. It would appear that if we can’t do any good we don’t want anyone else to be able to.
That was the core issue with the video link I posted, his cases in the main were those abandoned by convnetional treatment. The only side effect from his treatment was it often worked.
I don’t know whether I dare read Prof Peter Gotzsche’s book, I have enough fears already.
Happy new year.
Thank you for an excellent article, Malcolm. It is a model of clarity and should be required reading for all epidemiologists and medical statisticians… And dare I say it; NICE. I am uncertain about how we have moved from the age of applying a band aid to a cut knee, following a wash with water and a dab of chlorhexidine to the point where we must all be seen in A&E by a senior clinician and followed up for three months, just in case.
The move towards more open access research publications is welcome but when the data remain hidden and skewed by commercial interests, there is little point in holding up any particular study as an exemplar of anything. It should be clear that (at the commencement of any pharmaceutical solution) that the NNH is ever present and when examined alongside the NNP/NNT, pharmaceutical solutions would occupy far less importance than they currently do, when considering any model of health.
It is not beyond possibility that pharmaceutical companies have little interest in finding effective cures for various ailments. For they would effectively be killing the golden goose. Us, the patients in other words. It must be far more lucrative to suppress symptoms to a point where they are almost sub-clinical than to cure a diseased patient and remove their ailment.
In time, I hope that our society will come to see that NICE are a malign and detrimental influence on the health of the nation. Poly-pharmacy supported by vested Interests, combined with big sticks to ensure clinician compliance, along with the disturbing government trend of offering GPs cash to discover diseases, is unlikely to produce a healthy populace.
I hope that you and your family enjoy the holiday season.
Having an interest in mathematics, looking at those curves highlighted to me one of the biggest problems with this data – the missing data just when it starts getting interesting!
In geophysics, you don’t stop taking readings over an anomaly then just stop at the first sign of an anomaly, you keep going so you can see where the anomaly begins and ends! You don’t drill an oil well, and stop at the first sign of oil – you keep drilling until you have seen the last of it! Science is always interested in bumps, and bumps have beginnings, peaks and ends.
Of course, there is expense and statins have not been around for long enough to have tested this fully, but the sweet spot would be the 50% death rate time – for people starting at an age of 60, this would be about 20-25 years.
If the difference between experimental group and control continues to widen up till this point – then that would be the best hoped result for statins, and would provide a clear picture that there is benefit in life-long medication as it is currently prescribed (even if miniscule).
Of course after a certain amount of time, the curves must converge – this means that the death rate in the experiment group has to outpace the control after the peak benefit time. If statins provide continued benefit, this should not happen until the 50% death rate time, however if it happens sooner (as I suspect it might) then it would be a huge problem for the company and current prescribing practices.
In the name of science and good medicine, drug trials need to keep going, however it is obviously not in the interest of the company to keep trials going when they have started getting good results for obvious reasons. It is simply sloppy science and false economics to fail to test drugs (those designed primarily for longevity) until at least the 50% death rate time if not longer.
Although I don’t like the thought of vivisection, I can’t help wondering why there are no animal models of plaque build-up and heart attacks where the curves could indeed be extended much further through the animals’ life times.
I’d have thought statin side-effects might show up in animals too – cramping limbs for example, and inability to remember a maze!
David, perhaps it has something to do with Vitamin C.
David, speaking of cramping, I learned about and tried drinking a small amount of pickle juice for cramping or Charley horses which I still get with some frequency. It works quit well.
Mary,
I do want to emphasise that I don’t get cramps any more – I have fully recovered from statin poisoning – which I hope you will do soon.
You were trying to exercise yourself back to health, as I did. Do you think that is helping you?
David
Gordon,
I was just reading your response and right you are. I understand the 2×2 factorial and how and what the study wanted readers to think, but without a longer study…this tells me nothing. I cannot see how this study can have any of the reported confidence intervals without knowing more about the study design and specifics on those participants chosen. We know nothing about the demographics of the chosen participants. Without that, none of this makes any sense at all. Now, I might be speaking from a place where my primary study and concern has been in the area of the social sciences and psychometric testing. But, should we not know that information even more so when deciding to unleash a drug that can have life altering (and life threatening) consequences for the medical community and those it serves? I THINK NOT. So, number needed to treat and number needed to prevent or maim for that matter are of primary importance and should be answered by those who have the public good in mind. Those and other considerations in themselves are overwhelmingly significant to understanding and believing any study particularly for a five year only period. Just what does “at risk” mean? I don’t see those definitions anywhere in the literature. The explanations are, at best, hidden. The public has a right to know that. I fail to see how the authors can say that Simvastatin had benefit even for those without significant cholesterol levels unless we knew more about the study design itself and the demographics that truly represent the “normative sample.” Too many variables that would make this trial even worthy of reading much less using as a testament to the efficacy of Simvastatin are missing. And…apparently after some 12 years post widespread statin use…seem to be totally false and without concrete evidence. I certainly would like to see the follow up of these participants to see the number needed to harm, treat, or prevent. Now, that would tell me something. However, let us not forget also that there are widespread “patient reported outcomes” that need to be looked at in detail and in earnest. But, of course, I doubt Big Pharma is willing to allow their big bucks to be used to sink its own ship.
Yes, the exercise is helping a lot. Even after stopping statins, I felt so tired all the time. It was rather scary. I increased Ubiquinol as well. I just do not understand why it can take so long to feel better. There were times when I just gave up on exercise out of frustration. Then, I would get angry and try again. I am better and thanks so much. The cramping is not as bad, but enough that I look for ways to ease it quickly. Pickle juice does help. Who knew?
Mary,
If pickle juice works for you to stop the pain and cramps, then go for it! As you know, I used diclofenac, and I could almost measure my recovery by the amount I had to take to remain sufficiently comfortable to do my normal exercise. The prescription said up to 3 50mg tablets per day, but initially I was taking just one a day. Then I discovered that 25mg are available, so I suggested to my doctor that these might be better because I could start to lower the dose. I found I could manage pretty well on one 25mg tablet a day, then one every other day, then about 2 a week. (They are coated tablets, so cutting them would not have been a good idea!).
I did try ubiquinol (coenzyme Q10) for some of the time, but for me it didn’t really seem to make much difference.
I felt approximately normal after 9 months, and completely so by now, so it does take time – how long have you been since you dropped the statins?
It seems crazy that we have to discuss self-treatment in this way – but I guess medical profession can’t pretend that statins are very safe, while putting much effort into working out how to fix the mess they create!
I don’t know if Dr Kendrick would get into (more) trouble if he put together a page on how best to manage statin poisoning, but I think it would be extremely welcome to many!
I don’t want to get Dr. Kendrick in trouble either so there are some books out there that a friend told me about (one called “Poisoned! Recovering from Statin Side Effects” by Doctors James and Hannah Josef) that reference managing post statin poisoning. I am protective of both him and all our friends who post here.
However, I was first on Antara in 2004, which immediately caused terrific leg pain. After a few months I suffered from an abdominal aortic blockage. It was stented, but the pain remained and was so perplexing. I had never had any back issues. After a few years, my Pharmacist suggested this was listed as the number one side effect of Antara. When I approached my doctor, she gave me Simvastatin. She was clearly angry with me for asking to have my cpk levels checked. They were normal. My cholesterol plummeted to 121 and I felt worse than ever. That went on from 2008 until 2013. It has been almost a year and five months. I actually cut them in half for a few months, so it is a little confusing, but it has been over year for sure. I was hospitalized because my kidneys began to shut down, and I was very sick. My kidneys malfunctioned for one year prior (another issue I had never had). They kept me on antibiotics for a year. I knew it could not have been healthy. My CPK levels were six times normal. That was when I just had enough. After getting off statins all those symptoms went away for good. I still suffer pain, but it is not as bad and as distracting. I can deal with it. It is like the difference between feeling sore and feeling pain. One doctor actually tried to bully me into a pain stimulator with leads inserted in the epidural space of the spinal cord. I researched and there were too many cases of paralysis for my comfort. After a time, if the device stops being effective, you cannot remove the leads due to scar tissue that forms around it since it is a foreign object. You can also not have an MRI because of the titanium in the leads. I just could not do it so I kept looking for answers and I found them. I was treated like an infidel and was screamed at for refusing the intervention. I left his care.
So, like my favorite childhood story “The Little Red Hen”… I told myself, “then I will do it myself” said the little red hen…and, she did! And she keeps doing it, too. lol
David, I just researched the difoclenac and it is said to be quite effective. Do you have any stomach upset with this medication, said to be an ansaid, correct? I tried a few of them and got really sick even when I took them with food. I had not heard of the one you took, but just cannot take a lot of things because they make me so sleepy. I have also heard of Gralise, which is a extended release Gabapentin. I have a friend who had a terrible accident an has chronic pain. She has had a very good result with Gralise. Gabapentin also made me so sleepy. All this stuff scares me so much.
Thanks again, David.
Mary,
I am sorry you could not take diclofenac (I knew it could have side effects, but what doesn’t), but I think more generally the best thing is for you to find something that adequately controls the pain and cramping, so that you can do exercise – but do remember, all I am doing is describing my personal experience of statin recovery!
I noticed that you mentioned a book about recovering from statins, “Poisoned! Recovering from Statin Side Effects”. I looked it up, and it has mixed reviews because it recommends a very extreme diet of some sort. I do tend to be wary of fancy dieting advice – maybe because I like my food! But also, because I am much more cynical about diets after realising that the entire dieting advice about avoiding saturated fats and salt, was just plain wrong! Eating a reasonably balanced diet seems the most sensible approach.
When you have come to realise, by doing your homework, that the benefits of statins for people with serious heart disease, like myself, at best are very mediocre you tend to look around and talk with people taking statins to hear about obvious ‘side effects’.
One person in my surroundings is the electrician helping me now and then with my old house and he told me the other day that he did not want to take on any more jobs since he already had had three heart attacks, surgery and was now on five different heart drugs while I myself declined surgery and all drugs already 15 years ago. So, of course I asked him about statins.
“No, no! I will never touch them!” He had seen what that drug had done to one of his friends
After a couple of weeks on statins his friend had to use a rolling walker!
To me there is no science here – only religion when it is at its worse, i.e. just for profit and with utmost contempt for suffering people en masse.
Professor, I just want to say that your posts have given me much hope. I don’t have heart disease. However, my husband who had just turn 50, died of congestive heart failure. The death certificate listed a plethora of diagnoses (the first of which was hypercholesterolemia). However, he was diagnosed with CHF in June, and was dead in October. He had no heart tissue death from blockages. He was on high doses of statins and fibrates for years!!! If it is the last thing I do…I will devote my efforts at stopping this madness in whatever way I can. I pray God is with me. He sure was with you! You did the right thing. I admire your strength.
Mary,
Thank you for your encouragement and my wife really appreciated your comment!
I read this quote the other day:
“It seems that what we call science today is in reality nothing other than post-modern religion in which a created (Big Bang) physical universe exists and whose workings are explained by the credentialed priestly class dressed in white dust coats. And it seems Medieval practices haven’t changed much, except this time the persecution is rhetorical rather than physical. Or so we hope.”
More and more I think that there is much in what you say about science from what I see with my own eyes in academia.
Still I am an ardent believer in science as a means of understanding and giving plausible explanation of the only world I think exists, i.e. an external material world. The more plausible the explanations the more science I find. That is why I am on Dr. Kendricks side in the battle against the statins. There is no plausable explanation at all in official vilifying of our cholesterol and thus to me there is no science at all – only abuse of science by Big Pharma. It makes me just sick to think about it.
I too am an ardent believer and enthusiast of “science”, the problem is there is very little untainted science.
The power and opportunity that modern science confers distorts the purity of it in various degrees. So much so I have little faith in any of it.
Malcolm is doing some sterling work in his narrow focus of interest and expertise, my contention is why would any other area of science be any different.
Entities don’t secure the services of an expert to question a position, they secure the services to reinforce it. If they don’t they will be replaced by one that will. It all works the same.
Flyinthesky
Please read Prof Peter Gotzsche’s book “deadly medicines and organized crime”. Gotzsche is a MD with experience in thee pharmaceutical industry, founder member of the Cochrane Collaboration and a leader in the Danish section. The book has been awarded a prestigious BMJ award.
It will justify your worst fears!
Religion is such a funny thing. Why is it that most wars and atrocities men have visited one upon the other have been in the name of Religion? Seems rather hypocritical doesn’t it? The Big Bang theory came from Genesis. They ain’t foolin’ me!
The universe started with the big bang declare the scientists proudly, a big bang of what and who lit the fuse?
The universe was created by god declare the creationists proudly, who created God and what was the motive?
The creationists have ceded the fact that the universe was created by an omnipotent force, given it a name, have faith in it and worship it.
The scientists are still working on it but will inevitably come up with the same answer but it will be cleverly expressed by a formula Co, + Po. x In. = IOF
Conjecture plus Postulation multipied by Infinity equals Indefinable Omnipotent Force. Oops getting to sound a bit like climate science!
As to weather I’m a theist or creationist, or evolutionist I really don’t know, I like to cling to all of them because I believe that after an Infinite amount ot time has passed I still won’t know the answer.
Ho!ho!ho!
Thank you, Flyinthesky.
On that fantastic explanation, I am signing off for the year, and wishing you all a Happy Festive Season.
I have finaly decided to dress the Christmas tree today, despite a heart saddened by the dire state of our world. I must make the effort ……because you see…….
I love Santa Claus, and he is real…..honestly….just watch Miracle on 34th Street!
Good health to all in 2015.
Dr John Briffa showed interest in the notion of numbers needed to treat and blogged about them on an occasion or two. The notion is a useful tool, one that helps contextualise hyperbolic claims of reduction in relative risk. It is good of you both to bring these alternative analytical ideas to the attention of patients and interested parties like us.
John Briffa has been a dedicated blogger and strong believer in the learning points as can arise in a blog and comment arrangement. Rarely did he post less than two articles in any week. He informed his readers and at times readers leaving remarks informed other readers and even John himself. But his activities on his own blog, ‘A Good Look at Good Health’, and on ‘The Cholesterol Truth’, seem to ceased abruptly in the first week of September. I am aware of simple and quite innocent personal reasons why John might have shifted his attentions and priorities, but his absence from this side of things seems increasingly out of character and all the more untoward with the passing of time.
I have emailed, and John has usually replied in the past, but news is not forthcoming. I met John, briefly, in September 2011. He is charming, witty, and interested, and he received me warmly enough to ease my anxieties (They stemmed from the combination of my being in awe and very deprived of sleep upon that day).
Can anybody put my concerns at rest? With the sincerest and most heartfelt plea can anybody confirm that nothing untoward has befallen this courageous and pioneering advocate of more naturally oriented medical practice?
I had also noted the abrupt cessation of new articles on his blog and am concerned about this. I emailed him but got no response.
I added a comment to John Briffa’s blog on Dec 12, and unfortunately it is still awaiting moderation. Let’s he is back soon.
I received a “round robin” email from Dr. John Briffa late last year apologising for his silence and explaining that he needed a break and also that he and his wife have had a baby and he was giving his time to him/her. Nothing sinister, I hope, though I missed his blogs and was worried by the silence. He hopes to begin again soon, I believe.
I hope that reassures you.
Flyinthesky, when the infamous American comedian, actor and writer, W.C. Fields (1880-1946) was on his death bed, an old friend came to see him. When the friend noted W.C. had a bible on his bedside table, he asked him why since he always claimed to be an atheist. W.C. replied, “I’m a lookin’ fer a loophole.” And I guess that kind of sums it up for a lot of us. LOL Hope you all have a wonderful and happy holiday season, no matter what or who you believe in!!!
Slightly off topic of this latest post….but NOT ot about statins! question.
Just reading Dr. (biophysicist) Gerald Pollack’s latest book “The Fourth Phase of Water” and I’m trying to NOT alarm my-no-longer-taking-statins husband that there may be residual harm from when he did take- but how can I help him recover from ever having taken? Dr Duane Graveline, and Dr Hannah Yoseph have some helpful ideas.
Then BAM!, Doc Pollack mentions the antioxidant enzyme superoxide dismutase- SOD. (first few chapters of his astounding book free for sample download…. I looked into a ‘bioavailable’ supplement from ‘Life Extension, and this article.
http://www.lef.org/magazine/2006/6/report_sod/Page-01
Anyone have experience with the supplement, http://www.lef.org/Vitamins-Supplements/item00961/SODzyme-with-GliSODin-Wolfberry ?
I’m a biochemist, cautious and curious. But the recklessness with which the greedy Big Pharma and statin overlord pushers have dupped, conned and murdered people left and right, if someone responds to this, I may be happily convinced and willing to ‘risk’ the SODzyme supplements! THanks
Laurie, I would not rush to suggest that Pollacks ‘forth phase of water’ idea is nonsense but I did look into it briefly and I just could not dig the concept – by which I mean I could not appreciate the sense in it. We should apply the evolutionary test to most things. Evolution is about adaptation, and the process of selection steers adaptation to suit that which is familiar and commonplace to a point. Species can not become adapted to those eventualities that stand as rare experiences with quite the focus as with those eventualities that are more usual. So, .. ..
.. .. Our hormones struggle to cope with the length of day that results from the invention of the light bulb. This has ramifications for cortisol and insulin.
.. .. Our hormones and hormonal balances can be knocked off axis by the habitual wearing of shoes made of rubber and plastic. (This insulates us from the Earths electrical field and results in a dearth of free-electrons in us.) Earthing can have hormones trend to more normal levels and rhythms.
.. .. And to our physiology the paradigm of a ‘healthy balanced diet’ that is low in fat seems quite out of balance.
If the forth phase of water is rare I struggle to conceive how it was any less rare in the past when the process of adaptation by mutation and natural selection had us trending slowly from primate to human. I however retain an open mind and if you can perceive how I might be missing something of pertinence then please do drop me a line. I could use a steer to help me better appreciate Pollocks radical idea.
Something else.
The acetyl and mevalonate pathway is common to both plants and animals. With molecules of glucose its job is to produce mevalonate, then mevalonate can be reworked into sterols. In one of the later steps an enzyme weaves its magic to sythesise the mevalonate. That enzyme is HMG-CoA reductase, and my early inquiries indicate HMG is a fairly ubiquitous attachment to the the acetyl and mevalonate pathway. That must make HMG-CoA old, very old.
There was once a time before glucose, and in the scheme of things glucose arrived on the scene some time after life on Earth began. Clearly mavalonate arrived later, but when precisely? When did HMG-CoA arrive on the scene? I am prepared to think the order of 2 billion years.
In terms of evolution there must have been the occasion of the first mevalonate .. and following that the occasion of the first sterol. Which was the first sterol, and the second? The family of sterols now extends to about 200 in number. Here in Manchester supporting City or United can divide family members. With sterols it is whether they support plants or animals. There are plant sterols (phytosterols) and zoosterols. When did the first zoosterol arrive on the scene? Cholesterol is an example of a zoosterol. Was cholesterol the first zoosterol? Was the first zoosterol first biosythesised in a plant?
If the basic template for a plant cell and an animal cell is so similar what accounts for the differences? In early multicellular life on Earth where plants predominated what makes for a cell membrane? Is it polysaccharides and lignin in the main?
How did the lipid bilayer that typifies the membranes of the cells of animals arise? These membarbes rely heavily upon the involvement of cholesterol which seems to act a bit like mortar binding structural lipid elements together to form the membrane. What came first, the cholesterol or the membrane?
Could it be that emerging and growing enzymic diversity within life could be responsible for growth in the diversity of the familiy of sterols. The number of mevalonate offspring grew over evolutionary time (?). Would the arrival of increasingly lipophilic sterols have paved the way for cell membranes to trend to becoming more fatty. Might the arrival of zoosterols (or one) in a phyto context facilitate radical trends in membrane composition and might that be one of the trends that paved the way for the emergence of animal life?
So many questions and so few answers. Nonetheless the questions intimate that the ubiquity of cholesterol, essential to all creatures pink and fleshy, ought to inform us that cholesterol must be old (at least as old as all animal life), and by reasoned accounts the mevalonate from which cholesterol is made is even older. Mevalonate and the enzyme HMG-CoA might be about the same age. Stains target HMG-CoA and diminish its effectiveness. Who would still consider statins a good idea?
Despite I cannot pin down provenance precisely ‘the order of 2 billion years’ will do and present me with a great line to put before my doctor, “Don’t you dare think to meddle with my mevalonate!”
If Darwin were alive to day he may have suggested something along these lines. The kind of diversity of species represented in the schema of the tree of life required the emergence of a corresponding diversity and sophistication (evolution) in the underlying biochemistry. Biochemistry runs in families. Biochemistry has an order, not unlike anyones’ family tree.
With reference to Flyinthesky. “The universe started with the big bang declare the scientists proudly, a big bang of what and who lit the fuse?” So well put!
The precise nature and provenance of the big bang is not known. The theory could be wide of the mark. But the notion does time-stamp a beginning of a kind. The beginning does not matter so much as does what happened next. You see in the beginning there was no hydrogen, and there could therefore be no stars, and with no stars there could be no helium, lithium, no carbon, no oxygen, no nitrogen, .. .. no periodic table as such.
The big bang is an uncertainty but the events that followed the bang are less uncertain. Physicists can account for the provenance of hydrogen, then in turn that hydrogen accounts for the provenance of stars, and the life-cycles of stars account for the provenance of the naturally arising chemical elements that populate the periodic table. We are stardust, as the lyric advises, and we’d do better to better understand the engine that powers us all. Evolution is all around, its not just in species, because every event and eventuality that has ever arisen in the last 13.65 million years is spawned of some event or eventuality that came before. Events and eventualities are just like children, they are spawned of ones that came before.
Despite the inadequacies of the big bang theory the notion of the big bang has spawned explanations for the provenance of all that followed; thus lending pertinence to provenance, and accounting for the provenance in pertinence. (Did I really saythat?)
As recently as 150 years ago people thought the year 4554BC (or thereabouts) was the date of creation. Set in context and summarised in a paragraph or two the extent of cognitive advances of late are staggering.
As to the first part of your emminent post, whoosh, never even disturbed a hair on my head as it streaked over it, on the second part, post my reference the essence is the tranference of power and influence. The prevailing religon has to be debased before it can be relpaced with another.
We are at the halfway house position at this moment in time: put your faith in the lord, unless the scientist says different. It’s a power struggle.
Here’s a concept to wrestle with, have we evolved or were we created, ancient alien theory, by entities who were far smarter than we are.There is the enduring anomaly of the missing link.
We have the carbon dating scenario, all points to it’s accuracy, but is it? We don’t have an artifact with a date label on it, is it linear or exponential. We don’t know. It is however expeditous to say we do.
We also have in the frame genetic predispositions, that again is a red herring and not scientifically quantifiable, as well as handing down our genes we also hand down lifestyle and nutritional inclinations. It remains what it is, a power stuggle. What I am convinced of is we know almost nothing about almost everything.
Thank you kindly Flyinthesky…… I continue to look for anomaly and paradigm challenge everywhere. I LOVE the internet and the free flow of kindness, info and ideas. I’m out of it for a bit because my elderly mother-in-law just passed away. But leave you with… There is a dramatic and amazing “TED” talk online of Dr Pollack and his (our) water. I can’t recommend it more highly.
I appreciate your reply, and apologize if I appear radio-silent for a while….Laurie
“What I am convinced of is we know almost nothing about almost everything.”
I absolutely agree with you on this, and recognition of this important actuality ought to be the incentive driving curiosity, but the reality is that in many a person the fear of venturing into unfamiliar territory discourages curiosity as significantly as having ‘faith’ does.
Six questions are of particular and philosophical significance to an intelligent species like the human and yet they rarely receive consideration or attention:
What do we know?
How much do we know?
How much do we not know?
How much of that which we think we know is worthy of improvement?
How much of that which we think we know is in actuality a falsehood worthy of complete replacement?
How much of our behavioural responses and thought are truly rational, and how much is pre-programmed, if you like, and commanded by biochemistry?
I hadn’t realised deployment of intelligence and logical thought in the human, coupled to the relative ease or difficulty of deployment in, and by, individuals of the species, might be resolved by addressing these questions until I read your comment and began thinking about how to respond. Your remarks are truly thought provoking and certain of your seemingly simplest sentences are truly inspired, as was the case with this absolute gem, “The universe started with the big bang declare the scientists proudly, a big bang of what and who lit the fuse?” I am indebted to you, Flyinthesky, and I do not mind lending credit where credit is due. Aspects of your remarks have helped me see things more clearly.
I think those six questions can be answered in a way that can cast light upon the human condition, and hopefully permit some light to enter those who might benefit, to good effect.
And what you say about genetics and predisposition is profound too. I agree predisposition is phenomenon whose frequency and pertinence has been overstated, but I disagree too, for in vivo genetic switching, may give rise to symptoms generally regarded as being ‘unhealthy’. Such propositions deserve further qualification.
I propose to answer online but not commandeer the thread or Dr Kendricks blog, and with his permission I’ll return to submit a link wherein I hope to address some of the issues you raise.
Feel free
I’m sorry Christopher, I didn’t mean to disturb your sensibilities. Good luck with your efforts, I’ve been looking all of my life for answers to a lot of things and so far I have only managed to recognise the questions.
The answers that I’m looking for, that I don’t think I’ll ever find, must comply with two conditions: they mustn’t frighten people, giving rise to all sorts of opportunity and nobody can make a shed load of money out of it.
This the issue I have with most modern scientific endeavours they seem to fall foul of one or other and often both of these conditions. I understand that these things require funding so there is little to no science conducted on an altruistic or human curiosity basis, it all has to have a purpose and the commonality of purpose is either empowerment or enrichment, the net result is it distorts all of it. Even things like CERN someone is looking for an opportunity.
This is the issue with the big bang, it’s a power struggle between two entities religion and science, neither know the answer and neither ever will. But the one with the best and most credible postulation gets the power.
The quest for reality is exponential, the more questions you ask the greater amount of questions you generate, If I can give you a head start the answer to most of them or as near as you’re going to get is 42 !
1) I have answered that to the best of my ability.
2) same answer.
3) All good philosophic stuff but it’s actually a third way of asking the same question.
4) Depends if there are more bucks in it.
5) Depends if there are bucks to be lost by it.
6) Now there’s a question, the answer is probably 42, god/science forbid that we ever understand it, or think we do, because if we did we’d have the overwhelming urge to mess with it and probably break it.
My curiosity and my cynicism don’t make easy bedfellows. but hey…..that’s me.
Flyinthesky
4) Depends if there are more bucks in it.
5) Depends if there are bucks to be lost by it.
As a researcher (and thus a skeptic) of many decades I think that you are absolutely right; the above in particular sums it up. Your philosophy is on track; be skeptical.
Sorry Malcolm, way way of topic.
“Physicists can account for the provenance of hydrogen” Can you? or are you accepting a credible hypothesis by a perceived eminence.
The governments chief medical officer tells us…………. does he know? or is he accepting a credible hypothesis by, here’s a subtle difference, an on message percieved eminence.
In the latter case who generates the message? The government by its’ own volition or a vested interest that claims overall liabiity can be reduced by investing in our products.
It’s the same in most areas, once we say we know X instead of we think X, thinking X and knowing X have totally different power connotations, the latter usually adopted for obvious reasons, once the knowing is expressed, they often don’t “know”, the learning curve is curtailed.
Half of the people that have heart atticks have high cholesterol , half have low cholesterol. To me, that tells it all.
Would not the NNT be better described as the number needlessly treated?
That is one of the sanest comments I have ever read. It is in fact virtually the probability of NO benefit (1 – 1/NNT).
Christopher Palmer
Re Dr Briffas absence.
Had email today from his website saying that he hopes to return to blogging. It will take the form of more occasional posts than he was accustomed to producing as he has recently become a Father to a baby girl!
Let’s hope so, I enjoy his blogs too, and had wondered what had happened to him!
Everything published made a bunmch of sense.
But, what about this? suppose you were to create
a awewsome headline? I mean, I don’t wish to tell you how to run your blog, however what if yyou added a post title to possibly get
people’s attention? I mean What is T? | Dr. Malcolm Kendrick is kinda vanilla.
You might peek at Yahoo’s front page and watch how they write
news titles to get viewers to click. You might addd a video
or a related picture or two to grab people interested about what you’ve
got to say. Just myy opinion, it might bring your
blog a little livelier.
I appreciate your input. I suppose if I had the resources of Yahoo I could make things a bit more zippy. I am thinking about a couple of videos and other stuff. My problem is really time. Working full time, writing clinical papers a book and a blog means that I am somewhat stretched.
Please don’t make them ‘more zippy’ or ‘livelier’ !!! We royally are here for content, not style, and an excess of Style tends to have an effect of making one suspicious and less keen on spending time considering the content.
Not that some sense of humour goes amiss…
Lack of suspicion not being the same as suspension of all critical faculties in this case of course 🙂
Rodolfo,
Sound bites and headlines get far too much exposure and account for how people trend to becoming misinformed while thinking themselves informed.
One step on route to becoming better informed is the realisation that the devil resides in the detail. Many is the book with an uninspiring cover whose content is highly inspiring.
A step on route to wisdom demands a person judges a book upon its content and not on the cover. Many is the book or article I read whose qualities I cannot appreciate on the first read through. Rather than rush to think the books content is at fault I tend to think the faults may lie with my own incapacity to understand the text. That which seemed impenetrable upon the first read through often comes clearer on second, third or even forth read-through.
It is an almost universal human trait that we perceive failings in others more readily than we concede our own, and we squirm when this universal failing is pointed out. We’ll swallow a shed-load of dogma, while rank pragmatism is a bitter pill for anyone to swallow.
Absolutely no offence intended.
Dr Michael Mosley is a journalist and broadcaster whose interests major around diet, lifestyle, and health. He graduated in philosophy, politics and economics, worked in banking, and then elected to venture back to study for a career in medicine, intending to become a psychiatrist. In the event he subsequently joined the BBC to work as a producer, and collaborated on series presented by Professor Robert Winston. So far as I can discern Mosley is not a registered medical practitioner.
Mosley has trended from producer to presenter, and his style is earnestly transparent. He has fronted some features in the Horizon franchise that have looked at diet and exercise. What marks him out as interesting, is that his opinions have evidently altered over time, and when compared to the general conservatism as prevails within medicine his views seem progressive. It’s interesting, I think, to witness a person shifting long held beliefs upon matters, even to the point of outright reversal. Mosley is a person who has reversed his views upon the role of fat in the diet, amongst other things.
Your followers might be interested to learn that a BBC Horizon documentary presented by Mosley, The Truth About Exercise, first broadcast on 28 Feb 2012 is again available for on-demand viewing from iPlayer until around 12 Feb 2015. It might also be available from subscription cloud services such as Amazon Prime. It’s worth taking the opportunity to watch or watch again.
There are ways in which themes raised represent a clash of old school dogma and modern evidence based pragmatism, especially when a young featured doctor discusses blood fats and artery clogging in wholly inadequate old school terms, but other themes are more progressive. Something that was interest to me was mention of an enzyme called liporotein lipase that has bearing upon the metabolism of blood fats. Basically exercise can stimulate production of lipoprotein lipase and more liporptein lipase can significantly alter the % of fat that is in with blood, and this harks to an interesting facet of genetics.
Every living person ought to have the gene (or genes) that can account for the provenance of lipoprotein lipase, but the genes behind its production can be more or less effective. The clue for ‘how’ comes from the notion of genetic switching. Genes can have simple tags attached and the attachment of a tag effectively turns the switch off. The tag is a methyl (or CH3) group. One consequences of taking exercise is that tags may be added or removed from genes as a consequence of that exercise. Exercise can, it may seem, might remove a tag from the gene(s) behind lipoprotein lipase and therefore permit this enzyme to to do the work nature tasked it with. Inclination to be sedentary might encourage conditions whereby the gene is re-methylated and turned off again.
I mention this with a remark of Flyinthesky in mind. Flyinthesky expressed scepticism about health outcomes and ‘genetic predisposition’; the card has been overplayed, perhaps, in medical explanations. I agree.
I agree not because genes are unimportant, but because interest in genetic switching was, and is, one of the fastest reappraisals of scientific expectation and interpretation ever. Switches that can apply to individual genes are an odd mix of those that seem robust and not easily altered, and those that seem quite transient and dynamic. The more dynamic ones, perhaps, might lend an impression that genes are at fault when really it is these switches that are at fault, and they are at fault because certain of our habits might be.
http://www.bbc.co.uk/iplayer/search?q=The%20Truth%20About%20Exercise
Dr. Kendrick,
As a 54 year old male in the US, I was placed on statins for high cholesterol. In recent weeks I have been reading many articles very much inline with yours. My questions is, why hasn’t the mainstream media taken this and ran with it? This sure seems like something 60 Minutes would be all over! In my few weeks of research I have concluded statins do far more damage then good by a wide margin.
Thanks
Bob Williams
A good question
Pingback: Что СМИ не говорят вам об испытаниях Статинов? — Жирная Hизкоуглеводка
Couldn’t agree more?
Pingback: What the Media Isn’t Telling You About Statin Drug Trials | Chris Kresser
Pingback: The Truth about Statin Drugs | Chris Kresser
Pingback: More Truth About Statins- How We Are Being Misled By The Media – Idaho Center for Functional Medicine
Pingback: Cholesterol and the Carnivore Diet - Kevin Stock