I am a GP living in Macclesfield, having graduated from Aberdeen medical school many moons ago. This blog is my best effort at providing some balance to the increasingly strident healthcare lobby that seems intent on scaring everyone about almost everything. Is there a foodstuff that is safe to eat anymore? Is there any activity that does not cause cancer or heart disease? Sausages…..get thee behind me Satan.
As regular readers will know, Zoë Harcombe and I sued the Mail on Sunday (Associated Newspapers) and Barney Calman for libel. This is a saga that began over five years ago. Which has explained much of my recent silence on this blog, following a hearing in July last year.
“Before turning to the remaining issues, I should repeat that the exercise of determining the objective single natural and ordinary meaning of the Articles, and whether the Articles are or contain allegations of fact and/or expressions of opinion is wholly different and distinct from the assessment of Mr Calman’s subjective assessment of the meanings that the Articles bore (see [247] above). I have necessarily had to deal with many issues, in great detail, in the earlier part of this judgment. I put all of that to one side. Save for necessarily identifying those passages of the Articles that I have found to be privileged (or are agreed by the parties to be privilege) for the purposes of Curistan, the resolution of these other issues has no bearing on the objective assessment of the natural and ordinary meaning of the Articles and fact/opinion. In that respect, my task in the next part of the judgment is to apply the well-established principles as set out in G(5) ([380]-[387] above).”
Much of the judgement is rather similar. So, unless you suffer from insomnia, I would not recommend it as a cracking read. However, there are some gems to be found.
You may ask, and many have, why did you go ahead with this case. It was risky, costly, and you might lose. And, in the end, it will pass. People will forget it was ever written. Today’s news is tomorrow’s fish and chip supper wrapping.
Well, maybe. I think Judge Nicklin summed up what he felt were the main messages in the articles we complained about. This passage. Paragraph 254.
‘…the presentation of these articles, as a whole, reinforced this message. The “devastating investigation” exposed the “fake news” by “unequivocal science”. The “‘fake claims’ about proven medicines”, amounted to “deadly propaganda”, a “wanton spread of medical misinformation”, and a “vastly overstated” case by the “statin deniers”. The science showed that “none of which is right” and was contradicted by “researchers who have devoted their lives to understanding how to treat heart disease” and who had produced “the highest quality scientific evidence on the subject”. The “pernicious lies” of the ‘statin deniers’ “needlessly risked lives”, and damage to public health, that was “worse than the MMR scare”.
Essentially, in his finding about meaning [para 516], Judge Nicklin basically made clear we were accused of being pernicious liars spreading deadly propaganda – suspected to be for our own venal reasons. We had, potentially, killed many thousands. Someone did say to me ‘At least you weren’t accused of being a paedophile.’ This did not go down well with me.
‘So, killing thousands is better than being a paedophile, really?’
I consider that to be blamed for killing thousands is the worst possible accusation you can make against anyone, especially a doctor. Not only that, but the articles directly implied we were only doing this– in order to make money. Does it get worse. Can it possibly be worse?
Well, it could have been worse in that I could have been struck off, and not allowed to practise medicine ever again. After all, if what I did was ‘worse’ than the MMR scare, and we all know what happened to Andrew Wakefield who was struck off and can no longer work as a doctor. I have been waiting for the letter from the General Medical Council to drop through my letterbox for over five years now. So far, nothing.
In essence I could not possibly let this go, and nor could Zoë.
Where are we now? The initial judgement has been made, but the defendants (Associated Newspapers and Barney Calman) have indicated they intend to seek permission to appeal. And the appeals process can go on, and on. Ending up at an appeals court. Will the appeal be successful. I have no idea. Will they give in and accept the judgement. I hope so. I hope others can understand that if you are accused of killing thousands, simply in order to make money for yourself, then you really have to take a stand. If not, what?
In the case against the Mail on Sunday (Associated Newspapers) and Barney Calman, Health Editor of the Mail on Sunday.
I have written nothing on this blog for a while, because of my on-going legal case. Now we have a judgment, part one.
Step backwards for a moment. Zoë Harcombe and I are suing the Mail on Sunday and Barney Calman for libel. This goes way back to March 2019, yes over five years. The Mail on Sunday published article(s) that we felt were very damaging and defamatory.
In short, we were effectively accused of being liars, and ‘purveyors of misinformation’ about statins (drugs that lower LDL/cholesterol). Because of our lies hundreds of thousands of people had stopped taking statins, resulting in (potentially) many thousands of heart attacks, strokes and deaths. Which, as a doctor, is the worst ‘crime’ it is possible to be accused of.
There was much discussion, in the articles, of this being far worse that the MMR scandal involving Andrew Wakefield. You may remember that he was stuck off as a doctor for his papers and articles on the MMR vaccine. This could obviously have happened to me. If what I did was worse. This threat has hung over me for over five years.
In his judgment I think that the following statement was the most powerful
There is perhaps a palpable irony in the fact the Defendants, in Articles that so roundly denounced those alleged to be the purveyors of misinformation, so seriously misinformed their own readers
The Judge has basically ruled that the Mail on Sunday misinformed its own readers. And as he also said.
I have found that Mr Calman did not believe that the Claimants were dishonest, yet this is the core allegation that the Articles made against them, as Mr Calman must have known (or a reasonable journalist in his position would inevitably have realised).
We were not dishonest, yet Barney Calman wrote articles where the core allegation is that we were. I will write more on this issue over the next few weeks and months. The legal issues were ridiculously complicated and so I include my lawyers’ statement below, which explains a bit more as well as a link to the judgment itself. The full judgment – all 255 pages of it – can be seen here.
High Court dismisses Mail on Sunday’s public interest defence in “statin deniers” libel case
In a major Judgment delivered on 25 June 2024, Mr Justice Nicklin has dismissed a public interest defence advanced by The Mail on Sunday in a libel claim brought by Dr Zoë Harcombe and Dr Malcolm Kendrick. The decision follows a preliminary trial last year in what the Judge described as “the most significant piece of defamation litigation” that he had seen in a very long time.
The case relates to articles published in March 2019, which contained allegations that the Claimants had made knowingly false statements about the cholesterol-lowering drug, statins, causing a large number of people not to take prescribed statin medication with the harm to public health that flows from this (allegations which Dr Harcombe and Dr Kendrick assert are both highly defamatory and false). The Mail on Sunday refused to apologise or even remove or alter its articles. The Claimants therefore issued High Court proceedings in February 2020.
Dismissing the newspaper’s public interest defence, the Judge observed (at paragraph [457]) of his judgment) that:
“There is perhaps a palpable irony in the fact the Defendants, in Articles that so roundly denounced those alleged to be the purveyors of misinformation, so seriously misinformed their own readers.”
The case will now move on to its next phase, as the Court was not at this stage adjudicating on other aspects of the case such as the Truth defence which the Mail on Sunday is attempting to put forward, albeit the Court’s findings mean that the Defence as currently formulated, and subject to any appeal, “cannot be maintained” [562].
Dr Harcombe PhD, a writer and speaker on diet health and nutritional science, has said of the judgment:
“I am delighted by the findings of the court today, in what is a hugely complex case. I am grateful to the Judge for his detailed and careful analysis of all of the facts and pleased that he has recognised the enormity and unfairness of the public attack on our integrity.”
Dr Kendrick, a General Practitioner and author with a special interest in the epidemiology of cardiovascular disease, said:
“I am very pleased that the Judge has found in our favour, and that he has dismissed the public interest defence. It was always our position that we had not been treated fairly by the publishers, and the Judgment sets out clearly how badly we were in fact treated.”
Dr Harcombe and Dr Kendrick are represented by Claire Gill and Dominic Garner of Carter-Ruck, and by Adrienne Page KC and Godwin Busuttil of 5RB.
Links
I have been silent and off-line for a while. I am not unwell, but thanks for asking. There is a court case coming up in the High Court in London on the 3rd of July. I am suing the Mail on Sunday, along with Zoe Harcombe. This is complex and highly time-consuming case, and there are many sensitive issues on the line.
It was reported in the BMJ last year:
The controversy over the benefits of statins is set to be aired in the High Court in London, in what the senior libel judge has described as the “most significant piece of defamation litigation that I have seen in a very long time.”
Mr Justice Nicklin made the comment in a preliminary ruling in a libel action by Malcolm Kendrick, a GP, and Zoe Harcombe, a researcher, author, and blogger with a PhD in public health nutrition, against Associated Newspapers, publishers of the Mail on Sunday and Mail Online, over articles that labelled them “statin deniers” whose “deadly propaganda” had endangered lives.
In the judgment Nicklin ordered that the case should be heard in two tranches: a preliminary trial of certain issues, followed by a main trial. “It is no exaggeration to say that the parameters of this litigation are very substantial,” he said.
Kendrick and Harcombe are suing over articles published in the print edition of the Mail on Sunday and in Mail Online in March 2019. A news story in the paper was headlined “Statin deniers are putting patients at risk says Minister.”
Dr Zoë Harcombe and Dr Malcolm Kendrick have brought libel proceedings against both the publisher of The Mail on Sunday and the newspaper’s Health Editor, Barney Calman, over a series of articles first published in March 2019 in the news and health section. Dr Harcombe and Dr Kendrick complain that the Mail on Sunday made a series of libellous allegations, attacking their professional integrity with reference to their public statements and writings concerning the use and efficacy of statin therapy. Due to the unusual complexity of the case, it has been split into two trials. At a trial in July (Trial 1) , the court will decide, among other central issues, the meaning of the articles of which complaint is made, whether they were an expression of opinion by Mr Calman or a statement of fact and whether the defendants are entitled to rely on a public interest defence. The court at Trial 1 will not have to determine the truth or otherwise of the published allegations, and the question of what the defendants have to prove to be true, and whether they can defend their statements as expressions of opinion will depend on the outcome of Trial 1. The focus is on what was said by Mr Calman about the claimants and whether that can be defended.
Please note that comments have been disabled as this is an ongoing case.
With the resignation of Jacinda Ardern, my thoughts were dragged back to Covid once more. Jacinda, as Prime Minster of New Zealand was the ultimate lockdown enforcer. She was feted round the world for her iron will, but I was not a fan, to put it mildly. Whenever I heard her speak, it brought to mind one of my most favourite quotes:
‘Of all tyrannies, a tyranny sincerely exercised for the good of its victims may be the most oppressive. It would be better to live under robber barons than under omnipotent moral busybodies. The robber baron’s cruelty may sometimes sleep, his cupidity may at some point be satiated; but those who torment us for our own good will torment us without end for they do so with the approval of their own conscience.’ C.S. Lewis
At one point she actually said the following:
“We will continue to be your single source of truth” “Unless you hear it from us, it is not the truth.’
If I ruled the world, anyone who said, that, or anything remotely like that, would be taken as far as possible from any position of power, never to be allowed anywhere near it again. Ever.
Yet, there are still many who believe her to have been a great and caring leader. She certainly hugged a lot of people with that well rehearsed pained/caring expression on her face.
Enough of that particular woman. But it got me thinking about lockdowns again and the whole worldwide madness of Covid. This was a time of such blundering idiocy that I find increasingly difficult to believe it ever happened. A bad dream.
‘The sky is falling, the sky is falling…’ Cue, everyone running about in panic. People, allegedly, dropping dead on the streets. Mortuaries, allegedly, overflowing. Freezer lorries, allegedly, stacked with dead bodies. Bring out your dead!
I worked with doctors who strode around the wards in positive pressure protective gear. There were GPs who simply refused to visit elderly residents in nursing homes. On my patch this was all GPs and all nursing homes. Meanwhile I happily visited away with a mask stuck to the top of my head.
During the Covid pandemic I travelled far past angry, to reach a point of utter weariness. Instead of becoming outraged by the latest rubbish that was being pronounced, I very nearly washed my hands of it. However, after learning of Jacinda’s resignation I roused myself to have another look at what actually did happen. Or to be more specific, what was the impact of Covid on overall mortality. The only outcome that really matters.
Rid your mind of the numbers claimed to have died of Covid. The, never to be clarified distinction between those who died ‘of’ or ‘with’ Covid. Or those who read an article on Covid and then, overwhelmed with fear, stepped out in front of a bus. Thus, becoming a Covid related…associated, something, anything to do with Covid, death.
Over time the Covid figures became so ridiculous and unreliable as to become meaningless. I should know, I wrote some of the death certificates myself. Let me think… ‘She died of COVID, she died of COVID not. Eeny, meeny, miney mo…’
I am not saying that Covid did not kill a large number of people. But the fact that deaths from influenza disappeared completely for two years tells me all I need to know. ‘Roll up, roll up, Ladies and Gentlemen, to see the amazing lady influenza disappear before your very eyes.’ An astonishing trick, all the way from La La Land. ‘You expect me to believe that? Ho, ho, ho, very funny….Oh, sorry, you actually do.’
Anyway, to clear my internal database of horribly unreliable figures, I went back to look at my favourite graphs on EuroMOMO. This website looks at overall mortality, and only overall mortality. Their data comes from countries who do know how to record deaths, honestly. Unlike some others, who shall be nameless … China.
However, the main reason to focus on EuroMOMO is that overall mortality is something you cannot fake. About the only thing you can do to manipulate the figures is hold back data for a month or two – which has been done, but not to any great degree. So, without further ado, let us move onto EuroMOMO. Below is a recent graph. I have deliberately removed most of the information you need to know what it is showing. I wanted people to avoid jumping to conclusions … that they might then find it difficult row back from.
I found myself examining this graph idly and thought. Imagine if you had no idea what you were looking at here. What would you think? It’s a squiggly line, yes. Very good, gold star. What else?
To give you a bit more detail. This is a graph of overall mortality, across a large number of European countries. All of those who provide data to the EuroMOMO database anyway. Norway, the ultimate European lockdown champion, has mysteriously disappeared from the database. Maybe they shall return …. I have begun to see everything as a conspiracy nowadays.
The graph itself begins in January 2017 and finishes in January 2023. As you can see (if not terribly clearly) there are two wavy dotted lines. These lines rise up in the winter, and then fall back down in the summer. Something seen every year. This is because, every year, more people die in the winter than in the summer.
Everyone thinks they know the reason for this winter summer effect, but I am not so sure they do. But that is an enormously complicated topic for another time.
The lower, dotted lines represent the ‘average’ mortality you would expect to see [with upper and lower ‘normal’ limits] year on year. Above those wavy dotted lines sits a solid spikey line. This represents the actual number of deaths that occurred. Not just from Covid, but from everything.
This does raise an immediate question. If we keep seeing more deaths than we would expect in the winter, year on year, then the ‘average’ number of deaths should rise? Thus, the wavy dotted lines ought to be going up and up, in the winter. But they don’t.
I am not entirely sure why this is not the case. But it is a statistical question of such mind-boggling complexity that I am, frankly, unable to answer it. I have looked into it, but I was scared off by the sheer scale and difficulty of the mathematics involved. Too many equations for my poor wee brain.
Anyway, this graph starts in the winter of 2017 and ends about now. The vertical lines are drawn at midnight on Dec 31st each year. Which means that we have almost exactly six years of data. Excellent data, not manipulated in any way. I say this because, whilst the diagnosis of ‘Covid death’ may be disputed, the diagnosis of death cannot.
What stands out? Well, there was a very sharp peak of deaths in early 2020. This, as you have probably worked out, was when Covid first hit. I find it fascinating that it was so transient. It came, it went…gone. For a bit anyway.
Was the precipitous fall due to strict lockdowns? Some will doubtless argue this. However, we all locked down again in autumn 2020 and the death rate went up, and stayed up, for about six months. Until, that is, January came along, and it all settled down again. Which follows pretty much the pattern of 2017, 2108 and 2019. And the pattern of all pandemics. They come, and they go. Some a little earlier, some a little later.
What else do you see – now that we are all pretty much fully vaccinated? I think another thing that stands out is the sudden and sharp rise in mortality in November 2022. Which is virtually identical to the spike in 2020. Strange?
However, to my mind, the thing that shouts most loudly about this graph is that the years of Covid pandemic panic really do not look that much different from the previous three years. Half close your eyes, and there is almost nothing to see. The Covid peaks were a little higher, and a little longer – maybe.
If you knew nothing about the Covid pandemic I don’t think you would exclaim. ‘My God, look at these vast waves of death in 2020, 2021. What amazing, never seen before thing, happened here?’ Yes, first spike of early 2020 was certainly sharp, and unusual, but it was short. And very little different to the spike at the end of 2022. As for the rest?
Now, I would like to turn your attention to Germany. The most populous country in Europe. Here it is even more clear that the years of the Covid pandemic are not remotely unusual. If I had removed the calendar years off this graph, you would be hard pressed to spot the Covid pandemic. In truth, you would be more than hard pressed. You couldn’t.
The 2018 influenza spike was equally dramatic to Covid peak of 2021, if not more so. [You may have noticed that there was no peak in 2020] In addition, at the end of 2022, we have the highest peak of all. Future historians might well look at this graph and ask. ‘Tell me, why did the world go mad in 2020, and remain mad through 2021? Why did everyone lockdown in March 2020, and then do nothing whatsoever in December 2022?’
It almost goes without saying that, had we locked down again in November 2022, it would have been claimed that lockdown saved us all. Look at how quickly it came, then went. Well, they could have claimed it. But we didn’t lock down again, did we? In direct contrast to Germany. What of the people living in Luxembourg?
Luxembourg is surrounded by Belgium France and Germany. People move freely from one to the other, always have done, and still do. The ‘deadly’ Covid pandemic raged all around them. Here, absolutely nothing happened. Mind you, they also seem to have been unaffected by influenza.
Whilst the Germans were dying in large numbers in 2018, the Luxembourgians carried on serenely, not an extra death to be seen. Why? Discuss. [It seems that most/all countries unaffected by Covid, were also unaffected by earlier flu epidemics].
I know some of you may be thinking that Germany is much bigger than Luxembourg so … so what? If you are going to see an effect on mortality, you are more likely to see it happen, more dramatically, and rapidly, in a country with fewer people.
I should explain that the figures on the left axis, on the German and Luxembourg graphs (unlike the first one), do not represent total deaths, they are the ‘Z score’. That is, the deviation from the mean.
The upper dotted line represents a Z score of five. That means, five standard deviations above the mean. It has been decreed that if you hit more than five standard deviations above the mean, for any length of time, this is a signal that ‘something bad’ is happening. The alarm starts goes off, and epidemiologists run around bumping into each other. ‘The sky is falling… etc.’
If you use the Z score it makes no difference how large the population is. It has been specifically designed to make it possible to compare changes in overall mortality, in populations of very different sizes. I feel the need here to make it clear that Luxembourg is not that small. It has more than twice the population of Iceland, for example.
Enough of the maths already.
So, deep breath, and trying to bring all these random thoughts together. What does EuroMOMO tell us? It tells us that Covid was a bit worse than a bad flu season, with 2018 being a good reference point. [There have been far worse flu epidemics than 2018, and I am not talking about 1918/19].
What EuroMOMO makes most clear, at least to me, is that Covid was not, repeat not, a pandemic of unique power, and destructiveness. It could have never have remotely justified the drastic actions that were taken to combat it.
Belatedly, this is becoming recognised, as has the damage associated with lockdowns. Here is the abstract of an article from 2022. A bit dry, but worth a read. ‘Are Lockdowns Effective in Managing Pandemics?’
‘The present coronavirus crisis caused a major worldwide disruption which has not been experienced for decades. The lockdown-based crisis management was implemented by nearly all the countries, and studies confirming lockdown effectiveness can be found alongside the studies questioning it.
In this work, we performed a narrative review of the works studying the above effectiveness, as well as the historic experience of previous pandemics and risk-benefit analysis based on the connection of health and wealth. Our aim was to learn lessons and analyze ways to improve the management of similar events in the future.
The comparative analysis of different countries showed that the assumption of lockdowns’ effectiveness cannot be supported by evidence—neither regarding the present COVID-19 pandemic, nor regarding the 1918–1920 Spanish Flu and other less-severe pandemics in the past.
The price tag of lockdowns in terms of public health is high: by using the known connection between health and wealth, we estimate that lockdowns may claim 20 times more life years than they save. It is suggested therefore that a thorough cost-benefit analysis should be performed before imposing any lockdown for either COVID-19 or any future pandemic.’1
In the face of such evidence, the argument for lockdown seems to be transforming into a somewhat pathetic whinge. ‘We didn’t know. It’s all very well people saying we shouldn’t have locked down now. We didn’t hear you saying it at the time. We were just following The Science, don’t blame us. Better safe than sorry. Don’t blame us …I think you’re being very nasty to us.’
This, of course, is nonsense. There were plenty of scientists arguing against lockdown at the time. However, they were all ruthlessly censored, attacked, and silenced. Experts such as Prof. John Ioannidis, Prof. Karol Sikora, Prof. Sunetra Gupta, Prof. Carl Heneghan. These last two UK professors argued very strenuously against lockdowns. They were ignored, then vilified. Here from an article written in January 2021:
‘…Sunetra Gupta. She’s been getting flak from the mob for months but it reached a crescendo yesterday when she was on the Today programme. Why is the BBC giving space to a nutter, people asked? She isn’t a nutter, of course. She’s an infectious disease epidemiologist at Oxford University. But she bristles against the COVID consensus and that makes her a bad person, virtually a witch, in the eyes of the zealous protectors of COVID orthodoxy. Professor Gupta has written about the barrage of abuse she receives via email. ‘Evil’, they call her.’
‘…her chief crime, judging from the hysterical commentary about her, is that she is critical of harsh lockdowns. She is a founder of the Great Barrington Declaration, which proposes that instead of locking down the whole of society we should shield the elderly and the vulnerable while allowing other people to carry on pretty much as normal. It is this perfectly legitimate discussion of a social and political question — the question of lockdown — that has earned Gupta the most ire.’ 2
I would like to point out that I was arguing against lockdown, right from the very beginning. Yes, I do enjoy saying, ‘I told you so’ from time to time. It is one of the few satisfactions I get in life nowadays. Here is a section from a blog I wrote in March 2020. Once again, right from the start:
‘…However, there is also a health downside associated with our current approach. Many people are also going to suffer and die, because of the actions we are currently taking. On the BBC, a man with cancer was being interviewed. Due to the shutdown, his operation is being put back by several months – at least. Others with cancer will not be getting treatment. The level of worry and anxiety will be massive.
Hip replacements are also being postponed and other, hugely beneficial interventions are not being done. Those with heart disease and diabetes will not be treated. Elderly people, with no support, may simply die of starvation in their own homes. Jobs will be lost, companies are going bust, suicides will go up. Psychosocial stress will be immense.
In my role, working in Out of Hours, we are being asked to watch out for abuse in the home. Because we know that children will now be more at risk, trapped in their houses. Also, partners will suffer greater physical abuse, stuck in the home, unable to get out. Not much fun.
Which means that we are certainly not looking at a zero-sum game here, where every case of COVID prevented, or treated, is one less death. There is a health cost.
There is also the impact of economic damage, which can be immense. I studied what happened in Russia, following the breakup of the Soviet Union, and the economic and social chaos that ensued. There was a massive spike in premature deaths.
In men, life expectancy fell by almost seven years, over a two to three-year period. A seven-year loss of life expectancy in seventy million men, is forty-nine million QALYs worth. It is certainly a far greater health disaster than COVID can possibly create…’ 3
And lo, the damage is coming to pass. Maybe not so many people dying of starvation as I predicted, at least not in the West. In poorer countries, however …
Another terrible thing that happened during lockdown was the vilification of anyone who dared question the official narrative. Yet almost everything they predicted has come true. Have the likes of Professor Gupta been forgiven and welcomed back into the fold? Have a wild guess on that one.
What of those who deliberately whipped up the panic and led the dreadful behavioural psychology teams. They quite deliberately frothed the population into a state of terror. What of those, whose ridiculous models kicked the whole damned thing off? The Professor Neil Fergusons of this land? Yes, you.
These people are all still comfortably ensconced, advising away. Their positions fully secure. In the UK they were mostly given knighthoods, damehoods, and other shiny gongs to impress their friends with. This, I find hard to swallow.
More worrying is that there will never be an honest review on the pandemic. Why, because so many people in positions of power would be seriously threatened by it. Which means that any such review will end up as a completely bland whitewash. ‘In general the actions taken were reasonable, and in a situation where so much was unknown, it was better to try and protect the public … blah, blah.’ Case closed.
The reality is that these lockdowns were a complete disaster. A complete disaster. The fact that we will never have a proper debate about them, means that we will learn nothing from what happened. This, in turn, means that another disaster is on the way. Those who should be listened to will be attacked, silenced and censored, again.
Those who got it all horribly wrong last time will be handed even greater powers … next time. The reason why lockdowns did not work, they will argue, is because they were not strict enough, or long enough. We need proper lockdowns next time. You have been warned. Cast your eyes over China.
I will leave you with the conclusion of the paper ‘Are lockdowns effective in managing pandemics?’
Neither previous pandemics nor COVID19 provide clear evidence that lockdowns help to prevent death in pandemic
Lockdowns are associated with a considerable human cost. Even if somewhat effective in preventing COVID19 death, they probably cause far more extensive (an order of magnitude or more) loss of life
A thorough risk-benefit analysis must be performed before imposing any lockdown in future.
Which can probably be summed in in the words: Primum non nocere. First, do no harm.
The central guiding principle of medicine that was hurled out of the window in March 2020 by people who seem not to exhibit a scrap of humility, or humanity. Nor apology.
Ivor Cummins and me, and our part in Big Pharma’s downfall…
Ivor Cummins and Mark Felsted are running another conference looking at the causes of cardiovascular disease. I shall be speaking and presenting a few more thoughts. For example, why has the rate of CVD shot up in the last eighteen months? Possibly explanations? I hope you can attend, and you will all hopefully learn something new, and help us in our endless quest to derail the big pharma leviathan – or perhaps scratch the wing mirrors slightly.
As a change in direction, I thought I would share a short story I wrote. This was an entry to the New England Journal of Medicine competition. This one under the theme “A patient who presented too late”. It did not win, but I thought some of the readers of this blog may like it.
THE REASON WHY
The ewe was suffering, lying on its side, its bleat reduced to a painful gasp. ‘It’s nae coming out father.’ Annie wiped the blood down her trouser leg.
He hurled his shovel to the ground in a rage. ‘Whit have you done wrong this time!’
‘Nothing I…’ She stumbled away from him as he hauled open the entrance to the pen. He glared down at the sheep, struggling to give birth. ‘We lose another one, and I’m telling ye.’ He bent down to examine it. ‘Wrong way round. How could you no’ see that?’
‘I…should we call the vet?’
‘Vet!’ He looked ready to explode. ‘Do you ken how much a vet costs… do you?’
‘But it’ll die.’
‘It’s nae worth anything.’
‘It’s… I don’t know.’ Her shoulders slumped.
‘Oh, poor wee Annie disnae want to see the ewe die.’
Annie touched her own stomach lightly, tenderly. ‘No, I.’
‘Get the gun.’
‘Can you no just get it out, please… father?’
‘Dinnae be an idiot.’ His voice was a club. ‘Gun, now. You shoot it, and skin it. We freeze it and eat it ourselves.’
She stumbled out of the barn, into a fierce wind. Rain and sleet blowing down from the North, falling in sheets from heavy dark clouds. The hills above were now laced with wet snow. The courtyard glistening, moss covered, slippery. The house was freezing inside. The gun in a cupboard below the stairs.
She pulled it out and made her way back to the kitchen. For a moment she held the gun up, squinting through the sights. She could make out her father’s angry back through the dirty window. He turned, and for a moment, it was as though he were staring straight at her. But she knew he wouldn’t be able to see her, standing alone within a darkened room … Watching, heart beating too fast.
‘Hey Annie.’ Arthur was striding along a path beside the field. The sun was high, it was a lovely day, with small flowers studded amongst the grass. Below her the Cromarty Firth shone like a steel plate, as the sea cleaved the hills on either side. A lark was singing frantically above her, hovering high, a fluttering dot. She loved the early summer up here.
She was in a t-shirt and jeans, trying to fix the tap that fed a trough for the cattle. It was old, rusted, they badly needed a new one. Her fingers were already cut in several places.
‘Hello Arthur.’ She didn’t look up, but she knew he was studying her with interest. She pulled the t-shirt more closely round her neck.
‘Do you need a hand?’ He worked at the farm next door. She had watched him from a distance. Driving the tractor, chatting with other workers, talking to his cows. Yelling at them. Kicking them when they wouldn’t move, then laughing. At night, sometimes, she thought about him.
‘Just look at you.’ He had come up close. He took one of her hands in his, examining it with care. ‘What are you doing to yourself?’
‘The tap needed fixed.’ She allowed her hand to rest in his.
‘That piece o’ rusting rubbish?’ He laughed. ‘You’ll no fix that. You need a new one.’
‘Father says we cannae afford it.’
‘Aye… well I’m sure he did. I’m sure he did.’ For once, there was no trace of humour in his voice. ‘What about you Annie?’
‘Whit do you mean?’ She flushed.
‘Up here, by yourself, stuck wi’ your gloomy dad. What does Annie do?’
‘I work…’ She glanced round, making sure her father was nowhere nearby, watching. ‘The farm needs me, after mother died.’
‘I hear you have a brother. Big lad.’
‘Aye, but he… he left. He hasnae been back for years now. He works in the big city.’
‘What, Inverness. Aye, the great big city. Even got a MacDonald’s, might just be the centre of the World. Mind, he could walk back in a day… if he wanted.’
‘Well, I don’t know.’ She had no idea what to say next. She wasn’t good at conversations. She didn’t have many. An awkward chat about the weather over a cup of tea, down at the kirk on a Sunday. A half-hearted promise to visit from one of her mother’s old friends. Nobody really wanted to come to the farm anymore.
‘A bonnie lass like you.’ He touched her shoulder lightly. For a moment she allowed herself to lean in towards him.
‘No…No. I cannae stay.’ She leapt up.
‘Hey, hey up Annie. I didnae do anything.’
‘I …I have to go!’ She gathered her things together furiously into a leather bag, then almost ran up the road. Arthur watched her. He always noticed when she was in the fields. Working the dogs, driving the tractor, hair blowing in the wind like some Pictish warrior queen. That long vanished race who once roamed these lands. She always looked to be concentrating furiously, passionately, on everything she did. She made him feel alive, and awkward, like a wee boy…
…This night, the pain was worse than ever, grabbing at her stomach fiercely. Her periods had almost stopped and… and she reached down to touch her stomach. It was definitely growing. ‘You’re getting fat. I cannae have you slowing down, not now.’ Her father had snapped.
How she wished her mother was with her to offer some comfort and kindness. After she died, her father had become so different. Angry, shouting, red faced. He would be sitting slumped in front of the coal fire now, whisky bottle close to hand, no doubt. Staring at the flames.
Sometimes though. Sometimes he came to her room, and he was different then. She reached down to scratch the head of her Bramble, her collie dog. Bramble licked her hand.
‘Whit can I do lassie.’ Annie looked down into Bramble’s adoring eyes. ‘Whit can I do.’ She closed her eyes tightly as the pain caught at her again. She wondered about going to the doctor. Then she thought about her father finding out. What if it was a child… what if it was a child?’ The thought filled her with desperate longing, and terror. She knew you could get tests, but…
‘How many this morning.’ I felt the need for an early finish. It had been an unrelenting week.
‘Sixteen, the usual.’ Jill, the receptionist, brought my list up on her screen. I was the on-call doctor, starting early.
Five regulars, who were all depressingly regular in their visits and vague, never ending, untreatable complaints. ‘Who’s that first one, never seen her before. Anne Pierce? You know her?’ Jill had been born and brought up locally, she always seemed to know everyone, and everything about them. Mother to every waif and stray.
‘That’s her, she was waiting when I opened the door. Arthur Mackenzie brought her down, I saw him in the car, pretending he wasn’t watching.’ Jill kept her voice low and nodded towards the only patient in the waiting room. Hands gripped together; head down, staring at the floor. Hair dragged back a painfully tight bun. ‘She lives with her father on High Range farm, poor lass.’
‘Poor lass? Tell me more.’
‘Her father is…’ Jill flushed.
‘He is, what? Is this the secret service?’ I whispered into her ear.
Jill giggled. ‘Not very nice.’ I knew she would say nothing more. Miss confidentiality. Even though I was the doctor.
‘Well, if she’s a farmer, it must be something serious.’ Famers were notorious for putting up with anything. Bone broken after a fall… ‘Just a wee break, strapped a couple of bits of wood round it, hurts a bit when I walk.’ Or coughing up blood. ‘Just a wee cough, had it three years. Took some of the antibiotics we use for the cattle. Thought it would clear up doc.’ Yes, well, everything clears up when you’re in a coffin.
Annie had entered the room without meeting my eye. Her history had been simple. Abdominal pain, a bit of swelling. No periods. The pregnancy test I gave her to do was negative. She had been jumpy, wary, an injured bird. I watched the silent spasm of pain on her face as she got up on the couch.
Her abdomen was certainly enlarged, but it didn’t seem like any pregnancy I had seen before. I put my hand on and pressed down. It was like pushing on a car tyre. Hard, very hard. I tried to find an edge, but there was none. A mass was literally filling her abdomen. It must have been the size of a pillow. This was one of the few times when I had absolutely no idea what to say to a patient.
‘Are you okay doctor.’ My attempt to hide my emotions had failed completely. She seemed more concerned about me than her.
‘Yes, yes, thanks. But I think we may need to get you looked at.’
For those of you who are regular readers of my blog, you may have noted little activity recently. I found myself diagnosed with prostate cancer, and then radiotherapy, and anti-androgens, then in the midst of that I went down with COVID19. So, energy levels have been a little low. Particularly my ability to concentrate on writing, anything of great value.
I am going to give it a month, or so, to see how I feel. Then, I hope to be back on-line after that. I wil get back to approving comments this week. Thank you.
The COVID19 pandemic has thrown an issue into sharp focus that I have been observing for many years now. What is an expert? The simple answer is someone who has expertise. Deep knowledge of a subject that has been gained by spending many years researching, reading, speaking to colleagues, and suchlike.
However, that is clearly not enough. I have spent years researching cardiovascular disease. I have written papers about it, written books, given lectures… but I have never been referred to, by any in mainstream medical research at least, as an ‘expert’. I am very much something else. A maverick, a denier, zealot a … [insert insult of choice here].
I used to joke that there must be a secret expert exam that you have to pass in order to be called an expert. Or perhaps it’s a bit like the Freemasons. Someone has a quiet word in your ear to sound you out. Then asks if you would like to join the international brotherhood of ‘experts.’ Dedicated to something, or other.
Very soon, after the COVID19 pandemic struck, Imperial College Business School had this to say on experts:
‘In 2016, when Michael Gove made his famous statement that “people in this country have had enough of experts”, it seemed experts and expert knowledge were on their way out. The opinion of populist politicians and online influencers were deemed much more relevant to decision making than the findings of scientists or the theories of economists. From the antivax movement to newly resurgent creationists, the spirit of the times was very much against the expert. Science and its evidence-based rationality were in retreat and the trend seemed unstoppable.
Fast-forward four years and the world is suddenly a very different place. Experts like Imperial College London’s Neil Ferguson, and Peter Piot from the London School of Hygiene & Tropical Medicine are now central advisors to government and the profiles of experts are the material of front-page stories. With the arrival of a global pandemic, experts are back – and with a vengeance!
So, what has changed? And what can we learn from the recent success of the experts who are shaping government policy on coronavirus? First, the experts who are currently leading the government’s policy response to the pandemic are not just experts, they are leaders. They know that simply understanding a topic deeply and having something to say on an issue is not enough.’ Etc. etc, glory glory Imperial College 1.
I found the final sentence interesting. ‘They know that simply understanding a topic deeply and having something to say on an issue is not enough.’
In short, to be an expert you must also be a leader? I think this is probably true …. You certainly have to be at the top of some organisation or other.
Anthony Fauci for example. He was held by the mainstream media to be the number one expert about COVID19. His position unassailable – or at least it was. He was, and remains, the head of the National Institute of Allergy and Infectious Diseases. He remains the Chief Medical Advisor to the President.
Did he know more than anyone else about Sars-Cov2? Was this even a requirement? Tricky, as this was a completely new virus. Was he the perfect man for the job? He most certainly ticked all the expert boxes – so he should have been the ideal man? Hire that man right now…
Of course, there are those who have been far more sceptical about the value added by experts – to anything. David Sackett, who was a driving force behind the Evidence Based Medicine (EBM) movement – and who was also a very good man – wrote an article in 2000 entitled ‘The sins of expertness and a proposal for redemption.’
Here are a couple of sections. I suggest you read the entire article; it is not very long:
‘Is redemption possible for the sins of expertness? The only one I know that works requires the systematic retirement of experts. To be sure, many of them are sucked into chairs, deanships, vice presidencies, and other black holes in which they are unlikely to influence the progress of science or anything else for that matter.’
‘But there are still far more experts around than is healthy for the advancement of science. Because their voluntary retirement does not seem to be any more frequent in 2000 than it was in 1980, I repeat my proposal that the retirement of experts be made compulsory at the point of their academic promotion and tenure.’2
In this paper he refers to an earlier piece, written in 1983, where he first called for the retirement of all experts. Having voluntarily ‘retired’ himself as an expert in the field of ‘compliance with therapeutic regimes’. As he added:
‘I received lots of fan mail about this paper from young investigators, but almost none from experts.’
Some twenty years later he ‘retired’ himself again. This time as an expert in the field of evidence-based medicine, some would say the expert. He believed he had attained too much power and status and was therefore distorting everything around him.
As with all other acknowledged experts, he found that junior researchers deferred to him, and simply would not question him. He came to the conclusion that the very presence of an expert impaired scientific progress. [Of course, of all the experts in the world, he was the one that should not have retired].
In his opinion, experts crystallised into barriers to the progress of new ideas, and most other forms of innovative thinking. Their primary role became an immovable pillar, supporting the existing status quo. Of course, this expert problem has been recognised by many others … For example, Max Plank, in his famous quote:
‘A new scientific truth does not triumph by convincing its opponents and making them see the light, but rather because its opponents eventually die, and a new generation grows up that is familiar with it.’
Or:
‘Science advances one funeral at a time.’
So, who you going to call? If, that is, you are a government, and there is a pandemic? You do what everybody does. You call on the established experts. Leaders who sit at the top of the pyramid.
Those professors garlanded with honours. Opinion leaders. Even the mighty key opinion leaders (KOLs). No need to look elsewhere. All the expertise can easily be found, right? And the experts all know each other, so they can also recommend their expert friends – the ones they know and get on with.
A few years ago, there used to be an expression in business, which went something like this: ‘you never get fired for hiring IBM?’ Why not? Because IBM was huge, and they had the reputation of being the major players in IT solutions.
No-one would ever ask you to explain why you hired them. You just did. IBM was also bloated, cumbersome and vastly expensive – containing about as much innovation as a squashed cabbage. Which eventually caught up with them… eventually. Now, you tend to hire another massive company … GE, or suchlike. IBM still exists, but it came very close to the edge.
Of course, everyone needs expertise. If you want to build a bridge, then hire an architect and engineers who are capable of designing and constructing one that does not fall down. This requires skills and knowledge that take years to attain. True, validated, expertise.
Equally, if you want someone to replace your hip, find an anaesthetist and an orthopaedic surgeon, and their team of experts. Don’t pop down the local Botox clinic and hope for the best.
However, if you find yourself in a situation never seen before, where no-one really knows what to do … Then you will find experts are always going to propose doing only what they have always done. What they already know. As used to be said of generals, that they always started off any new war, using the exact same tactics that were being used at the end of the last war. Which never worked. Things had moved on … they hadn’t.
I do find it ironic that when the pandemic started, the key advisor to Boris Johnson was Dominic Cummings? The great ‘disruptor,’ the man who wanted to break apart the ‘cosy establishment’ and replace it with new thinking, and innovation. Here from the article: ‘Dominic Cummings: A model of disruptive leadership?’ [Sub-header. “The best way to spot those at the vanguard of disruption is by their unpopularity”].
The underlying problem is widespread institutional inertia that serves to contain rather than facilitate change. Leaders soon realise that being truly disruptive carries risks that either they, their board-level superiors, or those they lead find hard to tolerate. Few therefore follow through on good intentions, the common default being safety first…
Rightly or wrongly, Cummings believes the UK is being held back by a cosy establishment that stands in the way of reform. He openly disdains convention, as when deliberately bypassing traditional campaigning methods to sell Vote Leave’s ‘Take Back Control’ message, even if this means sailing close to the ethical wind.
You can tell that Cummings hits raw nerves because criticism of his modus operandi is laced with attacks on everything from his personal manner to his dress sense. But you wouldn’t bet on him lasting much longer in the Whitehall machine. The quicksand of inertia has a habit of swallowing disrupters in organisations a lot less complex and cunning than that of government … [Good call]
Change rhetoric might tell us that we need more people prepared to break the mould but our recent political experience indicates that having the will to disrupt rarely guarantees success against stubborn guardians of the ‘same old, same old’. 3
Well, as everyone in the UK knows, Dominic Cummings is now history. Disruptor no more. However, in February/March 2020 he was still very much in place – and he had Boris Johnson’s ear, as his most trusted advisor. You might have thought, therefore, that the scientific advisory group for emergencies (SAGE) would have contained a disruptor or two.
But no, we got the exact same old, same old. The well-established experts. The Chief Medical Officer, the Deputy Chief Medical Officer, the Chief Scientific Officer, the chief of this, the professor of that.
The great problem is that this ‘same old same old’ was going to have an in-built, and almost pathological resistance to risk – of any sort. In this case, by risk, I mean doing anything that is slightly different. Anything that may open you up to criticism. This is the main reason why the SAGE doomsday predictions have never matched reality.
Just as you never got fired for hiring IBM. If you are an epidemiologist, you never get fired for modelling a worst-case scenario. If you say there will be six thousand Omicron deaths a day – in the UK alone – yet the highest number reached was three hundred. Then are safe. This is the approved, standard direction of error.
On the other hand, if you said there would be three hundred deaths a day and it ended up at six thousand… all hell breaks loose. To quote Professor Graham Medley, who chaired the SAGE modelling group.
‘Professor Medley said one of the ‘worst things’ would be for the modellers to under-predict the approaching wave.
He told MPs: ‘The worst thing for me as chair of the committee is for the Government to say “why didn’t you tell us it would be that bad?”, so inevitably we are going to have a worst case that is worse than reality.’ 4
…inevitably we are going to have a worst case, that is worse than reality’… Roll that idea around for a moment or two. I did, and this was my interpretation. ‘Inevitably, our models will always be worse than the worst thing than can ever happen.’ Ergo, our models are designed to be utterly useless and inaccurate. A great way to plan your response?
Any decent disruptor would have questioned the assumptions underlying this ‘worst thing’. A disrupter would flip the question on its head. The worst thing, surely, would be to drive the Government into a massive over-reaction that could lead to such things as … thousands of deaths from undiagnosed cancers.
Or patients dying of heart attacks, terrified to attend hospital. Or care homes being flooded with COVID19 positive patients, because the hospital had to be cleared out. Or a tidal wave of mental health problems in children and adolescents. Or an increase in domestic abuse. Or … keep going, there are many damaging things that were caused by lockdown.
They would also have questioned the massive financial cost of extended lock-downs. The new hospitals that could not be built in the future. The much-needed healthcare staff not being hired – because we have run out of money. The inability to pay inflation matching pay rises, leading to staff resignations and loss of morale. The drugs that can’t be paid for, and on and on.
They would have remined those on the advisory board that this was not a zero-sum game. Every COVID19 death prevented, no matter how much it costs, is not necessarily a positive. There will be major, damaging, downsides to your actions, and these have to be taken into account.
However, if you stuff your advisory body with established experts you will get what you got. A group of people whose primary motivation is to ensure that they cannot be blamed for making a mistake. They will ‘hire IBM’. They will battle to maintain the status-quo. ‘Think of how terrible things would have been if we had not driven lock-downs on the entire country for weeks and months.’
Disruptor: ‘Look at how badly wrong your predictions have been, and the enormous and widespread damage you have caused. The cost of which may never even be known.’
Yes, as you can probably gather, I am not a great fan of experts. Of course, I do love expertise… and I love doing things as well as possible. At least those things that have been proven to work. I love innovation, and new thinking. Different ways of looking at the world.
What I hate, what we should all hate, is that any attempt to shift the status quo seems doomed to fail:
‘Change rhetoric might tell us that we need more people prepared to break the mould, but our recent political experience indicates that having the will to disrupt rarely guarantees success against stubborn guardians of the ‘same old, same old’.
When COVID19 arrived, we needed disruptors, new ways of thinking, and acting. We needed clear sighted innovators. What we got, predictably, inevitably, depressingly, were ‘experts’ to lay their cold, dead, hands on the situation. Experts desperate never to be ‘wrong.’ Having first decided what wrong meant. In this case it meant never, ever, underestimating the number of COVID19 deaths.
At this point I feel the need to quote David Sackett once more: I repeat my proposal that the retirement of experts be made compulsory at the point of their academic promotion and tenure.
Hear, hear. ‘Do I have a second for this proposal?’
Dr Joe Mercola – a man who I admire – interviewed me about The Clot Thickens recently. This is my latest book, in case you are unaware of this majestic tome… if so, where have you been? It was all over the mainstream press, all major news channels… then I woke up.
This interview is now going to be available from Sunday 13th February, for forty-eight hours only* [unless you go behind the pay wall]. I am not entirely sure what hour it will posted, as the US is several hours behind the UK.
As some of you may know, various authorities tried very hard to shut down Mercola’s website, as he had many articles critical of the mainstream response to COVID. He ended up having to take down all his articles after forty-eight hours, then put them behind a pay wall. Some weird compromise or other, that I don’t fully understand. Anyway, you can hear my great words of wisdom if you wish, from Sunday the 13th for forty-eight hours only*. You have been warned.
Having published the guest article by ‘Bob’ there have been a lot of comments. I have not replied, as it was not my article. However, Bob has put together a kind of generic reply to people’s posts which I think may be useful and informative.
Hello Everybody – I wrote the article and have read your comments. First, I want to thank Dr. Kendrick for publishing my thoughts in his esteemed blog. I started following Dr. Kendrick’s blog around 2015 and am a devoted reader. My favorite single post is the one titled “Salt Is Good for You.”
I was introduced to the wonderful world of Vitamin D in 2010 when a physician directed me to the Vitamin D Council website, now defunct. John Cannell’s articles on influenza, and on autism, were compelling for me. I started taking 5000 IU per day in December 2010 (at age 60) and I noticed that I no longer got colds or influenza in the winter. Before 2010 I would get one or two colds every winter, with the usual sore-throat – head cold – chest congestion sequence. Since then I have had exactly 5 colds, all very mild. I now take a higher dose but I think people should look at the advice provided in the Grassrootshealth article and make up their own minds as to appropriate dose.
My article sketches out a theory that yields a series of hypotheses which can be tested. Thus, one notes a general pattern, and scratches one’s head over exceptions. Hence my discussion of Ecuador and South America.
I propose that an underlying difference in susceptibility to coronavirus arises from the fact that the New World was epidemiologically isolated from the rest of the world until about 500 years ago. Before then the indigenous populations of the New World and the Old World were exposed to and therefore developed adaptive mechanisms to ward off different groups of pathogens.
This is illustrated by the well-known susceptibility of New World populations to Old World pathogens like measles and smallpox. The higher death rates in many South American countries suggests that the indigenous New World genome has not yet fully adapted to Old World coronaviruses. Thanks, Terry Wright, for the Guayaquil reference.
Thank you, John Stone, for the reference to the Stadler article observing that there is a significant level of immunity to Covid19 already present in the population. We had another clue to this fact early in the pandemic with outbreaks on two ships, the cruise ship Diamond Princess, and the US aircraft carrier Theodore Roosevelt. Both occurred before people took protective measures, and it can be argued that the close quarters of shipboard life are ideal for the transmission of the disease. On both ships, everybody was tested for Covid19. Results were remarkably similar. On both ships, 17 percent of the people tested positive for the virus, and of those, 50 percent were asymptomatic. It looks like 83 percent of the shipboard populations were immune to the virus. Why?
Several of you have pointed out that death rates from various countries are inconsistent with the sunshine theory. First, do not confuse cases with deaths. Case totals are the creatures of testing programs, which vary from place to place. Deaths are a much harder statistic.
That said, country-specific factors come into play. In comments, Andrew Larwood and Simon C pointed out Finland’s vitamin D supplementation program would reduce deaths. Their death rate per million is 59, which seems very low for a country in the winter at such a high latitude. Now I know why. Another factor may be fatty fish, a dietary source of Vitamin D, which is consumed in quantity in Scandinavia. Håkan, your comment about Sweden is relevant.
Many people attribute the higher rate of Covid19 deaths to the lack of a lockdown. However, an equally good case can be made that the dark-skinned immigrant population in Sweden is more deficient in vitamin D and thus more susceptible to the illness. See this article by Dr. David Grimes where he notes that 1 percent of the Swedish population may be responsible for 40 percent of deaths: http://www.drdavidgrimes.com/2020/04/vitamin-d-and-immunity-important.html and this one: https://www.bmj.com/content/368/bmj.m1101/rr-10 If you have read Dr. Kendrick’s last blog post, “Distorting science in the COVID pandemic,” you would know that the very low death rate (7 per million) in Morocco may be due to their use of hydroxychloroquine to treat sick patients.
David Bailey, your comment is spot-on. Look at the seasonality of acute myocardial infarction. In the higher latitudes one gets daily doses of sunshine in the summer, but not in the winter, and it is the dailiness of the dose that is key to protection of the endothelium. This is also why randomized clinical trials of vitamin D tend not to show a strong protective effect against CVD, because most do not use a daily dose, rather, dose intervals are weekly or longer (and the dose is usually too small and the duration of the trial too short).
I have known Steve Bennett for a few years now. He became a convert to the high fat low carb world (primal living and eating) and has set up Primal Living to promote this dietary message to the world, using his considerable financial muscle to do so.
In the midst of lockdown, he is running a series of youTUBE programmes, and interviews, discussing a number of topics, and from the resultant publicity he is hoping to gain donations to food banks – which are really struggling at the moment. He will match donations up to £100,000 to do this.
I hope you can watch some of the programmes. I hope you can donate, if you feel able. I am appearing on a couple of the shows. I think this is a very good cause. I support Steve Bennett and his team in the endeavour. Below is a slightly amended press release…
THE FOOD BANK SHOW – YouTube channel: The Primal Living.
Guests on the shows include politician Tom Watson and Dr Aseem Malhotra and Dr Malcolm Kendrick – amongst others (we are also waiting for conformation of singer Liam Payne – Liam is a huge supporter of food banks). The show will also be connecting live to the Trussell Trust, who with their army of amazing volunteers keep many of our food banks operational.
Every morning thereafter, we will be broadcasting live on youTUBE providing food and health advice. Steve Bennett The Food Bank Show host will be joined by doctors, medical experts and chefs, many of whom contributed to his latest health book FAT and Furious. Together – they will be taking your questions from around the country and additionally during the shows we will video link to food banks across the UK and discover new ways we can all help offer support.
With fast food chains closed, we want to seize this opportunity to reshape the eating habits of our nation and improve everyone’s health and whilst we are doing this together – help feed those most in need during this crisis.
Join Steve and his family, as they put on a truly interactive show and please encourage everyone you care and love to join them too.
Further Info
We aim to generate as many donations to the Food Banks as possible. Steve Bennett is going to match donations up to the first £100,000.
People can donate via a text or a justgiving page.
The show has 3 aims;
Help viewers learn about how to eat healthily
Raise money for foodbanks, with our partnership with the Trussell Trust
Entertain people
2% of UK families currently rely on food banks, but the virus has resulted in fewer donations and fewer volunteers being able to help.
After keeping social distance and washing hands, the next best thing we can do to help our immune and defences is to be metabolically healthy, this will be discussed at detail in the shows.
Most vulnerable are those with metabolic syndrome. In Italy while the average age of death was 81, the average person who died suffered from 2.7 underlying chronic medical conditions. Including High blood pressure, cancer, diabetes. Lowering blood pressure, reversing diabetes, high sugar levels, can happen quickly with the right advice and that is the message the doctors will be promoting.
In Wuhan, more than 60% of people who died, or had serious complications had high blood pressure or type 2 diabetes.
UK over 60% adults are overweight or obese. Only 17.4% of American adults are metabolically healthy.
I thought I should say something about the coronavirus for readers of this blog. I need to state that the situation is fast moving, facts are changing, and I am not asking anyone to go against any current medical advice.
Here, I am simply providing advice that I believe, currently, may be of benefit to people out there. I am acutely aware that there is controversy swirling about, but I will not promote anything that can cause any significant harm – but may cause significant good.
I have tended to look back a few years in time for some evidence, because current, emerging evidence is subject to massive bias and controversy, with various vested interests getting involved. The ‘older’ evidence has not been done in a rush and is therefore more measured.
1: Anti-inflammatories (NSAIDs)
COVID-19 appears to impact the lungs more than any other organ and COVID-19 can be thought of as a ‘viral’ community acquired pneumonia. There has been evidence for several years that anti-inflammatory agents e.g. ibuprofen, naproxen (NSAIDs) may worsen community acquired pneumonia. As highlighted in this 2017 paper:
‘Non-steroidal Anti-inflammatory Drugs may Worsen the Course of Community-Acquired Pneumonia: A Cohort Study:
CONCLUSIONS:
Our findings suggest that NSAIDs, often taken by young and healthy patients, may worsen the course of CAP with delayed therapy and a higher rate of pleuropulmonary complications.’ 1
There is now anecdotal evidence, particularly from France, that patients who take NSAIDs do considerably worse. It has been suggested they may lead to an increased death rate.
ADVICE: Avoid NSAIDs if possible
2: Vitamin C
Vitamins always cause massive controversy, and the mainstream medical community tends to be highly critical of the use of vitamins. However, vitamin C has been found to have many, many, positive impacts on the immune system. It also protects the endothelium lining blood vessels – thus preventing/delaying passage of pathogens from the bloodstream.
I include the full abstract from the 2017 paper ‘Vitamin C and Immune Function.’ It contains a great deal of medical jargon, but I have highlighted the most important parts.
‘Vitamin C contributes to immune defense by supporting various cellular functions of both the innate and adaptive immune system. Vitamin C supports epithelial barrier function against pathogens and promotes the oxidant scavenging activity of the skin, thereby potentially protecting against environmental oxidative stress.
Vitamin C accumulates in phagocytic cells, such as neutrophils, and can enhance chemotaxis, phagocytosis, generation of reactive oxygen species, and ultimately microbial killing. It is also needed for apoptosis and clearance of the spent neutrophils from sites of infection by macrophages, thereby decreasing necrosis/NETosis and potential tissue damage.
The role of vitamin C in lymphocytes is less clear, but it has been shown to enhance differentiation and proliferation of B- and T-cells, likely due to its gene regulating effects. Vitamin C deficiency results in impaired immunity and higher susceptibility to infections. In turn, infections significantly impact on vitamin C levels due to enhanced inflammation and metabolic requirements.
Furthermore, supplementation with vitamin C appears to be able to both prevent and treat respiratory and systemic infections. Prophylactic prevention of infection requires dietary vitamin C intakes that provide at least adequate, if not saturating plasma levels (i.e., 100–200 mg/day), which optimize cell and tissue levels. In contrast, treatment of established infections requires significantly higher (gram) doses of the vitamin to compensate for the increased inflammatory response and metabolic demand.’ 2
In short, Vitamin C can help prevent respiratory infections. It can also help to treat established infections, although much higher doses are required. This seems to fit with emerging Chinese data which appears to be showing considerable success with high dose intravenous Vitamin C in treating coronavirus.
It is unlikely that anyone working in the medical system in the West will agree to using high dose Vitamin C as part of any management plan. However, if your loved one is extremely ill in hospital I would recommend speaking to the doctors and asking if this can be added.
Whilst it is possible that vitamin C may prove ineffective, it also does no harm. Those who are currently attacking the use of Vitamin C and attacking those who believe vitamin C may be beneficial are, I believe, mainly concerned with their personal reputations.
ADVICE: Take at least 2g of Vitamin daily C to ‘prevent’ infection, probably more like 5g. Increase the dose to at least 10g if you are suffering symptoms.
3: ACE-inhibitors/ARBs
COVID-19 appears to enter the body using the ACE2 receptor (found on the surface of many cells, particularly in the lungs. Also found in high concentrations in the heart and kidneys.
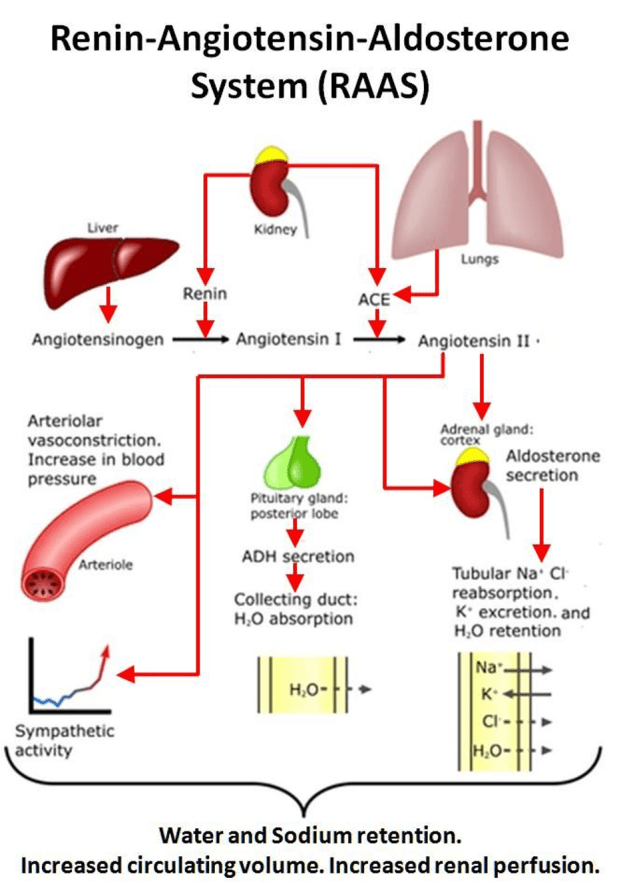
Because of its affinity to ACE2 receptors (and the more widespread Renin Aldosterone Angiotensin System or “RAAS”) COVID-19 is causing upset with the whole system – in complex ways. The system itself is complex.
To remind those of a more technical bent, here is the system:
I wished to make it clear that if COVID-19 impact on the RAAS system, trying to work out the resultant abnormalities, is not easy.
There are two main drugs that are designed to lower blood pressure by ‘interfering’ with the RAAS system. ACE-inhibitors (angiotensin converting enzyme inhibitors), and ARBs (angiotensin II receptor blockers). They are very widely prescribed.
Some people have suggested that these drugs should be stopped. Others have suggested that they should be continued. You may be able to see why the advice is contradictory, given all the possible interactions.
However, it does seem the COVID-19 creates hypokalaemia (a low blood potassium level). A rising potassium level indicates recovery from the virus. This is probably due to interference with the hormone Aldosterone due to degradation of many ACE-receptors in the body.
ADVICE – currently not enough information to provide any advice on ACE-inhibitors and ARBs. However, increased consumption of potassium, if symptomatic, can be advised. Dose?
‘People who eat large amounts of fruits and vegetables tend to have a high potassium intake of approximately 8000 to 11,000 mg/d,’ 3
So, up to Ig a day appears perfectly safe, and if more is being lost through the kidneys with COVD-19, there appears to be little danger of overdosage.
4: Chloroquine and Hydroxychloroquine
These drugs normally used to treat/prevent malaria (and are also used to treat various ‘immune’ disease). However, they have been found to be effective in treating other viruses and seem to have been highly effective against COVID-19 4. These drugs will only be available as part of medical management. They cannot be bought over the counter (in any country, as far as I know).
If you, or a loved one, is seriously ill, I would urge you to ask for – one or the other – to be used. Hydroxychloroquine has fewer side effects (drug related adverse effects)
ADVICE – Ask for one of these drugs if you, or a loved one, is seriously ill with COVID-19.
5: Vitamin D
This one is simple. Vitamin D has important effects on the immune system 5. A low vitamin D level in the winter is almost certainly why flu epidemics occur in the winter months. [Vitamin D is synthesized in the sun by the action of sunlight].
ADVICE – take at least 2000iu vitamin (preferably D3) daily.
I hope some people have found this useful. If anything I have written here proves to be wrong, or dangerous, I will change it. However, I am working on the basis here of ‘first, do no harm.’ The worse thing that any of this advice can do, I believe, is to NOT work.
In this blog I am going to have a closer look at an issue that has niggled away at me for a long time. Placebos. In part I was stimulated to write on this following an article that Maryanne Demasi published on the CrossFit site ‘Sometimes a placebo is not a placebo.’ 1
There are many, many different issues about placebos. Most of which people don’t even consider. Such as, is there really such a thing as the placebo effect? And if there is, how come we haven’t managed to sort out what it actually might be? I know most people reading this will retort. ‘Of course, there’s a placebo effect. It’s a known thing.’ Personally, I am not so sure. Like many known things it begins to fall apart under a bit of critical examination.
For example:
‘Whether you know you’re taking a placebo pill or not, it will still have a beneficial effect, new research has revealed. Scientists from Harvard University and the University of Basel prescribed a group of minor burn victims with a “treatment” cream, telling only some of them that it was a placebo. After the cream was applied, both groups reported benefits, despite the placebo cream containing no medicine.
The study goes against traditional medical thinking surrounding the placebo effect, which has always revolved around the idea that it was necessary to deceive patients in order for “sugar pills” to be clinically effective.’ 2
In short, you get the placebo effect whether you know, or don’t know, that you are receiving a placebo. Which kind of blows a major hole in rationale underpinning double-blind, placebo controlled clinical trials.
However, I am not exploring that particular rabbit hole today.
Today I am going to look at the question. What is in a placebo? You may well believe you know the answer to this. A placebo is an inert formulation containing no active ingredients.
This is a reasonable assumption to make as the medical definition of a placebo, as taken from the Merriam-Webster medical dictionary, is:
‘1a: a usually pharmacologically inert preparation prescribed more for the mental relief of the patient than for its actual effect on a disorder
b: an inert or innocuous substance used especially in controlled experiments testing the efficacy of another substance (such as a drug)’
A few years ago, I was speaking to an investigative journalist from the Netherlands who was trying to get hold of the placebo tablets used in a particular clinical trial. He wanted to establish exactly what was in them, and if they were truly inert. No such luck, these placebos were very carefully guarded, as was any information about what they contained.
He gave up, but I did file his tale in my mind, recognising this was something that needed to be looked in greater detail at some point in the future. Can it be true that placebos are not actually inert?
Surely, it’s possible to ask the pharmaceutical company running the trial what’s in the placebo. Well, you can try. To quote a section of Maryanne’s article
‘The process of obtaining regulatory documents, however, is by no means straightforward. In fact, it is often complicated and time consuming. I have made multiple appeals to a European drug regulator (Medicines Evaluation Board) to obtain information (Certificate of Analysis) regarding the ingredients of a placebo used in a controversial statin study (JUPITER trial), but so far, they have fallen on deaf ears. So, too, have my requests to the trial’s lead investigator, Dr. Paul Ridker.
Medical journals will need to take responsibility and insist that published papers report on the methodological details of “inactive” placebos. Recently, Shader of Clinical Therapeutics stated, “It will no longer be sufficient to simply indicate that a placebo was used.”
“We will require that a full description of any placebo or matched control used in a clinical trial be given in the Methods section. This means that color; type (capsule or pill or liquid); contents (e.g, lactose), including dyes; taste (if there is any); and packaging (e.g, double-dummy) must be noted,” he stated. “We are instituting this change as part of our ongoing effort to facilitate replication of findings from trials. All too often this valuable information is omitted from published trial results.”
In short, you can’t find out what is contained within the placebos. Or at least, it is exceedingly difficult – to impossible.
This is very disturbing indeed, because it has become increasingly clear that placebos are often far from inactive or inert. In fact, they often contain some quite unpleasant substances. For example, here from an article in Medical News Today
‘The authors outline an example where a particular placebo skewed the results of several studies. In studies that investigated oseltamivir, which people may know by its brand name Tamiflu, scientists often added dehydrocholic acid to the placebo.
Dehydrocholic acid has a bitter taste, as does oseltamivir. The researchers chose to add this chemical to the placebo so that the participants would not know whether they had received the active drug or the placebo.
However, both dehydrocholic acid and oseltamivir cause gastrointestinal side effects. When scientists attempted to calculate the rate of gastrointestinal side effects due to oseltamivir, they compared them with side effects from the placebo.
As the placebo also caused these types of symptoms, scientists underestimated the overall gastrointestinal side effect rate for oseltamivir.’ 3
Essentially, and you may find this rather shocking, a company doing a clinical trial can stick almost any nasty substance they like into a placebo and tell no-one. There are no regulations to prevent this happening, or at least none that I can find.
From time to time, however, the secret ingredients are revealed, or discovered, such as dehydrocholic acid. Here is Maryanne on the Gardasil (HPV) vaccine. In this case the ‘secret ingredient’ in the placebo was also identified.
‘In trials of the human papilloma virus (HPV) vaccine, participants were told they were either receiving a “vaccine or placebo.” The vaccine manufacturer defines a placebo as an “inactive pill, liquid, or powder that has no treatment value.”
However, participants in the placebo group did not receive an inactive substance of no treatment value. “Instead,” RIAT researchers state in the BMJ, “they received an injection containing amorphous aluminium hydroxyphosphate (AAHS), a proprietary adjuvant system used in the Gardasil vaccine to boost immune response.”’ 4
[RIAT = Restoring invisible and abandoned trials. Good people]
This is worrying. Many of those who are concerned about the potential for vaccine damage, believe it may well be the amorphous aluminium hydroxyphosphate (AAHS) itself which is the substance that can cause the adverse effects seen with many vaccines.
If both placebo, and vaccine, contain this adjuvant, then… it’s a free pass for the vaccine. In order to hide adverse effects with the vaccine, the placebo contained the substance suspected to cause adverse effects. Anyone who thinks that is remotely acceptable needs a long hard look in the mirror…
However, important thought it may be, it is time to move onto my favourite subject, statins – and placebos. For years I been highly suspicious of the adverse effect rates seen in the statin clinical trials. My concerns, and the concerns of others, formed part of a letter written to the then Health Secretary (Jeremy Hunt), and also to the National Institute for Health and Care Excellence 5
Here was the section on adverse events:
Conflicting levels of adverse events
In emphasising the cost per Quality Adjusted Life Year (QALY), NICE is clearly making a major assumption that the key issue is mortality reduction, and that statins lead to very few adverse effects. We would question this very strongly.
The levels of adverse events reported in the statin trials contain worrying anomalies. For example, in the West of Scotland Coronary Prevention Study (WOSCOPS, the first primary prevention study done), the cumulative incidence of myalgia was 0.6% in the statin arm, and 0.6% in the placebo arm*
However, the METEOR study found an incidence of myalgia of 12.7% in the Rosuvastatin arm, and 12.1% in the placebo arm
Whilst it can be understood that a different formulation of statin could cause a different rate of myalgia, it is difficult to see how the placebo could, in one study, cause a rate of myalgia of 0.6%, and 12.1% in another. This is a twenty-fold difference in a trial lasting less than half as long*.
Furthermore, the rate of adverse effects in the statin and placebo arms of all the trials has been almost identical. Exact comparison between trials is not possible, due to lack of complete data, and various measures of adverse effects are used, in different ways.
However, here is a short selection of major statins studies.
AFCAPS/TEXCAPS: Total adverse effects lovastatin 13.6%: Placebo 13.8%
4S: Total adverse effects simvastatin 6%: Placebo 6%
CARDS: Total adverse effects atorvastatin 25%: Placebo 24%
METEOR: Total adverse effects rosuvastatin 83.3%: Placebo 80.4%
LIPID: Total adverse effects 3.2% Pravastatin: Placebo 2.7%
JUPITER: Discontinuation rate of drug 25% Rosuvastatin 25% placebo. Serious Adverse events 15 % Rosuvastatin 15.5% placebo
WOSCOPS: Total adverse effects. Pravastatin 7.8%: Placebo 7.0%
Curiously, the adverse effect rate of the statin is always very similar to that of placebo. However, placebo adverse effect rates range from 2.7% to 80.4%, a thirty-fold difference.
How can the adverse effects of placebo range from 2.7% to 80.4%? Yes, there can be differences in the way that adverse effects are recorded, and that could explain, perhaps a five-fold difference – being extremely generous. But a thirty-fold difference?
Also, how can it be possible that the adverse effects of the placebo, and the statin, are always, almost exactly the same, in all trails – no matter the absolute figure. I believe that this could not possibly occur unless:
The placebos in each trial were carefully formulated to cause adverse effects at the same rate as the statin
The statistics on adverse effects were manipulated
Neither possibility should fill anyone with joy, nor confidence in the regulatory systems.
I have raised this issue with a number of different people, but they all seem determinedly disinterested. I suppose that if either of my two statements are true, it means that the entire database of randomised double-blind placebo-controlled trials can no longer be trusted. This is not a nettle to be grasped. It is a fifty-thousand-volt power line with a sign reading ‘Danger of Death!’ attached.
I can well understand the reluctance to investigate. However, I do not believe that we can possibly allow the formulation of placebos to remain a well-kept secret in future, current, or past trials.
If my suspicions about placebos are wrong, then can someone please prove me wrong.
*in the letter I had calculated this figure wrongly. It was not 0.06%, it was 0.6%. So, I have changed the text in the blog to reflect that.
Several people have asked after my welfare as I have not updated this blog for some time. The answer is that I am okay. Thanks for your concern. There have been a few things going on, one of which I will be able to speak about – at some point in the future – that have been taking up inordinate amounts of my time.
I am also writing, but for some reason, every time I sit down to write a new blog my mind goes completely blank. A very difficult thing to explain. It is as if a million thoughts all gather and just mangle each other up. Things seem very clear when I am walking about, but the moment I try to get started – glomp.
I am not sure if this is what is called writer’s block. It cannot really be, because I am writing other things – such as another book. However, it is very frustrating. I did fear maybe that I have run out of things to say – but in truth each day sees a newspaper headline, or a medical research paper, that has me itching for the keyboard. How can there be so much nonsense written in the world?
So, instead I am writing this rambling nonsense, that is of very little interest to anyone I suspect, but it may get me started again. Re-set my brain into super-blog mode – if there is such a thing.
Because I still believe there is a need for voices to question the misleading rubbish being churned out by people who claim to be scientists. Especially medical scientists, such as my great friends in Oxford who can write the most outrageous gibberish and get it published.
I have always liked to believe that science is a self-correcting system. Researchers can head of in the wrong direction for many years, decades even, but in the end the scientific truth will always catch up with them, tap them on the shoulder and make it very clear they are just being silly.
The days when there were special devices for blowing smoke up the rectum have faded from memory:
‘When an “apparently dead from drowning” person was pulled from the Thames [river running through London], it was thought that two things needed to happen to successfully resuscitate them: warming of the body and stimulation. Tobacco was becoming popular in Europe thanks to its exportation from the Americas, and a well known stimulant thanks to the alkaloid nicotine. The nearly dead drowning victim can’t smoke themselves, and certainly can’t swallow anything. And since hypodermic needles weren’t to be fully-invented for another hundred years, the only logical way to administer tobacco was rectally. Plus, the warm smoke would warm the individual from the inside. Win-Win. Thus, the tobacco smoke enema was born, and devices placed all along the Thames river.’ 1
From here came the mocking expression ‘Blowing smoke up your arse.’ Yes, doctors have always been keen on such activities. The first Chinese Emperor was advised by his doctors to inhale vaporised mercury – which was a magical substance so incredibly healthy that everyone should be ingesting it.
Inevitably he went mad through mercury poisoning, and started running around the forests naked before being overthrown and murdered. Still he did leave a nice tomb with terracotta soldiers and even, so it is said, an underground lake of mercury – to keep him healthy in the afterlife.
My how we laugh now at such silly ideas. But medicine has continuously felt the need to do something, anything, for the patient – even if they have not the faintest idea what will happen. Good, or bad. Bernard Shaw wrote about this over a hundred years ago in Doctors Dilemmas.
‘When your child is ill or your wife dying,” when you are confronted by “the spectacle of a fellow creature in pain or peril, what you want is comfort, reassurance, something to clutch at, were it but a straw. This the doctor brings you. You have a wildly urgent feeling that something must be done; and the doctor does something. Sometimes what he does kills the patient.”’
Leeches, other forms of bloodletting, trepanning, full frontal lobotomies, removal of the toxic colon, the radical mastectomy, strict bed rest following a heart attack – all these things and many more. The ‘sometimes’ that kill the patient.
These things have all gone – mostly. Evidence, science, got rid of them. Stupidity cannot run forever. At least this was once true. Today, I am not so sure. The need to do something, anything, still runs deep in the psyche of all doctors. The concept of ‘sorry, I can’t really do anything about that’ has never been front of mind.
My personal motto is ‘Don’t just do something, stand there.’ I call it masterful inactivity; others may call it laziness.
Anyway, to return to the main issue here, which is that medical science may now be incapable of self-correction. Erroneous ideas will be compounded, built on, and can never be overturned. Because of a thing called non-reproducibility.
In most areas of science, there is nothing to stop a researcher going back over old research and trying to replicate it. The correct term is reproducibility. In every branch of science there is currently an acknowledged crisis with reproducibility.
‘Reproducibility is a hot topic in science at the moment, but is there a crisis? Nature asked 1,576 scientists this question as part of an online survey. Most agree that there is a crisis and over 70% said they’d tried and failed to reproduce another group’s experiments.’ 2
This is not good, but in medical research this issue is magnified many times. Because there is another in-built problem. You cannot reproduce research that has been positive. Take clinical trials into statins. You start with middle aged men, split them into two groups, give one a statin and one a placebo. At the end of your five-year trial, you claim that statins had a benefit – stopped heart attacks and strokes and suchlike.
Once this claim has been made, in this group, it becomes unethical/impossible to replicate this study, in this group – ever again. The ethics committee would tell you that statins have been proven to have a benefit, you cannot withhold a drug with a ‘proven’ benefit from patients. Therefore, you cannot have a placebo arm in your trial. Therefore, you cannot attempt to replicate the findings. Ever.
Thus, if a trial was flawed/biased/corrupt or simply done badly. That’s it. You are going to have to believe the results, and you can never, ever, have another go. Ergo, medicine cannot self-correct through non-reproducibility. Stupidity can now last for ever. In fact, it is built in.
We face a rather dismal eternity of blowing smoke up our arses.
I thought I should tell you that I am about to be deleted from Wikipedia. Someone sent me a message to this effect. It seems that someone from Manchester entitled User:Skeptic from Britain has decided that I am a quack and my presence should be removed from the historical record.
I have no idea who this person is, perhaps it is possible to find out? It seems a bit harsh as I recently contributed money to Wikipedia to keep it going. Was this a terrible mistake?
To be frank, I am not entirely bothered if I no longer appear on Wikipedia, but I am increasingly pissed off that self-styled anonymous ‘experts’ can do this sort of thing without making it explicit why they are doing it, what their motives are, and if they have any disclosure of interest.
Perhaps user Skeptic from Britain would like to reveal himself and provide some information as to why he is so interested in trying to wipe me out? Perhaps one or two of you here could join in the discussion and see what emerges.
His reasons for trying to get rid of me are the following
Malcolm Kendrick is a fringe figure who agues(sic) against the lipid hypothesis. He denies that blood cholesterol levels are responsible for heart disease and in opposition to the medical community advocates a high-fat high-cholesterol diet as healthy. Problem is there is a lack of reliable sources that discuss his ideas. His book The Great Cholesterol Con was not reviewed in any science journals. Kendrick is involved with the International Network of Cholesterol Skeptics, I suggest deleting his article and redirecting his name to that. Skeptic from Britain (talk) 20:29, 2 December 2018 (UTC)
For the past half a century, the concept of a healthy diet has been synonymous with a diet low in fat, and particularly low in what is all-too-often referred to as “artery-clogging” saturated fat, the fat found in quantity in eggs, butter, meat and dairy products. The result has been a national dietary prescription to eat ever more plant-based diets: copious fruits, green vegetables and whole grains, while we minimize our consumption of animal products.
For those of us who are overweight or obese, this advice has been accompanied by the insistence that we got that way merely by eating “too much” and that the only way to solve our problems is to eat less and exercise more. And yet this now ubiquitous dietary advice has coincided with unprecedented increases in the prevalence of obesity and diabetes, raising the obvious question of whether this advice and the belief system associated with it may somehow be to blame.
Are they based on sound science? And if they’re not, which the evidence strongly suggests, then how did we come to believe them and why? And, perhaps most important, what’s the alternative? Why do we get fat and diabetic, and what can we do about it?
By asking these questions for the past 20 years, Gary Taubes has become perhaps the single most influential journalist covering nutrition and health today. He’s certainly the most controversial. His investigative reporting on the science of nutrition and the dietary triggers of obesity and diabetes are fundamentally changing the way we eat and live. Michael Pollan has described him as the closest thing we have to a “scientific Alexksandr Solzhenitsyn,” exposing the intellectual bankruptcy of current nutrition science. The Atlantic recently described his investigative journalism as so tenacious and obsessive that he had “fallen through a wormhole from reporting into expertise.”
Taubes’s skeptical, rigorously scientific approach to nutrition science is unparalleled and now he wants to share both the approach and the implications to our health and how to eat to remain healthy.
In this blog I would like to highlight some of the evidence that is not there. The missing link, the lost chord. The thief that steals in, in the night. The thing that is not there when you look for it.
“As I was going up the stair
I met a man who wasn’t there!
He wasn’t there again today,
Oh how I wish he’d go away!”
When I came home last night at three,
The man was waiting there for me
But when I looked around the hall,
I couldn’t see him there at all!
Go away, go away, don’t you come back any more!
Go away, go away, and please don’t slam the door…”
There was a theory, indeed there still is, that a myocardial infarction starts with damage to the heart muscle (myocardium), and the blood clot forms afterwards. Carlos Monteiro, a Brazilian researcher with whom I often communicate, promotes and supports this, the ‘myogenic theory of heart disease’. He is not alone.
Now, superficially this idea may sound completely daft. However, there is a great deal of evidence that can be gathered to support it. First, in a significant number of myocardial infarctions, no blood clot can be found. Here, from a paper entitled ‘Myocardial infarction without obstructive coronary artery disease.’
‘A substantial minority of myocardial infarction (MI) patients have no obstructive coronary artery disease (CAD) at angiography. Women more commonly have this type of MI, but both sexes are affected.1’
So, how can you have an MI, if there is no blood clot, and no blockage of a coronary artery? A very good question M’lud.
There is also an increasingly recognised form of ‘heart attack’ called Takotsubo cardiomyopathy, named after the Japanese octopus pot. This is where you have all the signs and symptoms of a myocardial infarction, but it is not a myocardial infarction. It is due to extreme levels of stress – both positive or negative. Here I quote from the British Heart Foundation:
Takotsubo cardiomyopathy
This condition is also called acute stress-induced cardiomyopathy, broken heart syndrome and apical ballooning syndrome.
Takotsubo cardiomyopathy was first reported in Japan in 1990. The word ’Takotsubo’ means ‘octopus pot’ in Japanese, as the left ventricle of the heart changes into a similar shape as the pot – developing a narrow neck and a round bottom.
The condition can develop at any age, but typically affects more women than men. The good news is that often the condition is temporary and reversible.
What are the symptoms of Takotsubo cardiomyopathy? The main symptoms of Takotsubo cardiomyopathy are chest pain, breathlessness or collapsing, similar to a heart attack. In some cases, people may also suffer palpitations, nausea and vomiting.’2
You can, in fact, die from Takotsubo cardiomyopathy. Another myocardial infarction that is not a myocardial infarction.
Equally, you can find that people can suffer from a myocardial infarction days, or even weeks, after a blood clot blocked the artery. Here is a paper entitled ‘Plaque Instability Frequently Occurs Days or Weeks Before Occlusive Coronary Thrombosis.’
‘In at least 50% of patients with acute STEMI, coronary thrombi were days or weeks old. This indicates that sudden coronary occlusion is often preceded by a variable period of plaque instability and thrombus formation, initiate days or weeks before onset of symptoms.’3
So, there you go. You can have four types of myocardial infarction:
A myocardial infarction with no obstructive arterial disease
A myocardial infarction cause by stress, with no obstructive arterial disease
A myocardial infarction that happens weeks after the thrombus forms
The ‘classic’ myocardial infarction with thrombus formation followed rapidly by infarction.
What are we to make of this gentle reader? Three forms of ‘myocardial infarction’ that cannot be linked in time, or in any other way, to thrombus formation. Or, to put it another way the infarction a.k.a. the bit where the heart muscle becomes seriously damaged, is not related to a blockage in the artery either immediately, or at all.
In addition to this, there is the observation of ‘the completely blocked coronary artery, without myocardial infarction’. Here is a case history from the British Medical Journal:
‘A 75 year old man was admitted because of stable angina pectoris without any history of myocardial infarction. His risk profile consisted of arterial hypertension and hypercholesterolaemia. At the time he was being treated with 100 mg aspirin, 100 mg metoprolol, 20 mg pravastatin, and 40 mg isosorbide mononitrate daily. ECG showed sinus rhythm, no Q waves, and slight T wave inversions at lead aVL and I. A bicycle stress test resulted in horizontal ST segment depression of 2 mm at 75 W. Coronary angiography was performed and revealed coronary artery disease with complete occlusion of the proximal part of the left coronary artery.’ 4
At this point you could very reasonably argue that there truly is no consistent association between blood clots, arterial obstruction, and myocardial infarction. Or, to put it another way, the widely held view that the blood clot, and subsequent arterial occlusion, immediately precedes the infarction, is contradicted by evidence.
Which leads to the inevitable conclusion that something else must be going on. Perhaps it is true that the infarction, due to extreme stress and build of lactic acid does come first. Then, as a consequence, the clot forms in the artery.
Hmmmm. I don’t think so. However, in order to understand what is actually going on it is necessary, unfortunately, to dig even deeper, to find the man that isn’t there. Banksy, a man who paints on walls, is never seen, but we know he was there because, otherwise, you can’t explain the painting.
On the weekend of the 1st July I am giving a talk at the British Lifestyle Conference in Bristol UK.
This is a great grassroots movement of people, and many doctors, who are trying to achieve a more holistic approach to health. I hope some of you can come along. Here is what the organiser, Dr Rob Lawson, has put together for a mention on my blog.
Vital optimism at work – and play.
“Lifestyle Medicine has been shaped by the natural evolution of Medicine. It is an established approach that focuses on improving the health and wellbeing of individuals and populations. It combines the broad facets of modern healthcare practices with the deeper understanding of being human. In the 21st century it has never been more important as a concept. And that is to create a society and an environment, from cell to community, which nurtures healthy longevity.
It requires an understanding and an acknowledgement of the physical, emotional, environmental and social determinants of disease and wellbeing. Hence the LM practitioner will engage with us as patients and operate within a boundary of evidence-informed medicine. A boundary in which our ideas, values, mind-set and social context blend not only with the clinicians’ expertise but also with clinical research outcomes.
Importantly, Lifestyle Medicine has a wider responsibility to recognise upstream determinants of disease and to promote population health, to protect ecological health and to reduce health inequity. This requires a realistic team approach and recognition that not one discipline or profession alone can meet our health needs.
On 1st July 2017 in Bristol Dr Malcolm Kendrick will be joining other world renowned speakers in Bristol at the inaugural Conference of the British Society of Lifestyle Medicine, the Science and Art of healthy longevity, https://bslm.org.uk/event/vital-optimism/, to which you are warmly invited. If you have never heard him speak – this is your chance! No better way to spend a Saturday in July“
It is not often you are passed such terrible news. But sadly, Mike Cawdery, a regular and highly impressive contributor to this blog, was murdered along with his wife, on the 26th of May.
‘The devastated family of an elderly couple murdered in their home on Friday say they are struggling to understand what has happened. Michael and Marjorie Cawdery, both aged 83, were the victims of a brutal knife attack leaving them both with fatal injuries.
A family spokesperson said: “The awful and incomprehensible events of Friday 26 May have deprived our family of two wonderful people Michael and Marjorie who were our father, mother, brother, sister and grandparents. “We thank the police for their prompt response and professional actions. We also thank everyone who has expressed sympathy in whatever way and offered help.”
I found out about this from his GP, who was kind enough to e-mail this news. He knew that Mike posted comments to this blog on a very regular basis, and he thought that I should know what had happened. Thank goodness, he did, otherwise I would have had no idea. I would have simply wondered why Mike Cawdery, our statistician par excellence, had fallen silent. [In truth, other people have since, e-mailed me with the news].
I never met him, I never spoke to him, but I believe that I – and other readers of this blog- knew him well. He seemed ferociously intelligent, and still driven to do what he thought was right. I felt he was an admirable man. Funny how the Internet brings people together into a ‘family’ that converses and argues and supports and occasionally falls out.
In the last month, Mike Cawdery posted 117 comments on the blog, all of them were worth reading. Here was one of his last ever posts.
‘May I plead with you all to keep a watch on the BMJ and to use their RAPID RESPONSE system just as one uses Dr Kendrick’s comment section. Many of the comments and references cited here are equally valid on some relevant editorials, news items and even reports. All one has to do is give name and rough address and answer a question or two. Open to all including doctors.
May I take this opportunity to suggest that any one, a patient, carer and particularly doctors as the ultimate carers sign up as “patient reviewers”. Interesting and gets patients and carers involved. Too long have patients been treated little better than pets (may be with less respect??). It is people like Dr Kendrick that have given patients an outlet to express their views and knowledge.’
At 83, he was still active, still getting involved, and still trying to make the world a better place. Mike, you will be missed, by us all.
Lumen: The lumen of the artery is the hole in the middle that the blood flows through.
The artery wall: The artery wall is made up of three layers: Endothelium/intima, media and adventitia
The endothelium: Usually thought of as a single layer of endothelial cells than line the lumen of the artery. [The layer may be more than one cell thick]. This layer of endothelium acts as a barrier to blood, or anything in the blood, leaking from the lumen into the artery wall. There is a bit of space, sometime called the intima just under the endothelial cells.
The media: This layer is mostly made up smooth muscle cells and elastic tissue. The muscle can contract or relax, depending on circumstances
The adventitia: This outermost layer is mainly made up of collagen. It is very strong and keeps the artery in shape.
The atherosclerotic plaque: The areas of thickening and narrowing of arteries (in heart disease). These are usually found between the endothelium and the media – smooth muscle layer. They lie beneath the endothelium – within the artery wall itself. The area often referred to as the intimal layer of the artery.
The elevator pitch
Various people who work in business tell me of something called the ‘elevator sales pitch’. So-called, because of a (highly unlikely) situation whereby you find yourself in an elevator (which we in the UK call a lift) with a rich, famous, person. You have a short space of time to outline your idea to them, what it is, what it means, and why it is of value. They then hand over a hundred million dollars to invest in you, and your idea. Or something like that anyway.
Whilst the elevator pitch is clearly a mythical beast, the general point is reasonable. You should be able – or you should at least attempt – to condense your ideas into a very short space of time, before people get bored and walk away. Well, clearly I have miserably failed on this, as I am now writing part twenty-seven of my idea(s) on heart disease. In truth, I am planning on the elevator breaking down for about ten hours between floors to give me the time needed.
Recently, though, I have been speaking to a number of people who have successful careers in business, music, the arts and suchlike. I have been trying out my elevator pitch on them. Admittedly the elevator I am thinking of is in the Burj Khalifa in Dubai, but I am trying. So, here goes. Doors close on the elevator. Me and Bill Gates…
Me. ‘Forget diet, forget cholesterol, the real cause of heart disease is blood clotting.’
Bill Gates looks at his watch. ‘You have one minute.’
Me. ‘Blood clots can form and stick to the inside of artery walls. They then get absorbed into the artery wall itself where, normally, they are cleared away by specialised white blood cells. But if blood clots keep forming rapidly, at the same point, or the blood clots are bigger and more difficult to shift when they form, they cannot be cleared away quickly enough and so end up stuck inside the artery wall. This leads to a build-up of blood clot residue, and remnants, in the artery wall itself. Which means that repeated episodes of clotting, over time, build into thickenings, and narrow the larger arteries, mainly in the heart and the neck, growing somewhat like tree rings. These areas of damage are usually called atherosclerotic plaques.
In time, the process of blood clotting, over a vulnerable area, leads to heart attacks and strokes as the final, fatal blood clot forms over an area of the artery that is already thickened and narrowed. In short, atherosclerotic plaques are the remnants of blood clots. Heart attacks and strokes are the end result of the same processes that caused plaques to form in the first place. Heart disease is a disease of abnormal blood clotting. It is as simple as that. The end.’
Ping. Elevator door opens and Bill Gates walks out.
Do you think he believed me? Of course not. Heart disease is caused by cholesterol, end of.
Bill Gates: ‘Who was that complete idiot in the lift, make sure he never gets the chance to speak to me again.’
Man in black suit: ‘OK boss.’
I should point out that I have never spoken to Bill Gates, and almost certainly never will. I merely used his name as an example of someone that you might try to convince using an elevator sales pitch.
I also know that my sales pitch will just seem like the most complete nonsense to most people. How can I possibly claim that atherosclerotic plaques are blood clots, when no-one else in the entire world is saying it? Am I not simply a flat-Earther? Indeed, am I not a lonely flat-Earther baying at the moon. At least the moon currently passing overheard, to join all the other moons that clearly fall into a big basket on the other side of the Earth – to be returned from time to time by an enormous dung beetle.
I like to think not, because the ‘blood clotting’ hypothesis fits all known facts about cardiovascular disease. In fact, many people have proposed the ‘blood clotting theory’ of CVD over, what is now, hundreds of years. From Rokitansky to Duguid to Smith – and many more. Here, from a paper written in 1993 called ‘Fibrin as a factor in Atherosclerosis’, co-authored by Elspeth Smith.
[Just to first remind everyone that Fibrin is a critical element of blood clots (along with platelets). Fibrin is made up of short strings of a protein called fibrinogen. When the clotting system (clotting cascade) is activated, the end result is that fibrinogen is stuck together end to end, in order to create long sticky strands of fibrin that entangle themselves around the clot and bind it all together.]
‘After many years of neglect, the role of thrombosis in myocardial infarction is being reassessed. It is increasingly clear that all aspects of the haemostatic system are involved: not only in the acute occlusive event, but also in all stages of atherosclerotic plaque development from the initiation of atherogenesis to the expansion and growth of large plaques.
Infusion of recombinant tissue plasminogen activator (rt-PA) into healthy men with no evidence of thrombotic events or predisposing conditions elicited significant production of crosslinked fibrin fragment D-dimer. Thus, in apparently healthy human subjects there appears to be a significant amount of fibrin deposited within arteries, and this should give pause for thought about the possible relationship between clotting and atherosclerosis.
It also provides in vivo biochemical support for the numerous morphological studies in which mural fibrin and microthrombi have been observed adherent to both apparently normal intima and atherosclerotic lesions. It should be noted that these observations are based on the human and not just the animal model.
In 1852 Rokitansky discussed the “atheromatous process” (sic) and asked “In what consists the nature of the disease?” He suggests “The deposit is an endogenous product derived from the blood, and for the most part from the fibrin of the arterial blood”.
One hundred years later Duguid demonstrated fibrin within, and fibrin encrustation on fibrous plaques, and small fibrin deposits on the intima of apparently normal arteries. These observations have been amply confirmed but, regrettably, the emphasis on cholesterol and lipoproteins was so overwhelming that it was another 40 years before Duguid’s observations had a significant influence on epidemiological or intervention studies of haemostatic factors in coronary heart disease.’
Unfortunately, since that paper was written the emphasis on cholesterol and lipoproteins has become even more overwhelming, and research into blood clotting and atherosclerosis has faded to almost nothing. It appears that the vast sums of money to be made from cholesterol lowering has completely distorted research into this area. All the funding, and all the international experts, have charged into the blind-alleyway that is the cholesterol hypothesis.
In a kind of supreme irony, in 1992 Pfizer were also travelling down the blood clotting route. I have (mentioned before) possibly the only remaining copy of a small booklet entitled ‘Pathologic Triggers New Insights into cardiovascular risk.’ And I quote:
‘Several features of mature plaques, such as their multi-layered patterns, suggests that platelet aggregation and thrombus formation are key elements in the progression of atherosclerosis. Platelets are also known to provide a rich source of growth factors, which can stimulate plaque development.
Given the insidious nature of atherosclerosis, it is vital to consider the role of platelets and thrombosis in the process, and the serious events that may be triggered once plaque are already present.’
Of course, this leaflet was promotional, for their product doxazosin. Doxazosin lowers blood pressure and also has effects on urinary retention. However, in this leaflet, they were trying to promote its effects on blood clotting factors. Basically, doxazosin reduces fibrinogen levels and plasminogen activator inhibitor – 1 (PAI-1). Plasminogen is activated by tissue plasminogen activator (tPA) which then becomes plasmin, an enzyme that slices fibrin apart, and breaks down blood clots. PAI-1 stops this happening, so makes clots more difficult to break down.
To quote, again.
‘These recent studies suggest that doxazosin may have a range of significant antithrombotic effects in many patients, in addition to its proven beneficial effects on hypertension and hyperlipidaemia. Following doxazosin treatment, a reduction of platelet aggregation and a tendency towards dissociation, together with a reduction in fibrinogen levels, might prevent excessive degrees of thrombosis at the site of vascular injury. In addition, reduced levels of PAI-1, and increased tPA capacity with doxazosin might stimulate fibrinolysis and early clot dissolution at these sites, and prevent the evolution of an acute coronary event.’
So there, couldn’t have put it better myself.
Then Pfizer bought Warner-Lambert, who made atorvastatin/Lipitor. The focus became Lipitor and lipids, lipids, lipids. Lo it came to pass that Pfizer never mentioned blood clotting ever again, lest it interfere with the LDL story. Pity really, because mighty Pfizer got it right in 1992. Smith got it right in 1993, Duguid got it right in the 1940s, and Rokitansky was right in 1852. Of course, there have been many others who got it right too. Many, sadly, lost to history.
At some point this, the blood clotting hypothesis, the correct hypothesis will win. Maybe that time will be now.
Postscript
I realise some people may still wonder (if they have not read what I have written before) how the blood clot ends up within the artery wall/beneath the endothelium.
The reason is as follows. If the endothelium is damaged, a clot will form, sitting on the inside of the arterial wall. Once the clot has stabilised, and been reduced in size by fibrinolysis, the remainder of the clot will be covered over by Endothelial Progenitor Cells (EPCs) that float around in the bloodstream and are attracted to areas of endothelial damage.
After a layer of EPCs has grown over the clot, and converted themselves into mature endothelial cells the blood clot will now, effectively, be sitting inside the artery wall. Underneath a new layer of endothelium. Thus, clot becomes plaque.






 The Clot Thickens is available worldwide in Paperback and eBook through Amazon:
The Clot Thickens is available worldwide in Paperback and eBook through Amazon: