
Lead
I have been studying cardiovascular disease for well over thirty years now. I have come across a million different hypotheses about what causes it. There is almost no foodstuff, vitamin, infectious agent, chemical compound, atomic element or activity [lack of, or excess] that has not been proposed at some point.
Many of them can look very promising, and the underlying hypothesis is often elegant – very elegant indeed. But what you must do with any hypothesis is to hold it close to the unforgiving flame of mortality data, and see if it is tempered by the heat – or simply melts.
I resolved very early on in my long and winding study on cardiovascular disease that any hypothesis had to explain everything – not just some things. For example, as almost everyone in the entire world knows a raised cholesterol level is considered the most important cause of cardiovascular disease. But it is exceedingly easy to find facts that seem to completely contradict this.
Here, for example, is a little graph looking at only two countries. It compares the death rate from heart disease in Russia and Switzerland, in men under the age of sixty-five relation to the average cholesterol level in those two countries.
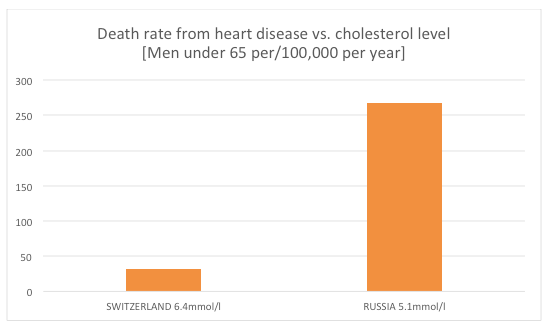
in Russia, with an average cholesterol level of 5.1mmol/l (197mg/dl) had a death rate 834% higher than that in Switzerland, which had an average cholesterol level of 6.4mmol/l (248mg/dl). Yes, this graph is the right way around. Yes, these data come from the World Health Organisation, and can be found on the British Heart Foundation (BHF) website. These particular statistics are now very deeply buried, but can still be found here: https://www.bhf.org.uk/publications/statistics/european-cardiovascular-disease-statistics-2008
I sometimes wonder if anyone at the BHF actually looks at these data, but that is a question for another day. Of course, when presented with facts like this, the dismissals. and creation of ad-hoc hypotheses rapidly reach into the sky. The word ‘paradox’ will be used pretty heavily, that’s always a good, temporary, escape route. In reality these two figures represent a full-blown black swan. But, hey, facts are slippery things.
Anyway, in my quest to explain everything about heart disease, perhaps the hardest single thing to explain is the fact that the rate of cardiovascular disease (heart attacks and strokes) has been going down in pretty much every single Western country for decades. I would say ‘first world’ country, but my son (a geography graduate) informs me that this terminology is now virtually barred for being racist. I shall be considered an ancient, prejudiced reactionary for using such a term.
So, I will say, Western Europe, North American, Australia, Japan, New Zealand and suchlike.
Now, the decline in CVD did not start at the same time, in all these countries. At this point I will make myself a hostage to fortune and make some sweeping statements. The rate of CVD peaked first in the US, in the late 1950s and has been falling since. It peaked next in Finland in the 1960s. In most of the other countries CVD peaked in the 1970s, before falling. It is impossible to say that there was a uniform worldwide effect. [Today, some countries are on the way up the mortality curve e.g. China and India].
However, I will make the general statement that CVD has been falling in most ‘first world’ countries for decades. This started long before any effective medical interventions were available. In the US, in the 1950s, there were no effective blood pressure lowering agents, no stents, no CABG, no clot busters…. Nothing really.
Possibly the greatest single factor has been the reduction in smoking. At the end of the second world war virtually all men smoked. Nearly 90% in the UK in the 1950s. Since that time the number of smokers has fallen, and fallen.
In addition to this, during the 60s, 70s, 80s and onwards, medical interventions have also greatly improved. In-hospital survival from a heart attack or stroke has improved almost year on year. The figures are complex, but around 60% of those admitted to hospital with a heart attack used to die – it is now around 30%, maybe less.
Some of this is due to the fact that ‘strict bed rest’ following a heart attack, the key medical intervention for decades, was abandoned. A piece of medical mismanagement that killed millions and millions… and millions.
What else may have cause the fall? I think that in the UK, the clean air act has a significant effect. The Great Smog of London, in the early 1950s, killed tens of thousands in less than a week. Much of this was from respiratory complications, but also CVD. It is now more clearly established that air pollution, in general, increases the risk of CVD. Most Western countries have drastically reduced air pollution.
Now, I would like to consider something almost never mentioned. Lead. That is the element, not the verb. Or the noun, as in dog lead.
In the 1920s someone discovered that if you put lead in petrol/gasoline it had all sorts of benefits on engine performance and wear and tear – and so on. Unfortunately, lead also caused all sorts of problem for human performance, and wear and tear. It is a heavy metal and, like other heavy metals, a powerful human toxin.
Despite the fact that lead toxicity was known for decades, it took until the nineteen-sixties before countries starting banning it from fuel – and pipes in housing – and the like. Which reversed a long-term trend of lead building up inside human beings. It lasts for decades within bone – gradually leaking out.
With regards to lead and CVD, is there a link?
A researcher called Weisskopf looked at the amount of lead in bones, and the rate of CVD. He found that those with the most lead in their bones were 837% more likely to die from CVD (relative risk)1 than those with the least lead in their bones. Now, whilst that is a relative risk, it is of the magnitude where we can safely say we are looking straight at a direct cause of CVD.
How does lead cause CVD. Most likely through the following mechanisms
‘Lead causes endothelial dysfunction by binding and inhibiting endothelial nitric oxide synthase and decreasing nitric oxide production.’2
Yes, we are straight back to my old friends, endothelial dysfunction and decreased nitric oxide (NO) production. In the world of cardiovascular disease, if you know where to look, all roads lead to NO.
If lead does cause CVD, is there any evidence that removing lead from the body can reduce the risk of CVD? [‘Reversibility’ and ‘Experimental Evidence’, the two most powerful of Bradford Hill’s canons for causation]. Which brings me to TACT. A trial designed to look at the impact of chelation on CVD. A way of removing heavy metals from the body…
What I love about this trial is that it was set up primarily to prove that chelation was nonsense, to be laid alongside homeopathy, and suchlike – by mainstream researchers. To quote an article in Medscape:
‘The original TACT trial wrestled with enrolment, ultimately taking over a decade to yield results, in part because cardiologists were absolutely convinced that chelation was a load of horse hockey.’ 3
TACT stands for Trial to Assess Chelation Therapy. When I first heard about chelation, I too, dismissed it as horse hockey. However, it turns out that I done the thing that I always advise everyone else against doing. I placed it in the ‘impossible/horse hockey’ category without making the effort of trying to find out what it was really about.
As it turns out, I should have made more effort…
‘TACT found that patients randomized to a regimen involving up to 40 separate three-hour infusions of a chelation-therapy solution (disodium ethylenediaminetetraacetic acid [EDTA], ascorbic acid, magnesium chloride, potassium chloride, sodium bicarbonate, B vitamins, procainamide, and a small amount of standard heparin) experienced an 18% drop in the trial’s primary end point (all-cause death, reinfarction, stroke, revascularization, or hospitalization for angina) compared with patients randomized to a placebo infusion.’3
More extraordinary than this:
‘When we broke the composite down to look at our secondary end points, we found that we had about a 40% reduction in total mortality, a 40% reduction in recurrent MI, and about a 50% reduction in mortality [in patients with diabetes],”’3
A 40% – 50% reduction in mortality. Well, well, well. Eat your heart out statins. In fact, eat your heart out every single pharmaceutical product ever tested. What has been the effect on mainstream thinking on CVD? As you would expect, absolutely nothing has changed in the slightest. Still TACT2 is now being set up – so we can all look forward to that being ignored in about seven to ten years’ time.
Anyway, in an attempt to bring some structure to this blog, I am going to return to the start. Why has the rate of CVD gone down in most first world countries over the last fifty years? One of the reasons, I believe, is that the level of heavy metal pollutants (in particular, lead) has been dropping since around the mid nineteen sixties.
I think it could be argued that the US was the first country to embrace the motor car. Thus lead toxicity would have hit the US before anywhere else. I am not going to argue this too strongly, but I place it before you, for your consideration.
I shall finish by saying that, if you want to look for reasons for the pattern on CVD over the last sixty years, or so, you really need to start looking outside the box. For there are more things in heaven and earth Horatio, than are dreamt of in your philosophy.
1: Weisskopf MG, Jain N, Nie H, et al. ‘A prospective study of bone lead concentration and death from all causes, cardiovascular diseases, and cancer in the Department of Veterans Affairs Normative Aging Study’. Circulation 2009;120(12):1056-64.
2: Natalia V. Solenkova et al: ‘Metal pollutants and cardiovascular disease: Mechanisms and consequences of exposure.‘ Am Heart J 2014;168:812-22

very good
Interesting. But if true, would this not suggest a clear pattern of increased CVD in built-up and polluted areas versus rural areas? Between the cities and the countryside?
Try looking at a map of CVD in the UK. Cities high, rural low.
But if lead is the main culprit there must still be an effect from other pollutant(s). (As lead is no longer in the fuel.)
And btw I live close to a busy main road 😦
I think my point is that lead is decreasing, but clearly not gone. It last in humans for decades. Also, I picked on lead, but I am certain that other pollutants are equally bad.
No surprise the results of the TACT study (and many others) have been ignored; whenever a study brings results that contradict what “everybody knows” (high cholesterol causes CVD etc), the mainstream comes up with one of my favourite statements – “yes, BUT we still recommend what we have been recommending so far, and more studies are needed in this area”.
Part XXVI: Mercury?
Mercury Exposure and Endothelial Dysfunction: An Interplay Between Nitric Oxide and Oxidative Stress.
https://www.ncbi.nlm.nih.gov/pubmed/26060268
Lead – it’s gotta to be another contender.
My situation is aircraft from 4 airports flying over head all the time, esp the light aircraft in summer and the M3 motorway just yards away.
Noise, pollution…both straining and stressing the body mentally and physically. How I hate modern life more and more…
Avgas or aviation spirit in the UK is used for piston aircraft and still contains lead. Jet fuel never contained lead, think of it as Diesel fuel 🙂
Leaded petrol for cars was phased out in the UK along with the rest of the EU in the late 90s, wasn’t it?
Just perused the wikipedia article on avgas. Some light aircraft with supplemental type certificate can ran on automotive petrol without ethanol. Also, many superlight aircraft use engines borrowed from other walks of life which can use regular car fuel. Also, a few car diesels have been certified, and guess what, they can run on jet fuel.
To re-invent a famous quote… There are facts, alternative facts, and statistics.
The TACT stuff is new to me, and very interesting – thanks.
Fascinating
A question from an ignoramus and slightly off the point – are CVD and arrhythmia two completely distinct diseases? Increasing numbers of friends in their 80’s have arrhythmia but their coronary arteries are squeaky clean. I suppose the answer could be simply ‘wear and tear’?
My mother who was incredibly healthy and into her 90s, was put on drugs for hypertension (that it turned out was only ‘white coat syndrome’) which gave her heart arrhythmia and syncope. After stopping the drugs, she started to get some heart problems (ie odd pains) and eventually suddenly died at 93 from a heart attack. I’m sure the hypertension drugs had some adverse effect on her, but we’ll never know!
Ann, do your friends eat a nutrient dense diet?
Lead, smoking, dirty air are all toxins – they consume electrons – as with pathogens – a.k.a. inflammation. This consumes Vitamin C = chronic sub-clinical scurvy! Fight inflammation and we fight heart disease – and most other diseases – chronic, acute or lifestyle diseases. Can it be that simple? Best way (not the only) to fight disease is with Vit C in suitable doses – the body’s primary redox agent. This is consistent with the known benefits (to IHD) of reducing carbs, avoiding toxins, and taking anti-oxidants (esp Vit C)? It’s all about electron balance, or to put it another way, the body’s voltage?
Hi I recently ha an exchange with Dr Mark Porter. I took exception to his recent article in the Times which more or less trashed the idea of people using Vitamin supp’s to combat disease. I challenged this firstly on the Vit C front (but also on others) and I am glad I did because you always learn something when you talk to people with opposing views. It gets you off your backside to investigate. Dr Porter kindly replied and sent me a link to a meta analysis that essentially showed that no Vitamin was beneficial in a statistically significant way in reltion to heart disease when supplemented, although selenium came pretty close. I decided to dig a little deeper into the meta analysis and in particular heart disease and Vit C category. I am convinced that Vic C can impact Lp(a) and hence CVD. When I looked closely at the 7 studies forming the meta analysis on Vit C I noticed that they had weighted them. Now I forget the exact method of weighting but it sure wasn’t based on dosage because one study was weighted with 78%!! of the overall value of the analysis and this study only used 250mg of Vit C per day on people with heart disease. This study came out as pretty much neutral on Vit C and given that the overall score OR was 0.99 for Vit C (the more below 1 the better) you can see that this one study had massive or should I say 78% effect on the outcome. As I said to Dr Porter, Linus Pauling would have laughed at 250mg even for healthy subjects. Incidently getting back to Selenium there is an interesting Swedish study that showed in subjects over 60 that a combo of Selenium and Coq10 slashed risk by 50%.
By the way Dr Porter is not talking to me anymore
This is very common. Give substandard dose and then dismiss the intervention as ineffective…
Smartersig
As you say 250 mg Vit C is pathetically low. However this is standard medical research practice. If they want to show x is better than y then they make sure the dose rate of y is as low as possible. In the case of vitamins the RDI are used because they know full well that RDIs are only of value in extreme cases of deficiency and are way short of optimal values. I have seen several studies where this practice has been used; the usual selection is OTC multivitamins which usually only contain RDIs. We are back in the 17th-19th century era of snake oil manufacture and snake oil salesment, astroturfing and agnotology http://www.bbc.com/future/story/20160105-the-man-who-studies-the-spread-of-ignorance
I can’t make him out. He posted seemingly pro-low carb after his experiment, but made some rather snippy replies to people who seemed to be encouraging him. He posted my reply and was almost insulting, then some time later he deleted it. Forgot to take it off the Wayback Machine though
https://web.archive.org/web/20160526203646/http://drmarkporter.co.uk/low-carb-diet-my-6-week-experiment-to-see-how-cutting-back-on-carbs-impacted-on-my-blood-cholesterol-lipid-profile
Then his blog went totally quiet after he had received the most replies EVER.
I wonder if he was spanked by the BBC or The Times or someone else, or threatened by dieticians.
He very much seems to alternate between sense and convention.
Excellent Malcolm – suspected this along with smoking reduction (a given) – but never dug studies on it – nice one ! Of course the monkeys take the credit for other people’s initiative – attributing outrageous amounts of benefit to their weak & ineffectual drugs…
If lead and other heavy metal pollution can be damaging to the heart, as it does appear to be the case, there is another idea that can help remove toxic pollution from the body. It’s an idea discussed earlier concerning NO.
Dr. Zane Kime in his book on sunlight therapy devotes a chapter to Sunlight and Pollution. On page 199 he has this to say:
“A number of noxious chemical agents have been tested including lead, mercury, cobalt, manganese, cadmium, fluoride, benzene, carbon tetrachloride, pesticides …. and dusts (quarts and coal). The amounts given is usually enough to cause a chronic intoxication.
The animals being given sunlight treatments eliminated some of the toxic chemicals ten to twenty times as fast as did the animals not receiving treatments.
Lead was removed twice as fast from animals receiving sunlight therapy as from others. The ultraviolet light seems to increase the enzymes that metabolizes toxic chemicals and help to remove them.”
The author goes on to write that in Russia, some coal mines require their workers to receive UV treatment. It was believed UV light helped keep their miners healthier. One way that came about was due to coal dust left miners lungs quicker when light treatment was applied.
Very interesting. I am, as you may know, a great advocate of sunlight as a healthy thing.
And, of course, we’re all told to stay away from evil sunlight because “it’s bad for us.” Doh.
And that’s why there is a chronic vitamin D deficiency in the UK and other ‘developed’ countries!
Anglosvizzera: lack of vit D leads to chronic health problems, and also an epidemic of osteoporosis, as calcium needs vits D and A to be absorbed and used by the body; both found only in natural fats, which, like sunshine, we are also told to abhor.
Fascinating stuff! Soul, that is very interesting too, and highlights the strong link between low vitamin D status and low levels of glutathione, the powerful antioxidant our bodies make and need to protect and detoxify cells.
There is a study however, looking at vitamin D and heavy metals in chickens – ‘The results obtained demonstrated that vitamin D3 caused accumulation of those metals in tissues and their toxicity in organisms. When increasing the vitamin dose from 200 to 500 IU on 1 kg of ration, that tendency was being heightened. On the three steroids which had been studied the metabolite 1,25(OH)2D3 displayed the greatest activity in accumulating metals in tissues, Pb in particular.’ Noooooo! How inconvenient! I wonder if it needs to be sunshine, and if so, why, or is this a peculiarity of chickens, or is something else is going on?
Interesting. Maybe Mike Cawdery can comment?
That’s a good question. I’ve read contradictory writings on supplementing with vitamin D3. Some highlight the positives found with it, and others the negatives, as you mention. The vitamin D council web sight I’ve found as a good source of information on vitamin D supplementation.
The book I mention does not want readers to take vitamin D supplements. The author mentions many times how taking vitamin D is different from light or sun therapy. there are obviously some similarities but the results seen between taking vitamin D supplements and sunbathing are frequently different, according to the author.
Eric
Sorry but I can’t give an explanation for this interesting information other than animals are generally pretty tough when it comes to self cure from all sorts of problems. I suspect that vitamins are part of this self-healing process..
Beautiful input as always 🙂
Talking about lead pollution, chemical lead compounds were used until rather recently as paint pigments. It is actually not the lead metal in itself which is poisonous. At the same time there there seems to be a sweet taste involved with these pigments and it is a “well known fact” that small children easily discover this when they are able to remove chips from painted walls and devour them. I think there are some jokes among children around this.
I though wonder how true this might be.
https://en.wikipedia.org/wiki/Lead_paint
Knowing that heavy metals are poisonous it surprises me, not least as a metallurgist, that one can drink tank loads of colloidal silver water without geting poisoned. It is as such considered as a “quack” remedy for cancer.
I though have my doubts about the “quack stamp” as when it is put on vitamin C. Especially when Big Pharma will now hunt every GP who would dare advocate this water as some king of remedy to his death. This water is in fact killing every kind of bacteria in aqueous solution and is also used in health care for treating burns.
Goran
Sharyl Attkisson in one of her youtube lectures points out that Wikipedia on medical issues is unreliable and manipulated by Big Pharma. Her specific complaint was where Wiki was at fault it was unable to edit/correct the wrong information – the edit was quickly reversed.
Wikipedia is never to be trusted – colleges and universities are always making this clear to students…
My only experience with editing Wikipedia bears this out.
Some years ago a company in South Africa was selling biodiesel plants to smaller municipalities who had no technical expertise, and the company had been exposed in the press as a scam operation.
The Wikipedia article on Biodiesel mentioned the company by name. I put in an edit with links to reputable news articles regarding the scam allegations. I verified that my edit appeared on the Wikipedia article.
A couple of days later I checked back and all mention that they were a scam had disappeared.
The medical regulator in Australia has ‘silenced’ a medical specialist doctor for encouraging his patients to quit sugar and junk food.
Göran, I think you are referring to lead acetate which is sweet but was to my knowledge not used in paints but only as a precursor for the pigments. I don’t think there were any lead containing paints available in the EU since the late 70s.
One notable exception may be Faluröd, the natural mineral pigment of which contains some lead. It is banned in many European countries but not Sweden and Germany, the argument being that that it contains only poorly soluble lead compounds. Still I worry a little about my garden shed which I repainted last year and which has a pear tree growing on one of its walls.
Lead compounds were also used as driers in many sorts of paint. (As well as compounds of other metals.)
“But what you must do with any hypothesis is to hold it close to the unforgiving flame of mortality data, and see if it is tempered by the heat – or simply melts.”
I don’t know if this came out of your own brains or if you ripped it off. But either way… nice.
I think it was mine, but I probably unconsciously stole it from someone else.
Personally I would put it down to the proper use of the scientific principle of the null hypothesis which these days is consistently ignored.
Oh, stop being so modest. It has exactly your tone of ‘voice.’ Brilliant.
Would it be OK to just micro wave it
Intriguing. There is a book, Malignant Medical Myths, by Joel Kaufman (if I remember it right) which goes into chelation therapy, and also agrees with what Dr K has said in previous posts about salt, statins and cholesterol. Maybe the anti-mercury dental fillings “cranks” also have a point? Thank you as always, Dr K.
And the anti-mercury in vaccines ‘cranks’ too? (Not to mention the aluminium salts in them….)
Gay,
There is an excellent point to having silver/lead amalgam fillings removed, indeed avoided in the first place. It has to do with the physical nature of the fillings rather than the chemical.
These amalgams are not adhesive, so the excavated cavities must be undercut to hold them. Healthy tooth material sacrificed! Amalgams are crystalline, changing dimensions over time. Small amalgams give way to larger ones as the margins succumb to gaps and decay.
Then, the larger amalgams, trapped in place by the undercutting, exert those inevitable forces on the weakened tooth and split it!
Personal experience. I had all my amalgams removed ten years ago. Six porcelain crowns and many acrylic composite fillings later, I have no amalgam, no mercury. I’ve no idea if the gone mercury made any sort of quacky difference, but my teeth are fine now. Everything is solid and stable.
Mercury in fillings is considered safe as long as you are alive. When you are dead it is a heath hazard and must be removed before you are cremated. Probably when you are buried too. Nice!
Gay Corran
Indeed this is an excellent book. He present 11 myths with many appropriate references. I have had a copy for years. Recommended,,, Along with Prof Goetzsche book Deadly medicines and Corporate Crime
Keep up the good work
Another excellent article. This may not be relevant, but as a child born in Bermondsey, South London in 1948 we were told to drink Jersey Gold top milk to help with the suppression of Smog in the fifties. We were given milk every morning at school. When I started as an apprentice in Fleet Street (printing plates were made of a mixture of 75% lead, 15% tin and 10% antimony) we were instructed to consume a pint of Jersey Gold top every day and had a medical and chest x-ray every year until we were 18. The importance of barrier cream on hands was also emphasised.
Malcolm,
I just wonder why those TACT infusions contained so many other ingredients – which seem to muddy the water – particularly perhaps the ascorbic acid.
Also, isn’t it possible to use CVD data relating to people who have never smoked – that would be interesting.
The trouble here is that we’ve all smoked – either actively or passively. Remember when the light in cinemas from the projection room was aswirl with cigarette smoke?
It is said that passive smoking is far less significant than active smoking.
I only took one puff of one cigarette – not because I was contemplating starting, but just out of curiosity! I think I could claim to be a non-smoker!
I grew up in a family of chain-smokers. Both my parents had severe and chronic bronchitis. Apart from an exploratory trial (it was the grown up thing to do) I never smoked but guess what? I seemed to have ‘inherited’ the family chest and now use two inhalers. The filthy polluted atmosphere of a Midland industrial city wouldn’t have helped, though I left and went to live by the sea in 1967.
P.s. My brother has ‘inherited’ the same family chest.
With smoking it seems to be the luck of the draw sometimes. I smoked a pack a day for 25 years from the age of seventeen before finally quitting, and drank heavily too. My cousin’s husband, the same age as me and a civil engineer like me, was a surfer. While I was sitting in a smoky pub talking rubbish with my fellow barflies, he was on some distant shore searching for the perfect wave. Put us back to back, I was the pasty-faced overweight one with bad posture, and he was the bright-eyed clear-skinned athletic blonde.
We buried him last year. Never smoked, but got lung cancer that spread to the brain, while I’m (touch wood) still healthy and active. But I did have to stop smoking and drinking or I’d be dead myself now, I’m sure of it.
Dr Kendrick
Another blistering attack on the medical research establishment and their ignoring of facts that they simply know nothing about – level of science taken up by other institutions as well.
I particularly liked the information on the TACT studies
As you would expect, absolutely nothing has changed in the slightest. Still TACT2 is now being set up – so we can all look forward to that being ignored in about seven to ten years’ time.
What surprises me is that money is available for TACT2.
I must say that as a researcher the official attitude to single instances of benefit have so changed from the 1940s. For example the first test of penicillin was in one man and they had to collect his urine to revover penicillin to continue his treatment (Dr LeFanu – The Rise and Fall of Modern Medicine) while these days many recover from “x” or “y” but medical research is not interested in looking at the reasons for the recovery. I suppose it is due to the ever perception of profit and to hell with human life
Very interesting that the CVD map shows a remarkable difference between urban and rural. Most people would have concluded that the variation was merely due to the ‘stress’ of city dwelling compared to the slow and easy idyllic surroundings enjoyed by country folk. Now there’s a more physical ‘kid on the block’ reason ie cleaner air. Pure and simple.
I wonder whether oral chelation supplementation would be an effective defence?
More trees everywhere please. In France wherever they do any alterations in towns they plant lots of trees, lungs of the earth. Family and friends have houses in this lovely country, north and south. Great read again Dr Kendrick, thank you.
My circumstantial evidence seems to tell me that people living in villages suffer from a host of tragic early diseases.
This is getting more gripping by the blog. I’m almost tempted to write to the BHF and ask them to explain their understanding of the graph about the big variations in death from heart disease vs cholesterol levels in Switzerland and Russia.
Give in to the temptation and write to them. I did some time ago and they told me they were right, even when they were wrong. You will find the reply on one of these blogs, but I don’t remember which one.
I wonder what the people of Mt. Isa, Qld., should do re lead levels in the blood; they do get plenty of sunshine in the Sunshine State. I keep referring your site to Trust me I’m a Dr. due to the poor science I view on this BBC TV show.
This is why I am not keen to eat vegetables grown on verges. Also, why do people sit on footpaths, outside cafes?
A really good hypothesis for testing, indeed.
Perhaps in addition to a direct effect on eNOS (as per your reference 2), it is worth noting that
Methionine synthase (as well as some of the methyltransferases) involved in homocysteine- and tetrahydrobiopterin- related metabolism are susceptible to blocking by lead (and other heavy metals). Tetrahydrobiopterin is essential for eNOS dimerisation and so for NO production, so that seems a fairly direct link (perhaps one among many). If that pathway is relevant, choline and betaine/TMG could be expected to be helpful. I’m not yet clear enough on the causality of homocysteine and CVD to comment on that aspect, but Hcy would be elevated which is a marker, at least.
My personal concern is that I have (according to my genes and other observations) somewhat messed-up metabolism in this area (methylation/BH4/eNOS) . The consequences of low-level heavy metal toxicity might well depend on genetic susceptibility. Food for thought.
Good point, and definitely ‘food for thought’. Epidemiological studies have established a positive association between high blood levels of lead and homocysteine, the latter already a known independent risk factor for CVD. Is at least some of the significance of high homocysteine because it may be actually signifying high lead?
Would like to mention here that it’s not just genetics and environmental exposure to toxins and gloom-and-doom, it’s the nutritional resources we consume and supplement to support our genes and cope with our environment. In a 2012 study which looked at lead, homocysteine and the micro-nutrients involved in metabolising homocysteine, the conclusion states: ‘the association between blood lead and homocysteine differed based on the levels of folate, vitamin B6, or vitamin B12 present in the blood. It may be important to keep sufficient levels of these micronutrients to prevent the possible harmful effects of lead exposure on homocysteine levels.’
Thank you! Your question is exactly what I was wondering. I found the 2012 study: “Association of Homocysteine Levels With Blood Lead Levels and Micronutrients in the US General Population” by Lee et al, J Prev Med Public Health 2012;45:387-393.
Very relevant and interesting (and open access).
For the mathematicians out there, one wonders if there is a way to correlate the decreases in certain things to the decrease in CVD in a mathematical correlation sense. In other words, could one say that the spike in CVD in Western countries in the 20th century was caused by:
CVD CAUSES 1900-2000 (Western world)
Smoking – 60%
Pollution – 15%
Transfats – 10%
Heavy metals – 6%
Other – 9%
Moving forward, the top 4 causes have now decreased, so not only has CVD decreased overall, the causes of CVD have changed. The mathematician might find the following:
CVD CAUSES 2000 – forward (Western world)
Smoking – 20%
Pollution – 5%
Transfats – 3%
Heavy metals – 2%
Other –
Genetics – 20%
Obesity – 40%
Other – 10%
The point, of course, is when one starts decreasing the main cause of something, the something will decrease, though not to zero. The decrease in causation of one thing, however, will cause causation in another to increase (assuming it is also not decreasing as a cause as well.)
So all things being equal, if you take away all external causes of CVD, one will be left with the genetic propensity to eventually die of CVD. This causality will continue to rise as the others fall.
Sorry for the long-length of the reply – just my 2 cents worth. 🙂 And thank you Doctor again for your openness and skepticism. A true Dr. indeed!
The various causes do not have the same rate (with respect to age). So as the major causes of concern reduce, people may live longer or die of other causes rather than the cause of concern.
Will we be concerned if we get it down to one death from CVD with a 100% cause by genetics ?
Interesting. I wonder where sugar and raised insulin would feature in the list of CVD causation?
Malcolm Kendrick:
“People create ad-hoc hypotheses at great speed, without any requirement for data – I find”.
Toxic corrosive fluoridation chemicals leach lead from plumbing into tap water.
http://www.ewg.org/enviroblog/2009/07/chloramine-lead-pipes-fluoride-contaminated-tap-water
Fluoridation chemicals contain heavy metal contaminants including traces of lead.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4090869/
Lead in gas, lead in paint and lead in plumbing all decreased in the US over the last 60 years, due to the efforts of a lot of people and the EPA. I wonder now that the EPA is under attack from the new administration will a rise occur over the next 60 years if the lead restrictions are repealed by the regulation hating folks?
I worked with an alternative practitioner in Savannah, Georgia and he used chelation therapy on patients that were too sick to undergo coronary bypass grafting..they swore by it.
Great post!
Off topic but of interest in view of all the ingredients in the TACT fluid this may be of interest:
Neurology. 2014 Sep 2;83(10):920-8.
Click to access NEUROLOGY2014574723.pdf
Vitamin D and the risk of dementia and Alzheimer disease.
CONCLUSION:
Our results confirm that vitamin D deficiency is associated with a substantially increased risk of all-cause dementia and Alzheimer disease. This adds to the ongoing debate about the role of vitamin D in nonskeletal conditions
and in my opinion the importance of low cholesterol due to statin therapy in Alzheimer’s
Interesting, Mike.
Still off topic – apologies, because the proper topic is of such interest, but my query is to do with February.
My husband and I have developed a bit of a suntan from walking about outside this month. But the sun is supposed to be far too low in the sky during February in our latitude (approx. 52 degrees north) to produce a suntan (and hence vitamin D). Does this mean the experts could have it wrong or does anyone know if the suntans could be protecting us from some other part of the spectrum – some wavelengths other than ultraviolet B?
Yes, UVA will make you tan, which is why most tanning beds use them. UVB doesn’t penetrate as deeply, but is more likely to cause you to burn, but only they generate the vitamin D, from our friend cholesterol on our skin, in a genuinely photosynthetic process (and it was once thought only plants could photosynthesise!) Anyway, UVA will get through the atmosphere even when the sun is low in the sky (more atmosphere to pass through due to the angle). UVB rays are pathetic weaklings by comparison, and get blocked by the atmosphere, clouds, pollution, glass, factor 8 sunscreen etc., which is why you’ll make the most vitamin D when the sun is at its highest in the sky. A good rule of thumb, at any time of year, is to check whether your shadow is longer than your height – if it is, you’re not going to be making vitamin D. Finally, if you’re tanning or burning surprisingly quickly, might be worth taking some Astaxanthin, an excellent all-round antioxidant and internal sunscreen.
TS,
You can get a suntan without making vitamin D. Darkening of the skin is caused by UV-A, but vitamin D is generated by UV-B. UV-B is absorbed by the atmosphere and thus varies a lot as the sun gets lower or higher in the sky. UV-A is much more constant.
The UV-A tan is fairly light and doesn’t last because it only oxidises the existing melanin in your skin. If you get UV-B as well, it creates more melanin for the UV-A to darken, giving you a deeper and longer-lasting tan, which is why tanning beds produce both UV-B and UV-A (not that I am recommending tanning beds).
Information from https://en.wikipedia.org/wiki/Sun_tanning
Thank you Emma and Martin for explaining so well.
TS
As Emma and Martin point out . . . the February tan you have will have been created by UVA, and the UVA does not enable the skin to produce vitamin D.
Sadly, the sort of tan UVA light produces is not very protective either. I found this conclusion some time ago in a study comparing UVA and UVB on human skin (a bit on the dry side). . .
.. “Photobiological implications of melanin photoprotection after UVB-induced tanning of human skin but not UVA-induced tanning” – Coelho
“It is quite clear that UVA-induced tans fail entirely to provide any photo-protective benefit, even at the level of a SPF (sun protection factor) of 1.5. This coupled with the fact that UVA-induced tans do not involve increased melanin production (Wolber et al., 2008) but rather its redistribution along with other aspects previously discussed elsewhere (Choi et al., 2010; Miyamura et al., 2011), underscores the misleading concept of a perceived benefit from tans produced by UVA-rich sunlamps”
So, the protective effect of the UVA tan is less than factor 1.5 sunscreen. Even so, the power of the Sun at this time of year is rubbish, so it hasn’t stopped me from making the most of the little sunshine we have had. And, there are other wavelengths that do good.
A picture is worth more than a 1000 words . . . so I would strong encourage anyone to look at the YouTube video . . .
“Vitamin D: UV, The Original Source – How to Use It” Edward Gotham
It talks about the beneficial effects of vitamin D, and starting at 25:00 min goes through the details of the different effects UVA and UVB have on the skin; then finishes with the problems of sunscreens.
good find!
Brilliant, Dr Kendrick, one of the best posts yet in this gripping series (please tell me this whole series will become a book eventually?)
Well done and thank you.
You’re onto something there, Malcolm.
Very interesting as always. Must send you my thoughts on NO.
“Russia banned the use of leaded gasoline nationwide in 2003 with the Federal Law on Banning Production and Use of Leaded Gasoline in Russian Federation.” http://transportpolicy.net/index.php?title=Russia:_Fuels:_Diesel_and_Gasoline
>
Yeah, that’s odd. Also, unleaded gas was first introduced in the US in 1972 and leaded phased out in the late 80s. If that was one of the major causes of CVD, why did rates peak in the 50s?
What caused rates to peak in Finland in the 60s when unleaded didn’t arrive until the 80s in Europe, and leaded was phased out in the late 90s? How was Finland different from Sweden? Both had a pretty low population density and few large towns, so that most folks were not exposed to high concentrations.
Many thanks, Dr. Kendrick, for another fascinating and informative post.
I curse you Dr Hendrick . . . but in a nice way.
I came across your blog just a couple of weeks ago. It makes captivating reading, even exciting reading. So I have been trawling through past postings – following up references – along with seeking out tutorials on blood clotting (so your comments on the LP(a) make sense).
As a retired teacher – ex-statin user – ex T2D sufferer – some mild heart problems – I have spent more time on researching these areas (CVD, diabetes, statins, alzheimer’s) than many would say, for a punter, is sensible. But hey, its better than sitting around doing sudoku; however, the wife is getting a bit edgy about the recent stall on the loft insulation project . . . and the garden . . . and putting up the new greenhouse.
So, having already a multitude of strands of research on the go, I now have your blog to add to the list of must-reads.
I appreciate your questioning approach, and that seems to include questioning your own ideas.
So now I must go and look up the TACT reference to see how they isolated the effect of EDTA as a chelating agent from the other chemicals in the therapy solution . . .
Many thanks for adding new dimensions of interest.
I know Harvard has rather lost its reputation for independent research/comment in the nutrition field and maybe heart disease too
But here it is coming doing heavily against chelation therapy post TACT
http://www.health.harvard.edu/blog/chelation-therapy-offers-small-if-any-benefit-for-heart-disease-201303266030
Just saying.
Jerome
Email changing Email changing Email Changing
My new email is: jerome@jburne.org
Myzen email being phased out
Please add to your contacts
40 Warrington Crescent
London W9 1EL
W9 1EL
0207 286 9294
07940 393 094
Blog. HealthInsightUK.org
Makes me a tad suspicious about who’s pulling the strings of the JAMA – “A home run for chelation therapy? Not according to the three top editors at JAMA. In an unusual editorial accompanying the TACT paper, the editors say that the results “should serve to dissuade responsible practitioners from providing or recommending chelation therapy for patients with coronary disease and should discourage patients with previous MI [heart attack] from seeking this therapy with the hope of preventing subsequent cardiovascular events.”.
It was a massive home run for statins, all the way to the bank, no dissuading of responsible practitoners with “unusual” editorials went on there. We’re all still waiting for Sir Rory to enlighten us, instead of shouting informed criticism down with “millions of lives…”.
I once read that death rates among non-miners in lead-mining towns show no particular ill effects from lead. So I’ve just looked up Broken Hill on Wikipedia. Although the article grumbles about high levels of lead in dust, and in children, it cites not one figure to suggest ill effects, serious or otherwise. Can one draw an inference from that? I doubt it, it’s only Wikipedia.
Does anyone here know about this topic?
I wouldn’t be surprised if most anorganic lead compounds were a lot less dangerous than organic compounds such as found in leaded gasoline.
Hi Dr. Kendrick
I am a retired dental surgeon actively investigating the possibility that my dilated cardiomyopathy was caused by mercury toxicity.
A 1999 study showed that heart muscle contained 22,000 times more mercury in dilated cardiomyopathy sufferers than matched controls with similar dysfunction of different cause. There was also high level of antimony. This research has never been followed up. (why?!!!) http://www.onlinejacc.org/content/33/6/1578
A 2012 study looking at the health records of 600 dentists found that they were at a very much increased risk of neurological (7.6 times), psychiatric (2.4 times) , cardiovascular (1.7 times ) and respiratory disease (1.5 times) compared to matched controls. http://bit.ly/2lGZ42E
Aren’t there little gizmos to gather up dust and fumes? At least this is what I see in a dentist’s surgery these days. Never had a filling myself, though.
One of my previous dentists was aware of the connection between lead and various diseases in dentists from way back. He switched to using polymer (?) fillings, then discovered they also outgas various toxic substances enough to affect dentists who work with them a lot but probably not enough to affect patients.
Of course when I wrote “lead” I meant “mercury”! The fumes are getting to me . . .
More fascinating reports, I love your posts please continue the battle against group thinking barriers.
You opened with “that any hypothesis had to explain everything – not just some things” Unless the hypothesis is, damage to the endothelium layer explains everything another variable has been added. Environmental toxins such as “lead” are modern variables and don’t explain heart attacks earlier in history. If someone wants to look at “map of CVD in the UK. Cities high, rural low” the stress from city noise or crowding could also explain that variable.
If you want to look under a rock that has been given little attention – I don’t think you will find a single person with heart disease who has a normal, relaxed respiration rate. I would challenge you to pay attention to the respiration rates of your patients with known CVD. I think you will find that all are at or above the top end for normal respiration and most if not all are mouth breathers. (Mouth breathing can be hard to spot)
The washout of Co2 from over breathing greatly reduces nitric oxide thus setting up the endothelium for constriction and serious damage. It is controllable (seriously) while toxins like “lead” may be less so. Over-breathing is also something that could explain everything…
“” relaxed respiration rate””. Is respiration rate the same thing as pulse rate? Or are you speaking about how many breaths per minute these people take?
Breaths per minute…
I believe Buteyko method of breathing emphasizes your point about overbreathing especially with regards to those with asthma.
Yep – it’s way too simple for most (99.9%) doctors to even begin to grasp. However the ones that believe that nitric oxide (or lack of) is involved in CVD should look hard at the relationship of carbon dioxide and NO. Over-breathing washes out Co2 and thus tanks NO. It’s not sexy like the other theories floated so it’s likely to continue to be ignored. Simple sugars increase respiration rates without a connection to activity and the list goes on. Years of sugar abuse resets the bodies tolerance for a lack of Co2 while at the same time washing out nitric oxide. Again – just too simple for doctors to get.
Thanks – and I look forward to another large number of intersting and informative replies too.
Interesting.
I’ve started seeing a naturopath rather than an M.D. to manage my hypothyroidism when I couldn’t convince the M.D. to prescribe anything other than T4. I’ve gone along with her recommendations as far as diet and supplements, but I drew the line at chelation. Perhaps I should reconsider.
Powerful. Lead began to be used in gasoline in the 1920’s. and the meteoric rise in CVD in the U.S. began in 1920. President Eisenhower’s heart attack in the mid-50’s likely had an influence on the reduction in smoking. From 1968 CVD rates began to drop like a rock, and despite an upward blip in the late 70’s (likely in part due to the economic crisis), have been dropping ever since.
Yes, but unleaded gas was not introduced until 1972, and I can remember from my first trip to the US in 1983 that leaded was still very much available, and that folks would let their V8s idle everywhere, at the drive in bank, drive in restaurant, just sitting in the car park waiting for someone with the A/C running (and if the wind came from behind, they’d vent their car with their own exhaust. Mind you, those V8s had a might idle burn rate, and in those days there were still plenty of cars with a carburator and no catalytic converter, so you’d get unburned tetra-ethyl lead, too.
There were (and likely still are) also those nutcases who took out their convertor on purpose.
There’s another interesting correlation with lead, that is crime, http://www.motherjones.com/environment/2016/02/lead-exposure-gasoline-crime-increase-children-health
I can’t find the references, but I recall reading that earthing can chelate heavy metals – another woo-woo protocol that may need to be considered?
This is taking me back to my childhood when we lived in an old house in what was, back then, real countryside. My father always stressed that in the morning we should let the tap run for a while before making the tea for breakfast. This was because the water supply came through lead pipes.
Many years later, my daughter was in hospital, and a little boy in the cot next to her was being treated for lead poisoning; he evidently had a habit of chewing the bars of his cot, and the paint had obviously contained lead as Dr Goran mentioned earlier.
To this day I still allow the tap to run from force of habit, even though the water supply now comes through plastic pipes. Old habits die hard.
Really interesting blog Dr Kendrick. Thank you, and one that I didn’t need to go to the medical dictionary to understand on this occasion!
Doctors are being attacked for using chelation in autism therapy, too. The proximate cause of autism is neurological injury, and clearly an overload of metals (primarily mercury and aluminum) in the wrong place, such as the brain, are a primary cause of this. And, like HBOT, it can be helpful, so it must be attacked.
Your comments jumped out at me because I had very serious Mercury poisoning as a baby and nearly died. In addition my mother always cooked with aluminium cookware, so I probably absorbed lots of it until I was 23 years old. I am now 68 and can assure you that I am not autistic.
Anita Thompson: Throughout human evolution we have ingested aluminum, since it is one of the most abundant elements in Earth’s crust. Thus we have developed a highly effective biological capability to excrete it; we absorb only about 0.3% of the Al we ingest. Injecting it into muscle tissue, though, is an entirely different matter. Nano particles of Al salts are used in vaccines as an adjuvant, to stimulate a stronger immune response than the antigen would by itself. Foreign invaders in the human body are customarily attacked by specialized white blood cells called macrophages, engulfed, and dissolved by their enzymes. These enzymes are incapable of dissolving metals, so they can carry the particles to the organs, including the brain, and deposit them, Trojan horse style. Two sources of peer reviewed science on this subject: vaccinepapers.org and a 2015 medical textbook, “Vaccines and Autoimmunity” (chapter summaries are available on line for free). I am the same age as you. We got only a few vaccines, and none in infancy. In the U.S. today, in the first year of life, infants are given 23-26 vaccines. This has no immunological value, since infants are incapable of producing antibodies for the first 12-15 months. It is done to “train the parents” that regular visits to the pediatrician are essential for their child’s health. Mercury is an entirely different matter. There is a press conference starting 20 minutes from now, at the National Press Club in Washington, D.C. with Robert F. Kennedy Jr., Robert DeNiro, and Nico LaHood, and moderated by Sharyl Attkisson, concerning the World Mercury Project. I’ll be watching.
Gary, please let us know what you see. If you have time…
Sasha: The press conference involved the World Mercury Project offering a $100,000 challenge to a journalist or anyone else who can produce a single published scientific paper showing that it is safe to inject the amount of mercury in a vaccine (multi-dose vials of the flu shot contain 25 mcg per dose) into infants or pregnant women. If the vial is not properly shaken, the last dose or two can contain a larger amount. A bit of a gimmick, but a meaningful one. The ethyl mercury in thimerosal is twice as persistent in the body and five times as toxic as the methyl mercury in fish, yet doctors tell pregnant women not to eat fish, but get your flu shot. A large percentage of the flu vaccine is distributed in the U.S. in multi-dose vials. The majority of them likely go to clinics which serve the poor, but you never know; could be your local Walgreen’s uses them. Mercury is so toxic it should never have been used in medicine, yet it remains in vaccines at the behest of CDC and WHO. GSK, that paragon of virtue, sent a letter to CDC offering to produce all of its vaccines without thimerosal, but CDC turned them down.
Gary: thank you. I would never consider getting a flu shot but the push is relentless – Costco gas stations, 10% off groceries at a supermarket if you get one, etc etc…
There’s a good documentary going on now The Truth About Vaccines. One free episode per day. You probably know about it but let me know if you need a link…
What about radiation exposure? Does the radiation from airplane travel cause higher hear attacks in people that fly more oftern>
Aircrew are exceptionally healthy but this may be healthy worker syndrome. Aircrew and passengers with plenty of long distance travel will have messed up circardian rythms, and that is going to have a far larger effect on CVD than cosmic radiation.
Also, plain gamma and neutron radiation is probably overestimated by the LNT (linear no threshold) model. There was even a high rise building in Taipeh that was accidentally built with contaminated steel. When this was discovered years later, inhabitants were screened and followed. They had some abnormalities in their bloodwork but no increased cancer rates. Similarly, areas with high natural background radiation do not have increased cancer rates. I am not aware of a study of CVD in areas with high background radiation.
It is ingested radiactive parcticles that emit alpha and beta radiation from within your body that you need to worry about.
Thank you for this information. I have always wondered if the increased radiation in the atmosphere since the 1950s, due to bomb testing and power station accidents, along with medical xrays could be one explanation for the dramatic increase in various forms of cancer.
Anita, there is no increased radiation in the atmosphere except for a couple of weeks after atmospheric bomb testing (which was discontinued ~50 years ago) or after a power station accident, which fortunately happens only every 20 years roundabout, as this requires radioactive particles to be suspended as aerosoles.
Food, yes, but moderate, depending on where you live. Soil / dust again could be critical in some parts of Eastern Europe or Japan.
Medical radiation, yes, but with the exception of tests where they inject you with an alpha decaying isotope, probably overrated by the NLT model.
I remember Strontium-90 was always the big bogeyman during the nuclear test era, because it is calcium-seeking, and goes from grass to cows to milk to children’s bones.
A study of hundreds of thousands of deciduous teeth, collected by Dr. Louise Reiss and her colleagues as part of the Baby Tooth Survey, found a large increase in 90Sr levels in through the 1950s and early 1960s. The study’s final results showed that children born in St. Louis, Missouri in 1963 had levels of 90Sr in their deciduous teeth that was 50 times higher than that found in children born in 1950, before the advent of large-scale atomic testing. Commentators on the study said that the fallout was likely to cause increased cases of diseases in those who absorb strontium-90 into their bones. — https://en.wikipedia.org/wiki/Strontium-90
Wow! Yet more essential food for thought, This blog should be required reading for all involved in healthcare.
I find it sad that few seem to recall Professor Derek Bryce-Smith who, so far as I recall, was the first to expose the dangers associated with lead in paint and petrol.
His obituary is interesting: http://www.telegraph.co.uk/news/earth/environment/8671336/Pollution-triumph-of-the-inconvenient-truth.html
Ray
There’s a strange and fascinating connection between the reduction in lead in the air and a reduction in violent crime. I’ve published some criminology and was sceptical to say the least, but the data stands scrutiny and has been the subject of science reports on the BBC’s PM programme.
By the way, lead was previously used in petrol as a lubricant.
http://www.bbc.co.uk/news/magazine-27067615
I think polyunsaturated fats like sunflower and corn oil and trans fats began to fall out of favor about the same time unleaded fuel was introduced, just look at Mary Enig’s piece on canola on westonaprice.org.
Interesting piece by Enig but why worry about which oil will do the least damage, simply take Dr Esseltyns advice NO OIL!!, no matter what the variety
His diet is pretty strict
So far, I have considered olive oil, if not Italien from a known source, to be pretty safe.
As always the blog is brilliant and as usual it raises interesting and thought provoking comments and references. One of my complaints against the medical research establishment is its apparent inability to independently research the mass of data that is in its keeping. At one time there were proposals to sell personal data. As I stated in a rapid response in the BMJ this would be a disaster as Big Pharma would buy, cherry pick it and then inevitably make it impossible for anyone else to see the data as it was “confidential”.
Properly examined this NHS data could confirm a lot effects on heart disease, diabetes, obesity, Alzheimer’s (now the No 1 killer in the UK) etc., etc. Will the NHS data ever be reviewed by independents – probably not. It will be sold, probably by the back door.
Mike, a propos gathering data from the NHS, (sorry, slightly off topic) when people I know die earlier than expected, my first thought is “were they on statins?” Not a question one can easily ask at such a time. But their medical records might be very interesting. Such data gathering really ought to be done. I know people who were on statins who died or nearly died of heart failure, MI, stroke, rupture of the aesophagus, pancreatic cancer; and I know people, including myself, who became diabetic while on statins. At the very least, the statins did not protect those people. Apologists for statins sometimes suggest that without them, the outcomes could have been worse in those who lived; unprovable, and doesn’t wash where the subject died, of course. It would be interesting, possibly revealing, if we knew of any correlation, (i. e. how many patients died, from what event, not from advanced age, while on statins) from GP medical records.
A good idea Gay . . . but call me cynical . . . it would cost money and effort to set up such a study and when you have so much invested in the statin juggernaut it is hard to do anything to jeopardise things. If those in charge suggested such a study some among them would feel threatened and fear that they may be shown to have been wrong headed all along.
Yes, Antony, cynical you are. And right. But when, in thirty years or so, statins have been abandoned because so many people have become ill on them, then someone will start to look at all the medical records which will show illness and mortality rates while the poor mugs were on statins. Like me, becoming diabetic while on simvastatin and following the GP recommended diet, and my husband having a TIA while on the same drug. Meantime, millions more will suffer and die for the sake of the pharma companies’ profits. Let’s hope Dr K’s research and brilliant, cogent, humorous writing reaches more and more ordinary people like us, who used to trust our doctors.
Thank you Dr. Kendrick for the time you spend into this fascinating topic of heart health!
It made up for another fascinating read.
The column in the periodic table starting with carbon goes carbon – silicon – germanium – tin – lead. If I remember my high school chemistry that means that tin and lead could muscle carbon aside and take its place, creating a different molecule.
Tin and lead have been very widely used in tin-plated steel cans with lead solder seals that a lot of food is preserved in. These days the inside of cans is lacquered and a non-lead solder is used, but these are recent innovations. In the early years tin cans were probably a prominent source of tin and lead ingestion. (Not sure of exact timelines.)
Those leaded cans were implicated in the Franklin arctic expedition of 1845…
I think so far down the periodic table things get a bit less clear-cut. It appears that lead can have either 2+ or 4+ states, and my understanding is that a lot of the problem is due to its calcium (Ca2+) like behaviour (rather than more carbon-like arrangements, although tetra-ethyl-lead is of this form).
Yeah, that’s typical of those metals. Can’t decide which oxidation state they want to be in.
OT, but when I see a chemical name like disodium ethylenediaminetetraacetic acid, my eyes glaze over.
I wish chemists would adopt a suggestion I heard many years ago from a computer programmer: like what is done in the computer world, use capitalisation for clarity. So for instance the above could be written DiSodium EthyleneDiAmineTetraAcetic Acid, which is much easier to read and pronounce, even if you don’t know what it means.
But then, every profession loves its obscure terms that binds it together and keeps the outsiders out…
Great review! Interesting! Thank you for sharing!
VERY interesting! I recall a plastics factory where one of the powders contained lead and the guys working with it were also given a pint of milk a day, and laid off whenever their lead levels (which were regularly tested) went too high.
Of course if this plastic was used to make water pipes there’d be a bit of an own goal.
Certainly we had lead water pipes when I was young, can;t remember when they were replaced, originally I think with copper, plastic came later. They would have been pretty endemic, and I also recall the early morning water tasting sweet probably as it had stood in said pipes overnight.
Likewise like a couple of other contributors my thoughts also turned to mercury in dental fillings, would be interesting to know the timescale of this being adopted and unadopted again. Also the organochlorines which predated the current organophosphate pesticides. And the water fluoridation, fluoride being so reactive might affect the solubility of heavy metals.
Hmmm!
Actually though it was the butter all along – according to New Zealand this is why CVD has started to increase again there
https://profgrant.com/2017/02/02/rebuttal-to-rod-jackson-are-new-zealanders-the-worlds-leading-butter-eaters/
Terribly tricky stuff this butter you know, even when you eat less of it it actually works as if you are eating more of it . . .
Only recently has lead been phased out as an ingredient in the manufacture of PVC piping in some countries, which means that older installations will still have pipes containing lead compounds. And I think it might still be used in the manufacture of stormwater pipe and fittings so if you collect rainwater for drinking via plastic pipes … ?
http://www.pvc.org/en/p/lead-stabilisers
Craig.
Except pipes for fresh water are made from HDPE.
Eric, in which country? Still PVC where I live.
Just add this to the mix. I read a while back about a Finnish study showing reduced mortality including heart attacks in men having saunas. It was dose dependent too – more saunas, less death (or should I say, later death). Could be all sort of reasons, but one might be the deep cleansing of the body through the skin of things like lead.
-Great post. Thank you!
Just discovered this: “Whey protein lowers blood pressure and improves endothelial function. . .
ajcn.nutrition.org/content/early/2016/10/25/ajcn.116.137919
If you’re pardon the pun, that’s whey out there!
Unlikely, knowing what else wheat protein does.
I guess it is proper to mention the observations of “all” colonial doctors, including Weston Price, about a hundred years ago and onwards who noted that no indigenous people did have “any” of our “modern diseases”. But as soon (10 -20 years?) they were exposed to our European nutrition habits, including canned food with lead containing solder in the can??, they got them all.
My own prime suspect would be the sugar together with the white flour which were both addictive food elements and with poor nutrition value. They also brought havoc to the dental status as Weston Price so eloquently documented with his photographs in the 1930-th.
I was strongly reminded of a blog post by George Henderson, it took a while to find it and collect associated materials:
http://hopefulgeranium.blogspot.co.uk/2015/05/chemical-atherogenesis-alternative.html
In this other endothelial or eNOS poisons are considered from a similar point of view.
Compare and contrast?
Here are some papers that I found of interest (the first from the above blog post): “Chemical Atherogenesis: Role of Endogenous and Exogenous Poisons in Disease Development” by Ross, Matthews and Mangum, Toxics 2014, 2(1), 17-34; doi:10.3390/toxics2010017 (open access) is worth a look.
The paper is complicated, has missing links, and has distractions (perhaps that’s only in my view).
There is a list of toxins associated with atherosclerosis development Acrolein, allylamine, arsenic benzo(a)pyrene, other PAHs, bisphenol A, PCBs, cigarette smoke constituents, vinyl chloride and air pollutants (particulate matter, ozone, and NOx). I don’t read much into a lack of lead and others toxins on this short list.
Another interesting paper is “Subchronic Toxicity Organophosphate Insecticide induced Damages on Endothelial Function of Vessels in Rabbits by Inhibiting Antioxidases”
by XIONG Xiao-Ming et al Progress in Biochemistry and Biophysics 2010, 37(11): 1232~1239
In which some hypotheses are raised and effects in rabbits explored showing several mechanisms at play (some gene/snp dependent).
Finally the paper “Mercury Exposure and Endothelial Dysfunction: An Interplay Between Nitric
Oxide and Oxidative Stress” by Swati Omanwar and M. Fahim, International Journal of Toxicology 2015, Vol. 34(4) 300-307 has many interesting connections and comments.
Overall I’m a bit surprised how rarely (failure of) dimerisation of eNOS comes up (it brings in a whole other set of genes that may affect susceptibility to any vascular/NO troubles). NOS monomers make superoxide not NO, and if there are some dimers producing NO the superoxide and NO react to form peroxynitrite (bad news thrice ).
I thought “Heavy Metals and Human Health: Mechanistic Insight into Toxicity and Counter Defense System of Antioxidants” by Arif Tasleem Jan et al, Int J Mol Sci. 2015 Dec; 16(12): 29592–29630, was going to get there, but not quite (still an interesting paper).
I have too much respect for the human body to believe that, with the loss of the ability to make vitamin C, it didn’t find some way to compensate. After all, it’s been an awful long time without the knack.
It was intriguing to find that there appears to be a close relationship between vitamin C and uric acid and that uric acid may help to compensate for lower levels of vitamin C. Here are just a few things I found:
Reduced-serum vitamin C and increased uric acid levels in normal-tension glaucoma.
https://www.ncbi.nlm.nih.gov/pubmed/19763599
“Normal-tension glaucoma patients had lower serum levels of vitamin C and increased levels of uric acid.”
(Could uric acid be stepping up because ascorbate levels are low?)
Uric Acid and Oxidative Stress
http://www.ingentaconnect.com/content/ben/cpd/2005/00000011/00000032/art00006
“This review presents the current evidence regarding the antioxidant role of uric acid and suggests that it has an important role as an oxidative stress marker and a potential therapeutic role as an antioxidant.”
Uric acid and serum antioxidant capacity: a reaction to atherosclerosis?
http://www.sciencedirect.com/science/article/pii/S0021915099002142
“The higher serum uric acid concentration seemed associated with elevated total serum antioxidant capacity among individuals with atherosclerosis. This finding is consistent with experimental evidence suggesting that hyperuricemia may be a compensatory mechanism to counteract oxidative damage related to atherosclerosis and aging in humans.”
The effects of vitamin C supplementation on serum concentrations of uric acid
http://onlinelibrary.wiley.com/doi/10.1002/art.21105/full
“Supplementation with 500 mg/day of vitamin C for 2 months reduces serum uric acid, suggesting that vitamin C might be beneficial in the prevention and management of gout and other urate-related diseases.”
Conservation of vitamin C by uric acid in blood
http://www.sciencedirect.com/science/article/pii/0748551485900157
“These experiments suggest an important physiological role for urate in preserving ascorbate in blood and other biological fluids.”
And I throw in this, just to be a little on topic:
The Role of Lead in Gout Nephropathy
http://www.nejm.org/doi/pdf/10.1056/NEJM198102263040905
“Until recently, renal disease was considered a major cause of death among patients with gout. Modern long-term follow-up studies of renal function, however, have indicated that hyperuricemia and gout rarely result in kidney damage unless other renal disease supervenes. These conflicting views of the occurrence of renal disease in gout might be reconciled if a single agent could be identified as a cause of both gout and renal disease in some patients. Lead is a likely candidate for such an agent, since this heavy metal has long been recognized as a causative factor in both gout and nephropathy.”
A big P.S.
Does this sound familiar?
Uric acid is a final enzymatic product in the degradation of purine nucleosides and free bases in humans and Great Apes. The pathway of purine catabolism in humans is shortest among vertebrates because about 8–20 million years ago during primate evolution the activity of urate oxidase (uricase, an enzyme catalyzing conversion of uric acid to allantoin) was lost in a two-step mutation process.[1,2] In other mammals, the last enzymatic product of purine degradation chain is allantoin, which is excreted in the urine. Lower vertebrates (e.g., fish) have enzymes that further degrade allantoin to allantoic acid and glyoxylic acid and finally to urea. As a consequence, humans have to cope with relatively higher levels of uric acid in the blood (200–400 μM) and are prone to hyperuricemia and gout.[3]
According to a hypothesis championed in the early eighties by Ames et al.,[4] the silencing of the uricase gene with an increase in the blood level of uric acid provided an evolutionary advantage for ancestors of Homo sapiens. This hypothesis was based on in vitro experiments which showed that uric acid is a powerful scavenger of singlet oxygen, peroxyl radicals (RO•2) and hydroxyl radicals (•OH). Urate circulating in elevated concentrations was proposed to be one of the major antioxidants of the plasma that protects cells from oxidative damage, thereby contributing to an increase in life span of our species and decreasing the risk for cancer.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2895915/
So we might have been a bit careless with our enzymes/genes along the way, what? Not just with ascorbic acid.
BUT there is another consideration, one that interests me as a worrier about the natural MEAN values that the body seems to strive for – it doesn’t seem to like extremes. The conclusion of the above study is:
“In conclusion, uric acid is involved in a complex reaction with several oxidants and may have some protective effects under certain conditions. On the other hand, uric acid cannot scavenge all radicals, with superoxide as an example. Uric acid is an antioxidant only in the hydrophilic environment, which is probably a major limitation of the antioxidant function of uric acid. Reactions of uric acid with oxidants may also produce other radicals that might propagate radical chain reaction and oxidative damage to cells. In addition, uric acid itself and/or downstream radicals can engage, as a biologically active proinflammatory factor, intracellular oxidant production via the ubiquitous NADPH oxidase-dependent pathway resulting in redox-dependent intracellular signaling and, in some conditions, oxidative stress. In our opinion, these considerations taken together may explain the oxidant-antioxidant paradox.”
Can’t say I completely understand all this but it is interesting and a bit worrying since the PRO-oxidative effects of vitamin C have also been written about in several other studies. (Easy enough to find on a search for “PRO-oxidative effects of vitamin C “) Difficult to be convinced about anything.
Thank you
Makes Sense that heavy metals play an important part. There are lots of interesting papers and theories on iron too. Chelation works on lots of metals if I understand it correctly, so it may also reduce extra iron and other heavy metals, that’s why they add them back in the formulation. I wonder if Lead and Iron are more attractive or bioavailable together?
Roundup(glyphosate) is also a Chelator, of Magnesium and manganese, that is why constant spraying reduces available minerals and the plants grown on roundup soil are weaker and have less nutrition. Glyphosate is now ubiquitous in the US due to its high usage…maybe this is something related as well. It presents many other problems; Cancer, gut bacteria, hormones, etc. Lots of ways to screw things up.
Unfortunately I can’t make my comments any shorter.
It concerns ‘ADD ONS’.
It was obvious our host Dr K was going to ‘paint himself into a corner’ and not produce magic.
I applaud Malcolm for his efforts with this worthwhile topic….’The operation was a success, but the patient died’.
History:
67 yo M
MI and CABG at age 38
Still smoking from the age of 15….I know!
Support ‘Statins’ for secondary care.
Multiple health problems…any wonder I smoke and drink like a witch.
Current Pathology: bugger the USA..all in mmol/L.
Total chol. = 3.4
HDL = 1.7
LDL = 1.4
Trigs = 0.6
Glucose = 5.5
Homocysteine = 12.6 Oops
APO B = 0.48 g/l
Lp (a) = 0.02 g/l *not current 2013. But can assume excellent (according to the actuaries).
NT-proBNP = 28.8 pmol/L ..shithouse (smoking).
ADD ONS:
This is not advice and has the potential to do you harm. This is only my own ‘Bio-hacking’ N=1.
(1) Nutrition: Micro/macro bits sorted I think and sick to death of any more on this subject.
(2) Supplements: Think I have tried the A-Z of everything. Refined it down to what I consider suitable for me.
(3) Chelation: Originally was an idea to treat ‘Plumbers disease’…you can guess where that one is going. Looked into it 25 years ago. Could not afford ‘professional’ treatment. Got the ‘Protocol’. Then self administered x 8 times IV. Have no opinion with this one. The research is a bit clouded…also chelate’s good minerals. Not convinced either way with this one. There is a theme of a ‘good money making idea’ from the promoters/clinics.
(4) Was ‘slowly’ using 19,000 iu Vit C IV every 2 months. Also B12 injections. Period of 3-4 years. Again, no definitive conclusion.
(5) Hydrogen Peroxide (H2O2) 35% food grade. This is a scary treatment. Self administered 11 treatments of 1% H2O2. I suspect this (no profit) treatment has a useful purpose. Keep in mind that all radical treatments have the potential to shorten your life.
(6) Sodium Theosulphate: Been taking 6 x crystals for the last 20 years. The theory being that it depletes Cyanide, Carbon Monoxide and other bad shit out of your blood. This is an allusive one with no research or references to anything. There is absolutely nothing with this. If anyone knows anything at all…please let me know.
Well, here we go again with intriguing yet debatable evidence.
As long as they put lead in the gasoline – what a silly idea – it was sort of a proxy to low SES, living in concrete hell, not near parks, etc.
Unfortunately, these circumstances independently raise CVD risk and other mortality. Low SES does, living near road traffic does (exhaust, stress, noise), stress does.
Chelation therapy if it works so well we should all chelate. However, including potassium and vitamins sort of makes it harder to figure out whether it was the chelating, or, well, the other good stuff (potassium known to relax blood pressure).
Finally, putting lead in gasoline was a silly idea, but lead and mercury poisoning are not things of the 20th century. Silly people used lead sugar for their wine, lead pipes, lead glass, and basically bathed in mercury, which was a common ingredient in syphilis antidotes, and I seem to recall a compound called kalomel, a laxative, or what was it? Anyway they certainly noticed the symptoms (neurological) but I would not know about CVD specifically.
Sorry about the late response to your comment “.. putting lead in gasoline was a silly idea, but lead and mercury poisoning are not things of the 20th century”. I was very seriously ill and nearly died of mercury poisoning in 1949, right in the middle of the 20th century. It was caused by my GP prescribing a grey teething powder, which contained mercury. A significant number of babies did die before this powder was banned in the UK. The illness was called Pinks Disease by the medical profession.
Dr Kendrick
Your presentation of the TACT trial findings could certainly have been better. Firstly the link you provided took me to a log-in page. Secondly you didn’t point out (or even notice?) that the treatment seems to work only in diabetics (you seem to imply that it works better in diabetics). More information, including the reasons why another trial is needed, can be found here:
http://www.mayoclinic.org/medical-professionals/clinical-updates/cardiovascular/results-trial-assess-chelation-therapy-tact-study-presented
Several important issues are described which highlight alternative explanations for the result seen in diabetics. It therefore makes sense to try to replicate/confirm the diabetes sub-group results in another trial, just of patients with diabetes (no real evidence of benefit in other patients).
An open access paper of the trial (concentrating on diabetics) is here:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4111470/
There’s a vast difference between the numbers Dr Kendrick quoted and the Mayo Clinic figures on the TACT study.
Dr Kendrick quoted: ‘When we broke the composite down to look at our secondary end points, we found that we had about a 40% reduction in total mortality, a 40% reduction in recurrent MI, and about a 50% reduction in mortality [in patients with diabetes],”
Mayo clinic article: The chelated group showed a drop in all-cause mortality (10.4 percent vs. 10.7 percent); a drop in MI (6.2 percent vs. 7.7 percent); a drop in other factors as well.
But: The chelated group started with a lower average LDL which would have resulted by conventional theory in a drop of 3% anyway, close to the 3.5% observed.
And: The biggest effect was seen with diabetics. However, the placebo group of diabetics got glucose infusions, which may have made them worse off compared with the chelated group.
When I saw a write up on TACT six months ago, it quoted the same numbers as Dr Kendrick. I am surprised there’s such a discrepancy with what Mayo quote and I wonder where it comes from.
Can statins increase homocysteine levels ? Springer link 2002 could be of interest.
One statin increases the level of homocysteine and the other one decreases it.
There is a real need to get to the bottom of the different numbers..
Sadly, it seems the HR 8;37 results from an error. The author’s explanation is beyond me, but the “old” abstract in pubmed is not the same as the one at the beginning of the corrected article. This refers to Marc G. Weisskopf et al. in Circulation 2009, 120: 1056-1064, the correction is at http://circ.ahajournals.org/content/130/5/e43.full.pdf
Thanks, will have a look.
I’m just reading A book by David Jay Brown and Garry Gordon MD, definitely worth a read for anyone interested in EDTA chelation. I’m going to start taking ETCA orally tomorrow along with Vit C, Magnesium and a high quality multi vit and mineral. Incidentally, Garry Gordon seems to have disappeared entirely? There is some suspicion that he got ‘shut down’ by the FDA. Of course, we are all just conspiracy theorists!