Lead
I have been studying cardiovascular disease for well over thirty years now. I have come across a million different hypotheses about what causes it. There is almost no foodstuff, vitamin, infectious agent, chemical compound, atomic element or activity [lack of, or excess] that has not been proposed at some point.
Many of them can look very promising, and the underlying hypothesis is often elegant – very elegant indeed. But what you must do with any hypothesis is to hold it close to the unforgiving flame of mortality data, and see if it is tempered by the heat – or simply melts.
I resolved very early on in my long and winding study on cardiovascular disease that any hypothesis had to explain everything – not just some things. For example, as almost everyone in the entire world knows a raised cholesterol level is considered the most important cause of cardiovascular disease. But it is exceedingly easy to find facts that seem to completely contradict this.
Here, for example, is a little graph looking at only two countries. It compares the death rate from heart disease in Russia and Switzerland, in men under the age of sixty-five relation to the average cholesterol level in those two countries.
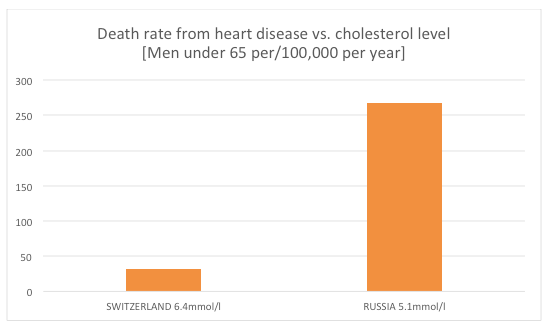
in Russia, with an average cholesterol level of 5.1mmol/l (197mg/dl) had a death rate 834% higher than that in Switzerland, which had an average cholesterol level of 6.4mmol/l (248mg/dl). Yes, this graph is the right way around. Yes, these data come from the World Health Organisation, and can be found on the British Heart Foundation (BHF) website. These particular statistics are now very deeply buried, but can still be found here: https://www.bhf.org.uk/publications/statistics/european-cardiovascular-disease-statistics-2008
I sometimes wonder if anyone at the BHF actually looks at these data, but that is a question for another day. Of course, when presented with facts like this, the dismissals. and creation of ad-hoc hypotheses rapidly reach into the sky. The word ‘paradox’ will be used pretty heavily, that’s always a good, temporary, escape route. In reality these two figures represent a full-blown black swan. But, hey, facts are slippery things.
Anyway, in my quest to explain everything about heart disease, perhaps the hardest single thing to explain is the fact that the rate of cardiovascular disease (heart attacks and strokes) has been going down in pretty much every single Western country for decades. I would say ‘first world’ country, but my son (a geography graduate) informs me that this terminology is now virtually barred for being racist. I shall be considered an ancient, prejudiced reactionary for using such a term.
So, I will say, Western Europe, North American, Australia, Japan, New Zealand and suchlike.
Now, the decline in CVD did not start at the same time, in all these countries. At this point I will make myself a hostage to fortune and make some sweeping statements. The rate of CVD peaked first in the US, in the late 1950s and has been falling since. It peaked next in Finland in the 1960s. In most of the other countries CVD peaked in the 1970s, before falling. It is impossible to say that there was a uniform worldwide effect. [Today, some countries are on the way up the mortality curve e.g. China and India].
However, I will make the general statement that CVD has been falling in most ‘first world’ countries for decades. This started long before any effective medical interventions were available. In the US, in the 1950s, there were no effective blood pressure lowering agents, no stents, no CABG, no clot busters…. Nothing really.
Possibly the greatest single factor has been the reduction in smoking. At the end of the second world war virtually all men smoked. Nearly 90% in the UK in the 1950s. Since that time the number of smokers has fallen, and fallen.
In addition to this, during the 60s, 70s, 80s and onwards, medical interventions have also greatly improved. In-hospital survival from a heart attack or stroke has improved almost year on year. The figures are complex, but around 60% of those admitted to hospital with a heart attack used to die – it is now around 30%, maybe less.
Some of this is due to the fact that ‘strict bed rest’ following a heart attack, the key medical intervention for decades, was abandoned. A piece of medical mismanagement that killed millions and millions… and millions.
What else may have cause the fall? I think that in the UK, the clean air act has a significant effect. The Great Smog of London, in the early 1950s, killed tens of thousands in less than a week. Much of this was from respiratory complications, but also CVD. It is now more clearly established that air pollution, in general, increases the risk of CVD. Most Western countries have drastically reduced air pollution.
Now, I would like to consider something almost never mentioned. Lead. That is the element, not the verb. Or the noun, as in dog lead.
In the 1920s someone discovered that if you put lead in petrol/gasoline it had all sorts of benefits on engine performance and wear and tear – and so on. Unfortunately, lead also caused all sorts of problem for human performance, and wear and tear. It is a heavy metal and, like other heavy metals, a powerful human toxin.
Despite the fact that lead toxicity was known for decades, it took until the nineteen-sixties before countries starting banning it from fuel – and pipes in housing – and the like. Which reversed a long-term trend of lead building up inside human beings. It lasts for decades within bone – gradually leaking out.
With regards to lead and CVD, is there a link?
A researcher called Weisskopf looked at the amount of lead in bones, and the rate of CVD. He found that those with the most lead in their bones were 837% more likely to die from CVD (relative risk)1 than those with the least lead in their bones. Now, whilst that is a relative risk, it is of the magnitude where we can safely say we are looking straight at a direct cause of CVD.
How does lead cause CVD. Most likely through the following mechanisms
‘Lead causes endothelial dysfunction by binding and inhibiting endothelial nitric oxide synthase and decreasing nitric oxide production.’2
Yes, we are straight back to my old friends, endothelial dysfunction and decreased nitric oxide (NO) production. In the world of cardiovascular disease, if you know where to look, all roads lead to NO.
If lead does cause CVD, is there any evidence that removing lead from the body can reduce the risk of CVD? [‘Reversibility’ and ‘Experimental Evidence’, the two most powerful of Bradford Hill’s canons for causation]. Which brings me to TACT. A trial designed to look at the impact of chelation on CVD. A way of removing heavy metals from the body…
What I love about this trial is that it was set up primarily to prove that chelation was nonsense, to be laid alongside homeopathy, and suchlike – by mainstream researchers. To quote an article in Medscape:
‘The original TACT trial wrestled with enrolment, ultimately taking over a decade to yield results, in part because cardiologists were absolutely convinced that chelation was a load of horse hockey.’ 3
TACT stands for Trial to Assess Chelation Therapy. When I first heard about chelation, I too, dismissed it as horse hockey. However, it turns out that I done the thing that I always advise everyone else against doing. I placed it in the ‘impossible/horse hockey’ category without making the effort of trying to find out what it was really about.
As it turns out, I should have made more effort…
‘TACT found that patients randomized to a regimen involving up to 40 separate three-hour infusions of a chelation-therapy solution (disodium ethylenediaminetetraacetic acid [EDTA], ascorbic acid, magnesium chloride, potassium chloride, sodium bicarbonate, B vitamins, procainamide, and a small amount of standard heparin) experienced an 18% drop in the trial’s primary end point (all-cause death, reinfarction, stroke, revascularization, or hospitalization for angina) compared with patients randomized to a placebo infusion.’3
More extraordinary than this:
‘When we broke the composite down to look at our secondary end points, we found that we had about a 40% reduction in total mortality, a 40% reduction in recurrent MI, and about a 50% reduction in mortality [in patients with diabetes],”’3
A 40% – 50% reduction in mortality. Well, well, well. Eat your heart out statins. In fact, eat your heart out every single pharmaceutical product ever tested. What has been the effect on mainstream thinking on CVD? As you would expect, absolutely nothing has changed in the slightest. Still TACT2 is now being set up – so we can all look forward to that being ignored in about seven to ten years’ time.
Anyway, in an attempt to bring some structure to this blog, I am going to return to the start. Why has the rate of CVD gone down in most first world countries over the last fifty years? One of the reasons, I believe, is that the level of heavy metal pollutants (in particular, lead) has been dropping since around the mid nineteen sixties.
I think it could be argued that the US was the first country to embrace the motor car. Thus lead toxicity would have hit the US before anywhere else. I am not going to argue this too strongly, but I place it before you, for your consideration.
I shall finish by saying that, if you want to look for reasons for the pattern on CVD over the last sixty years, or so, you really need to start looking outside the box. For there are more things in heaven and earth Horatio, than are dreamt of in your philosophy.
1: Weisskopf MG, Jain N, Nie H, et al. ‘A prospective study of bone lead concentration and death from all causes, cardiovascular diseases, and cancer in the Department of Veterans Affairs Normative Aging Study’. Circulation 2009;120(12):1056-64.
2: Natalia V. Solenkova et al: ‘Metal pollutants and cardiovascular disease: Mechanisms and consequences of exposure.‘ Am Heart J 2014;168:812-22
3: http://www.medscape.com/viewarticle/814643?pa=QYKVfN05tfWXqq6%2BfjZ30whyKyHVDGvMW4WYyHO8jprcrUBo6WRIR4VFzOaThtqB8SIvl8zjYv73GUyW5rsbWA%3D%3D

