
7th August 2020
A doctor working in Sweden as an emergency care physician contacted me to discuss all things COVID-19. He has also written a blog, which can be seen here.
I asked if I could reproduce it on my blog as I felt it was a fascinating persepctive on what was happening in Sweden. It is also incredibly well written, in English, for someone who is Swedish. Most humbled. I hope you enjoy it.
Ok, I want to preface this article by stating that it is entirely anecdotal and based on my experience working as a doctor in the emergency room of one of the big hospitals in Stockholm, Sweden, and of living as a citizen in Sweden.
As many people know, Sweden is perhaps the country that has taken the most relaxed attitude of any towards the COVID pandemic. Unlike other countries, Sweden never went in to complete lockdown. Non-essential businesses have remained open, people have continues to go to cafés and restaurants, children have remained in school, and very few people have bothered with face masks in public.
COVID hit Stockholm like a storm in mid-March. One day I was seeing people with appendicitis and kidney stones, the usual things you see in the emergency room. The next day all those patients were gone and the only thing coming in to the hospital was COVID. Practically everyone who was tested had COVID, regardless of what the presenting symptom was. People came in with a nose bleed and they had COVID. They came in with stomach pain and they had COVID.
Then, after a few months, all the COVID patients disappeared. It is now four months since the start of the pandemic, and I haven’t seen a single COVID patient in over a month. When I do test someone because they have a cough or a fever, the test invariably comes back negative.
At the peak three months back, a hundred people were dying a day of COVID in Sweden, a country with a population of ten million. We are now down to around five people dying per day in the whole country, and that number continues to drop. Since people generally die around three weeks after infection, that means virtually no-one is getting infected any more.
If we assume around 0.5 percent of those infected die (which I think is very generous, more on that later), then that means that three weeks back 1,000 people were getting infected per day in the whole country, which works out to a daily risk per person of getting infected of 1 in 10,000, which is miniscule. And remember, the risk of dying is at the very most 1 in 200 if you actually do get infected. And that was three weeks ago. Basically,COVID is in all practical senses over and done with in Sweden.
After four months. In total COVID has killed under 6,000 people in a country of ten million. A country with an annual death rate of around 100,000 people. Considering that 70% of those who have died of COVID are over 80 years old, quite a few of those 6,000 would have died this year anyway. That makes covid a mere blip in terms of its effect on mortality.
That is why it is nonsensical to compare covid to other major pandemics, like the 1918 pandemic that killed tens of millions of people. COVID will never even come close to those numbers. And yet many countries have shut down their entire economies, stopped children going to school, and made large portions of their population unemployed in order to deal with this disease.
The media have been proclaiming that only a small percentage of the population have antibodies, and therefore it is impossible that herd immunity has developed. Well, if herd immunity hasn’t developed, where are all the sick people? Why has the rate of infection dropped so precipitously? Considering that most people in Sweden are leading their lives normally now, not socially distancing, not wearing masks, there should still be high rates of infection.
The reason we test for antibodies is because it is easy and cheap. Antibodies are in fact not the body’s main defence against virus infections. T-cells are. But T-cells are harder to measure than antibodies, so we don’t really do it clinically. It is quite possible to have T-cells that are specific for covid and thereby make you immune to the disease, without having any antibodies.
Personally, I think this is what has happened. Everybody who works in the emergency room where I work has had the antibody test. Very few actually have antibodies. This is in spite of being exposed to huge numbers of infected people, including at the beginning of the pandemic, before we realized how widespread COVID was, when no-one was wearing protective equipment.
I am not denying that COVID is awful for the people who do get really sick or for the families of the people who die, just as it is awful for the families of people who die of cancer, or influenza, or an opioid overdose. But the size of the response in most of the world (not including Sweden) has been totally disproportionate to the size of the threat.
Sweden ripped the metaphorical band-aid off quickly and got the epidemic over and done with in a short amount of time, while the rest of the world has chosen to try to peel the band-aid off slowly. At present that means Sweden has one of the highest total death rates in the world. But COVID is over in Sweden. People have gone back to their normal lives and barely anyone is getting infected any more.
I am willing to bet that the countries that have shut down completely will see rates spike when they open up. If that is the case, then there won’t have been any point in shutting down in the first place, because all those countries are going to end up with the same number of dead at the end of the day anyway. Shutting down completely in order to decrease the total number of deaths only makes sense if you are willing to stay shut down until a vaccine is available. That could take years. No country is willing to wait that long.
COVID has at present killed less than 6000 in Sweden. It is very unlikely that the number of dead will go above 7,000. An average influenza year in Sweden, 700 people die of influenza. Does that mean COVID is ten times worse than influenza? No, because influenza has been around for centuries while COVID is completely new.
In an average influenza year most people already have some level of immunity because they’ve been infected with a similar strain previously, or because they’re vaccinated. So it is quite possible, in fact likely, that the case fatality rate for COVID is the same as for influenza, or only slightly higher, and the entire difference we have seen is due to the complete lack of any immunity in the population at the start of this pandemic.
This conclusion makes sense of the Swedish fatality numbers – if we’ve reached a point where there is hardly any active infection going on any more in Sweden, in spite of the fact that there is barely any social distancing happening, then that means at least 50% of the population has been infected already and have developed immunity, which is five million people.
This number is perfectly reasonable if we assume a reproductive number for the virus of two: If each person infects two new, with a five day period between being infected and infecting others, and you start out with just one infected person in the country, then you will reach a point where several million are infected in just four months. If only 6000 are dead out of five million infected, that works out to a case fatality rate of 0.12 percent, roughly the same as regular old influenza, which no-one is the least bit frightened of, and which we don’t shut down our societies for.

Very interesting, but who is the doctor?
Here’s the link https://sebastianrushworth.com/2020/08/04/how-bad-is-covid-really-a-swedish-doctors-perspective/
It was at the end of Dr. Kendrick’s opening paragraph
Sebastian Rushworth, M.D.
A link to his original blog post is noted in the first paragraph of the article.
Sheila Dillon: Click the link “here” at the top of this post, and it will take you right to Dr. Rushworth’s blog. I, and I suspect many others here, have subscribed. Much good information there.
I just wish that our government had the good sense of the Swedes
Thank for for sharing this Malcolm.
While what he says seems very reasonable in a Swedish situation, I’m just not sure how much it also applies in very different contexts … maybe we need to see how the numbers change over a full year, and look (as you do) at excess mortality.
My friends are often taken aback when I point out that the worst-case UK “Covid death” numbers are still significantly less than the annual deaths from smoking-related diseases.
It would be interesting to know how that perspective works with Brazil etc…
This guy’s other stuff is very interesting too.
I love his take on “Do statins save lives?”
Hi second conclusion is a great way of restating the issue:
“What this means is that it is pointless to get your cholesterol levels tested – the number you get back doesn’t tell you anything about your probility of benefiting from taking a statin.”
What’s Covid death numbers got to do with deaths from so called smoking related diseases. Those aren’t actual deaths, but statistical mumbo-jumbo used for ideological, political and financial reasons.
Do you think that the UK’s initial response was to try and achieve herd immunity like the Swedes seem to have done? But due to public pressure (and the approaches taken around the world) they caved in? I know that Sweden also had a problem with care homes which seemed to be the case almost everywhere else on the planet – that seems to me a bit coincidental given that the age demographic in China and Italy indicated that they were the most vulnerable!
It wasn’t public pressure, it was the scaremongering of a certain discredited epidemiologist that persuaded the Government that, unless they locked the country down – clearing out sick elderly in-patients from hospitals to care homes to make ward space to take all the Covid patients – then the NHS would be ‘overwhelmed’. Hence the slogan, “stay at home, protect the NHS, save lives”.
But I think it was public and press pressure as well, Steve. And that was quickly ratcheted up. In fact, I think very quickly the government was preoccupied with what they were thinking. I think today it’s the press and public leading the way and an inept government following.
I predict that some time in future an ex minister or someone close to decision making will come out and say “We knew but we were in so deep and didn’t know how to get out of the mess.”
Most likely they were offered a bribe by the World Bank.
Don’t forget also the wide spread stream of donations of the Bill & Melinda Gates Foundation to various Universities and News Media in the UK.
Might not be the nicest president in the world. This from a human rights group on Belarus;
“Civil society activists, lawyers, rights groups, and independent media face government harassment and pressure. Authorities have arbitrarily prosecuted dozens of journalists on a variety of grounds and in June 2018 the government adopted further restrictions on internet freedoms.
Belarus is the only European country to use the death penalty”
The lady who went for office is now in Lithuania while her husband is in jail for flimsy enuff reasons. Even the Poles are not happy with the election where the sitting Pres got 80% of the vote. Mmmm.
I think there is a strong chance you are right. Hectoring by the broadcast media at the daily governmental briefings soon put an end to that. “Herd immunity, Prime Minister – are we no better than animals?”
beejay68, the “public” don’t do public pressure, it is the MSM as instruments of corrupt or ignorant politicians who do the pressure, and claim it is from the “public”.
I think some leaders of countries are deliberately kept in the dark regarding big issues so they have plausible deniability. Boris’s immediate response was from his own common sense (yes he plays the bumbling likeable politician but he’s not stupid) and trusted colleagues, in going the Swedish route for quick herd immunity. He was obviously told to do otherwise by the ptb. Hence the shambles we have to live through and the planned destruction of the UK economy and most of the western world.
What happened was Neil Ferguson produced his cataclysmic estimates of 500,000 people dieing in the Uk. That scared the government into lockdown. He also estimated 30,000 deaths in Sweden if they didn’t lockdown. He has a lot to answer for.
Not this again,
Sweden took a snapshot of the Imperial College code and used their modified version to decide on their policy. Prof. Ferguson had nothing to do with Sweden’s policy.
The 500,000 death number was predicted if the U.K. did nothing, perhaps 500,000 was too high, we’ll never know, but the U.K. decided not to take the risk.
The mortality rate seems about right, even accounting for age, but the infection rate seems way off. Could this be social distancing? Could this be the virus isn’t very infectious. Interesting questions.
Ferguson has been wrong about everything he predicted and the code they used sucked, so why would this prediction be any different? I very much doubt that the measure have done anything except kill the elderly and destroy the economy. If they worked, there’d be no flu either and there is: see the chart Flu deaths vs Covid deaths in https://thehumanunleashed.com/covid-the-case-against-the-uk-government/ “You can see that, following a tremendous spike in death rates, since mid-June deaths linked to COVID have been significantly lower than flu/pneumonia deaths.” If any of the measures were logical, I’d probably have accepted them, but they are not.
Are you familiar with Graham’s hierarchy of disagreement? Your reply ranks down at the bottom of this pyramid and is little better than name calling.
“Ferguson has been wrong about everything he predicted and the code they used sucked, so why would this prediction be any different?”
Can you be more specific in how the code “sucked”. Any files, functions, coding style , naming conventions, you can point me at? I’ve looked at the code and there is a huge omission but I wonder if you’ll see it too.
So I guess when you say he’s been wrong in the past you’re referring to the Foot and Mouth outbreak in 2001. A professor from Edinburgh disagrees with Dr Ferguson’s analysis but perhaps this is just academic sour grapes. Dr Ferguson got the Foot and Mouth gig but the Edinburgh chap didn’t. The culling programme seemed to work. Culling was used in 1967 too so perhaps this was the right thing to do. Other countries adopted the same strategy and Prof Ferguson had nothing to do with that. We still cull entire herds when TB is found.
Ferguson was also good at swine flu predictions and BSE predictions.
I’m sure you are capable of finding the code on Github and the expose on the Web. Of course, the report is under a fake name (Sue Denim). The best bit is ” Non-deterministic outputs. Due to bugs, the code can produce very different results given identical inputs. They routinely act as if this is unimportant …This problem makes the code unusable for scientific purposes, given that a key part of the scientific method is the ability to replicate results. Without replication, the findings might not be real at all – as the field of psychology has been finding out to its cost. Even if their original code was released, it’s apparent that the same numbers as in Report 9 might not come out of it.”
Not just foot and mouth, also BSE and swine flu.
So you can’t point at anything specifically wrong with the code although there’s plenty of choice. I have pulled the code from Github and looked at it, built it, and run it, but I was interested in your direct observations.
I’ve read this thing about the model producing different results on every run but this is how these models work. They are run many, many times with slight perturbations and you hope that some pattern emerges. In the case of the Imperial College model, they use the current time to seed the random number functions so you would observe different results every time. This is how weather forecasting works by the way.
I asked about Foot and Mouth but you changed the subject to BSE & Swine Flu.
I have no idea if there is anything wrong with the code – at all. I wouldn’t understand the coding anyway. However, that is not really relevant. The important issue is, what are the assumptions? I have just been reading a report Technical Group Report: Model fitness-for-Purpose Assessment report on the COVID modelling that has been done so far.
Key partners of the report include: NORAD, WHO, CDC etc.
The key conclusions are:
The majority of the models are mechanistic, incorporate age-distribution in transmission and mortality parameters, and base the IFRs on strong assumptions from data collected early in the pandemic. At the
same time, most models do not account for particular sub-populations or comorbidities, do not include indirect COVID-19 effects on other diseases and do not model economic outcomes. There were also differences across the models, such as in their purposes and aims, in how COVID-19 transmission and contact patterns have been implemented, in the breadth of interventions considered, and in how these interventions were constructed.
You may see a few flaws, or important omissions, in there.
Anyway, the Imperial Model was very simple. Everyone is equally likely to become infected (assumption). Unless various steps are taken, 80% of the population will become infected (assumption). The Infection Fatality Rate will be 0.9% (Assumption).
66 million people x 0.9% x 80% = ~500,000 dead = lockdown
Lets try an IFR of 0.1% and see what happens.
“It is also incredibly well written, in English, for someone who is Swedish.”
He doesn’t say that he was born Swedish or grew up and/or was educated in Sweden. Given his name, I would suspect an Anglo origin, but I haven’t found his educational CV to confirm or deny.
Sweden is the 2nd best country in the world in English as a second language: https://ceoworld.biz/2019/11/05/revealed-the-worlds-best-non-native-english-speaking-countries-2019/
I live in Sweden and I can tell you everybody with an academic degree has that level or a similar level of English. Give us non-natives some cred, will ya? 😉
I think this was just Malcolm’s polite way of saying, “The English isn’t perfect, but ignore that.”
I think it was quite perfect (I’m not a Swede).
I have noticed that most non-English speakers write significantly better English than us locals do! I guess that people who actually learn our grammar are less likely to make mistakes than us locals who just absorb it!
I have visited Sweden 3 times and I am very impressed that I can go anywhere and speak English and the responses I get back lack any hesitation.
Thank you
I do wonder if that happened to me, that I have the right T-cells. I wish there was a way to test it somehow, cheap and widely available.
I work in healthcare, and had frequesnt contact with covid patients – not as intense though as health professionals on covid wards or A&E. Three of my colleagues I worked closely with in March and April tested positive, and were off with covid for a few weeks – I got away. When I say closely – it is not possible to keep 2 metres away in a hospital setting if you work together approaching patients and collecting samples. When antibody testing started, not many of A&E staff in my hospital tested positive, and those who did had been covid positive before (that is just anecdotal, following many conversations with various nurses and support workers, no idea if official numbers exist or are available, I would like to see thos, they might show a completely different picture).
My husband is a psychiatrist. Hasn’t missed a day of work, nor any of his colleagues. Had a few patients transferred to med/surg facilities. No State or Federal health official followed up with any staff etc.
Have you ever tried to convince a demented, psychotic or Meth redrawing individual to wear a mask and stay far away?
Has anyone noticed the lack of massive infections reports at any psych hospital in the WORLD?
Interesting point….
Holly, nothing to do with Psych. patients being younger and in perhaps better (metabolic) health than those frail and unwell inhabitants of ‘God’s Waiting Rooms….’
Also, it appears that non-permanent staff are a feature of Aged Care / Nursing homes – even public hospitals – the world over. That alone would account for the residents being exposed to a wider spread of the “outside” population and therefore chances of being infected.
The Devil is always in the ‘Details’ !
dear Agg,
the tests are all a scam, they do not test for anything related to any virus. If you don’t believe me, just read the limitations of the test of the manufacturer, that is where they tell the truth, namely that is it completely useless and unvalidated.
even the who cdc and ecdc don’t lie about this, they ALL openly state the tests are not validated.
not valid, means not valid, it means that NOBODY on this complete by insanity infected earth actually has proof wether or not ANYBODY is infected, nobody is confirmed, nothing, zero, etc.
it is a total disgrace
Bravo!
Thank you
Thanks to the Swedish doctor for the article & to you for reproducing it.
Why isn’t this featuring on the BBC news?
Censorship in a democracy is a serious concern.
“Censorship in a democracy is a serious concern”.
Sounds like a theoretical possibility.
But in the real world – do you know of any democracies? Any single one?
Why not ? Because it does NOT fit the mandated narrative.
BBC and news? The ultimate oxymoron.
Do you mean the Biased B B C
What a great piece to share. Well done, Sweden!
Each T cell will develop its own T cell receptor (TCR) that is specific for a particular antigen. T cells that survive thymic selection will mature and leave the thymus. They will circulate through the peripheral lymphoid organs, each ready to encounter a specific antigen and be activated. Once activated, the T cell will proliferate and differentiate into an effector T cell.
The thymus involutes as we age and so produces fewer naïve T cells over time. Does therapy to encourage thymic output by slowing down oxidation have a part to play in treating those at risk of C-19?
Does oxidation actually slow down thymic output? Does oxidation increase in the elderly? Citations?
This was interesting so I looked it up. There’s lots of studies on the thymus. One found that you could make your thymus healthier (or younger) by increasing human growth factor, increasing insulin sensitivity and taking DHEA. The ways that I know about to do that are fasting and HIIT training. They don’t need to be done at the same time.
https://www.medicalnewstoday.com/articles/326329
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5869099/
Thanks for being curious, Kara.
Yes, fasting has a part to play in slowing down ageing, as does reducing calories to 1/3rd normal daily intake.
You’ll know that obesity is a major risk factor in controlling C-19 and all other viral antigens.
Dr Kendrick
Thanks once again. Wish I was Swedish.
Many people will be interested and reassured by this sensible analysis from Dr Rushworth.
Some of the people who won’t generally be interested in this article are –
* Journalists – it’s not a headline grabber and besides it shows all of the press Covid hysteria to have been irresponsible. So you will never see this article in the mainstream press. * Politicians – who are too busy continuing to dig in the big hole they’ve made. They think they’re burying the evidence and maybe they’re right. Besides Covid Hysteria is a great opportunity to dictate to people – that’s why they go into politics. * Very large numbers of people who just prefer to catastrophise in general – Covid has been a marvellous opportunity for them, the like of which I hope they never see again. They prefer to never let the facts get in the way of a good wail.
This is a powerful combination. I’m passing this article on to as many people with two brain cells to rub together as I can find.
Best regards
Dr Patrick Nerney ________________________________
The only respectable case I could see for a lockdown was that something might turn up – the virus would mutate to become less deadly, treatment would improve dramatically, or – least likely – a vaccine would be developed swiftly. With hindsight the only one of those hopes to bear any fruit is the treatment one – particularly learning not to kill patients with ventilators.
There was also the “save the NHS” argument, but that rapidly proved ill-judged as staff waited around in hospitals with nothing to do while their colleagues discharged infectious patients into care homes.
It’s all been a bloody disgrace really: an outbreak of hysteria worthy of a place in the history books. People started off underestimating the problem – a sniffle from China that probably wouldn’t reach us – and then leapt to wild overestimation of it. No doubt some of the economic damage would have happened lockdown or no. Frightened people cowering at home don’t make for prosperity.
Still, however badly the media, the NHS, PHE, and the government have behaved I must say that a special place in hell should be reserved for the schoolteachers’ unions. They’d be nane the waur o’ a hingin’.
I think that if teachers are too scared to teach and aren’t intelligent enough to analyse the stats, perhaps they shouldn’t be teachers at all. Or to be fairer, let them stay at home without pay once they’ve used up their holiday allowance. A relative of mine who is a qualified teacher working as a care assistant as no teaching jobs would love to get back to teaching. I’m sure she’s not the only one.
I hate to disagree but the only scientific basis for a lockdown a.k.a. Mass quarantine is to prevent the spread of a pathogen that presents an existential threat to our species (or for example to any species upon which our existence depends) – in this case it was obvious long before we acted that such a threat did not exist.
Which is not to say that it won’t exist in the future and that it is probably prudent to act on the basis that it might and we should prepare plans accordingly, because if it does happen it will not be pretty.
Quarantine is for the sick not the healthy.
Existential threat to our species is very clearly – our own kind – and our own ‘thinking’ or rather fear-framed beliefs operating a self-reinforcing script.
The scientific basis for choking back the global economy while imposing forms of martial law under medical pretexts is the science of genetic selection and applied psychology.
That final suggestion might be going a bit too far.
But I agree with your take on the EIS and their shameful position in all this melee.
My last comment was in response to dearieme from August 7, 2020 at 11:50 am
The comment made was ‘They’d be nane the waur o’ a hingin’ refers to martial law to those who have no Scots dictionary handy.
Tsk tsk Dearieme, “… They’d be nane the waur o’ a hingin’…. – Don’t limit it to Teachers!
Politicians should queue at the scaffold…. Right behind “journalists”., you know, the creatures mentioned by Dr Nerney, too lazy to dig out Truth.. Yet another previously important part of Society who’ve abrogated Responsibility.
Thank you for sharing this excellent concise coherent synopsis of a Swedish doctors experience. If only more people working in medicine felt less frightened about sharing their views. The amount of censorship around this has been truly disturbing. I have several friends who work in the NHS and Social Care sector who tell me a similar story. A sensationalist media has driven Government policy to the detriment of public health. No country ever improved its healthcare system by making itself poorer.
More power to your elbow Dr. Kendrick.
Received this link today from a Russian connection. A Lady in India has researched the covid ‘plandemic’. Whilst her credentials are unknown, she makes a lot of sense to the whole global situation:
Derek Reynolds. Retired layman with an inquiring mind.
There’s a fine line between genius and madness
Ok until she moved over to electric magnetic radiation weaponry – should have left it at that.
It doesn’t change the facts about the live exercise that should have started in September 2019.
There are also other sources that confirm this.
There’s also a biological theory that can explain the influence of HF EM radiation on human cells’ sodium pumps. It has to do with field strength amplification (200-2,000 x) in regions with different electrical dielectric strengths, like the cell wall in its watery environment.
Further, her English is perfect so she can’t be crazy. 😉
The International Health Regulations 2005 that she treats basically states that you’re not allowed to travel if you’re not vaccinated. States are committed to submit legislation to ‘permit submission to these regulations’.
So, this covid exercise may be a coronavirus that is part of the regular flu repertorium. What I read today on the BBC website is what she mentions also: a case of buebonic plague has been diagnosed in China. Now THIS could be the ‘deliberately released pathogen’ from the second exercise. Bill Gates in interviews has also hinted at a ‘second epidemic’ ‘that WILL get attention’.
Surprisingly Sweden is one of the countries that signed off on this.
Actually I haven’t heard her talking about EM radiation weaponry…
HDB – She comes across as very rational. But we are just getting to grips with what she has said which is confounding, incredible and terrifying – then she moves on to something completely different which seemed to morph in to other horrors – Hydra like. At that stage with maybe an hour to go, I needed to get out and clear my head so did a 30 minute climb to come across some wild campers beside a mountain top lake – far from the madding crowd !
Slightly batty….giving her the benefit of the doubt.
Derek Reynolds – thank you for posting this link.
Probably most of the answers to the questions that many are asking ‘what the hell is going on?” are here!
The technique of hiding information in plane site is being well used.
I hope people take the time to watch the video ( I’m only 18 mins in) and ask the question ‘Is this what the world needs?’ ‘Is this the only way to achieve it?’
I fear people we may never have heard of or given permission to have already made that decision for us. I hope the sacrifices that have been and will be made are necessary.
Well!
So this virus is working it’s way through communities – why is there a ‘race for coronavirus vaccines’ led by Bill Gates? So much money and resources are going into this race for a virus that may be fading – this would be better spent on developing effective preventatives and treatments for the afflicted now.
And given the virus has most impact on the elderly, why is Gates saying the entire global population has to be vaccinated – and why is software billionaire Bill Gates leading on international public health?!?!
Now they’re admitting the vaccines are unlikely to be effective in the elderly, and the suggestion is to vaccinate children to protect the elderly – this is wrong. Children aren’t generally at risk with this virus, why should they be vaccinated and have their own natural defences disrupted?
It seems the goal is to hook the entire global population on annual coronavirus vaccination, and dramatically boost already burgeoning vaccine markets.
See my recent rapid response on this matter on The BMJ: Is it ethical to vaccinate children to protect the elderly? https://www.bmj.com/content/364/bmj.l108/rr-4
Great marketing strategy. Will they get a best in category award?
Just like we had a ‘anti-terror security state’ we will now have a ‘bio-security state’. Patrick Zylberman wrote about this in his 2013 book ‘Tempêtes microbiennes’, a review (in English) of which you can read here: https://booksandideas.net/Imagining-Health-Disasters.html
Thank you for this
The world of the MSM fantasy seems to be at odds with reality
This is very interesting. Thank you for posting the article. If we had better treatment for covid and after effects there would not be much of a problem.
As far as I can see there is a non-pharmaceutical option, hyperbaric oxygen treatment. But then I’m a fan.
Both China and USA tried it on a few patients instead of intubation, they all came quickly out of distress. A somewhat larger study should be completed but can’t find anything published.
I found a discussion in an online engineering publication on converting aircraft which are hyperbaric chambers, an online diving magazine begging that a study be allowed as they knew where to find the large chamber which hospitals in London used in the past.
Blood and tissues become very high in oxygen, viruses cannot survive that.
For people who have suffered long covid it’s healing on steroids.
If I knew I could go in a chamber I would not worry about catching it in spite of my age and poor state of health.
A good idea but I doubt if there are enough facilities to do it on a large scale, especially in third world countries.
On the other hand there are the various HCQ based prophylactic treatments and MATH+ for more advanced cases.
No chance Steve, and for the same reason the ‘(Dr Paul) Marik Protocol is studiously avoided… both incorporate Ascorbic Acid / Vitamin C, the Great Satan in the eyes of Mainstream Pharmaceutical-driven medicine.
Oh, and because they both are effective at fraction of the cost.
India just replaced the hcq the much less controversial yet very effective ivermectin.
https://indianexpress.com/article/india/up-new-protocol-ivermectin-to-replace-hcq-in-treatment-of-covid-patients-6545236/
I also bought a load of ivermectin, over the counter, in the pet shop…
What a co-incidence ! I happen to know where you will find many, MANY never-to-be used-again airliners, some not all that old and could still be flown to where they’d be utilised.
Indeed, the smaller ones still parked at local airports – owned by recently bankrupt airlines – could quickly be re-purposed for hyperbaric sessions.
https://airplaneboneyards.com/airplane-boneyards-list-and-map.htm
Agate Karevoll: Hyperbaric oxygen treatment is indeed a very useful therapy for a variety of conditions. Alas, it is not easily accessed here in the U.S., except for wound healing (after amputation) in diabetics. Not enough money for the Big Boys in it. My own doctor refused to consider referring me for cancer therapy. Happily, I seem to be cancer free. Time to find a new doctor, except the face-diaper mandate seems nearly universal now here in California. And I have no need of a doctor! I feel great!
I think masks are a filthy habit. One of my local hospitals has forced its employees to double mask. Two of the four staff I spoke with admitted they are getting headaches. They wear a face shield as well. This in a state with very low case numbers. I think this hospital could be vulnerable to lawsuits because I am pretty sure that there are no studies on double masking and therefore they are playing with their employees’ health with no data.
anna m, you may well be right. This is not from a journalist or politician, but from a hospital https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2493952/pdf/annrcse01509-0009.pdf. They wondered how much benefit masks worn in operating theatres might give. The answer appears to be not a lot. Those who vehemently claim masks reduce transmission might like to find a suitably comparative study to demonstrate their point.
This from Arthur Firstenberg:
As a person who went to medical school, I was shocked when I read Neil Orr’s study, (see link above) published in 1981 in the Annals of the Royal College of Surgeons of England. Dr. Orr was a surgeon in the Severalls Surgical Unit in Colchester. And for six months, from March through August 1980, the surgeons and staff in that unit decided to see what would happen if they did not wear masks during surgeries. They wore no masks for six months, and compared the rate of surgical wound infections from March through August 1980 with the rate of wound infections from March through August of the previous four years. And they discovered, to their amazement, that when nobody wore masks during surgeries, the rate of wound infections was less than half what it was when everyone wore masks. Their conclusion: “It would appear that minimum contamination can best be achieved by not wearing a mask at all” and that wearing a mask during surgery “is a standard procedure that could be abandoned.”
I was so amazed that I scoured the medical literature, sure that this was a fluke and that newer studies must show the utility of masks in preventing the spread of disease. But to my surprise the medical literature for the past forty-five years has been consistent: masks are useless in preventing the spread of disease and, if anything, are unsanitary objects that themselves spread bacteria and viruses.
Ritter et al.,https://app.cyberimpact.com/click-tracking?ct=zYPbknbzndPrP_GvheTWrorlvYiPtU2KN7–C9aE5cC9chlYiczC9ZiHgHqIh3HWylgG61L9yEix0D-poRkprWfy_PnbeUVwRB1dEoT0zzk~ in 1975, found that “the wearing of a surgical face mask had no effect upon the overall operating room environmental contamination.”
Ha’eri and Wiley, https://app.cyberimpact.com/click-tracking?ct=mML94gukm1apjaWVTbaN_p2e9dxUWCXTS_b2rCRC7_LVpbcOj_4X4-QS9ZEXxyOoWBQBR9bceDxLkdr3G_q_PZl_XhoE7g1cZEjsOlFAVlw~ in 1980, applied human albumin microspheres to the interior of surgical masks in 20 operations. At the end of each operation, wound washings were examined under the microscope. “Particle contamination of the wound was demonstrated in all experiments.”
Laslett and Sabin, https://app.cyberimpact.com/click-tracking?ct=p7BMpg8nmzHyuzycxYrkERt6fGH1fCbL30MoofaW7NU5kW9tb2t9rn12bcXMM-pIuB0oasZ0zwdX5lyYvQR8unHMgANMPGWGww_Ri1WfMuI~ in 1989, found that caps and masks were not necessary during cardiac catheterization. “No infections were found in any patient, regardless of whether a cap or mask was used,” they wrote. Sjøl and Kelbaek https://app.cyberimpact.com/click-tracking?ct=bH21cUPHe2_9bOukCPHEZ6gfFG56cLSEywcqMrUOF50t62BiqSQaqTKfHcihlhlA29NpdDVBCVnFh_F8vlVbwBEJEhYu4RLsb2cIzp4D9Kw~ came to the same conclusion in 2002.
In Tunevall’s 1991 study https://app.cyberimpact.com/click-tracking?ct=XgEDhZ-VJePhbG66BU_x6rNhtsoLkEIku-wqjX5QLi9gU_oV3f76KlLUZV71In_LeIKc2VAQOMuDnh-MqnoZJASCz3aquSxosy89bh1bUEU~, a general surgical team wore no masks in half of their surgeries for two years. After 1,537 operations performed with masks, the wound infection rate was 4.7%, while after 1,551 operations performed without masks, the wound infection rate was only 3.5%.
A review by Skinner and Sutton https://app.cyberimpact.com/click-tracking?ct=l-8TKFLSOSl8s4vDh_Wj-axPBKDb1t4CrhVq3wiZ-it1AsXBXuulb7VuliAu4V3krfgnX2DoSEkJuZVgX3zMnvLmBboZLQ9GnD6jyvdXtlw~ in 2001 concluded that “The evidence for discontinuing the use of surgical face masks would appear to be stronger than the evidence available to support their continued use.”
Lahme et al https://app.cyberimpact.com/click-tracking?ct=Bz-XF_1OtIUpqAJUKsCjB7mVRhD1dOGsddQTi92jxpiKXIgWsn8iXE1JJ6wQru5i6IE5l4qocPIGg66qCAlSa6NbQml8ix0lU-3bz3mqMuw~., in 2001, wrote that “surgical face masks worn by patients during regional anaesthesia, did not reduce the concentration of airborne bacteria over the operation field in our study. Thus they are dispensable.”
Figueiredo et al.,https://app.cyberimpact.com/click-tracking?ct=mTDHuRIwpjF_lwzCSbTl9_Heweog2YxSIdT7N1L0tM2VXeDwGVzcaQPzfzLi_yrwSqEom9hlY1Zdk5z8xX2AAiboCksCJU-GwfJFAnqy89E~ in 2001, reported that in five years of doing peritoneal dialysis without masks, rates of peritonitis in their unit were no different than rates in hospitals where masks were worn.
Bahli https://app.cyberimpact.com/click-tracking?ct=Dh_lNWhekvyhZhu-T7yFYQmr-_l0QXlwMLoe96kfOkeFdQp1Kp4-Zn75LFDFUnngyJgmpZyuw-3fgJa7XwPa0D1m90R9ZKqyS4p2jQUJQe8~ did a systematic literature review in 2009 and found that “no significant difference in the incidence of postoperative wound infection was observed between masks groups and groups operated with no masks.”
Surgeons at the Karolinska Institute in Sweden, https://app.cyberimpact.com/click-tracking?ct=PfxQOMygMiYz2tnDEeXA8UFIudGGzrw0HQLeQgOa-zxwPlIIoNR92UGibOhDgD9D-6JCEhBAPTHUxj72uMQHCjddpbcCtqmJjvRCGrdTGDk~ recognizing the lack of evidence supporting the use of masks, ceased requiring them in 2010 for anesthesiologists and other non-scrubbed personnel in the operating room. “Our decision to no longer require routine surgical masks for personnel not scrubbed for surgery is a departure from common practice. But the evidence to support this practice does not exist,” wrote Dr. Eva Sellden.
Webster et al., https://app.cyberimpact.com/click-tracking?ct=cvKpEoXrBDbrEmCaZM_va0BsAOFDoy337rq2lgc-EWcZ2Y3Ao92etryazJesBjikA7lvtPtgqU2P_1F6C1HIFeYHwEj9uKck_5AEYncyGUM~ in 2010, reported on obstetric, gynecological, general, orthopaedic, breast and urological surgeries performed on 827 patients. All non-scrubbed staff wore masks in half the surgeries, and none of the non-scrubbed staff wore masks in half the surgeries. Surgical site infections occurred in 11.5% of the Mask group, and in only 9.0% of the No Mask group.
Lipp and Edwards https://app.cyberimpact.com/click-tracking?ct=WRIXiwuR_jrqhsHC3tmMcQsQ3lDmCQfxqud0TaaDXJCZZPOBVPkoOpGYoPxqpHZ3NQO_VuEEktEYnwi72UDADGuHXCoiKel0AsnJErgRZVA~reviewed the surgical literature in 2014 and found “no statistically significant difference in infection rates between the masked and unmasked group in any of the trials.” Vincent and Edwards https://app.cyberimpact.com/click-tracking?ct=OHQGujFy2XUyF1PsMPfMxgdPGMqzxeqjUtwa035xQyTSy_UuMneJLV9VyuuXRP6DC6B6djl5ZgsCtBpwPB0spXNF6k9TV54F2Hh7KQSMxyM~ updated this review in 2016 and the conclusion was the same.
Carøe https://app.cyberimpact.com/click-tracking?ct=XUK3i1aO0K63CaxmSZIZjfUVSetVC1Y61lcTGtcKP5c2UvVIucesnBt9tv7WJNJvGqvF8SmZlIh1XbB38KX1WW8Iuhsp9v04erYvYpgx_po~ in a 2014 review based on four studies and 6,006 patients, wrote that “none of the four studies found a difference in the number of post-operative infections whether you used a surgical mask or not.”
Salassa and Swiontkowski, https://app.cyberimpact.com/click-tracking?ct=TltpBc_3PRvwjtOI83n7RMPur7ezO7S917_8tLC-25fjg8Z9tGvRqXU6z8nThiB_jEq9i_uKFDFKE3L-cbm_9zqlE2uhsbO29A6i8lgef9w~ in 2014, investigated the necessity of scrubs, masks and head coverings in the operating room and concluded that “there is no evidence that these measures reduce the prevalence of surgical site infection.”
Da Zhou et al., https://app.cyberimpact.com/click-tracking?ct=KDFAGEfWxl_AIG2The9U06KB_yQgqF3ZKa3qknMTFiSuljheELsuwZXWoejOTq_XbVUTLgFeBM5XCBMFL37BSZ0w0Cnct31nPxON-2k0XaY~ reviewing the literature in 2015, concluded that “there is a lack of substantial evidence to support claims that facemasks protect either patient or surgeon from infectious contamination.”
Schools in China are now prohibiting students from wearing masks while exercising https://app.cyberimpact.com/click-tracking?ct=utx-MQ_PX-m_skrbpAVcLXTFBu2QezLcGM44LlEdXShO02tPnRn-I674Yx7wS-gaygMrAD-gKJNqdOlJI9yjQmciaoDO-Hqco6rdOl63Wqw~. Why? Because it was killing them. It was depriving them of oxygen and it was killing them. At least three children died during Physical Education classes — two of them while running on their school’s track while wearing a mask. And a 26-year-old man suffered a collapsed lung after running two and a half miles while wearing a mask. https://app.cyberimpact.com/click-tracking?ct=IJxEFBHcWAvzULdOsSyE83oUS9kVbUsoP0GsCdj5XzEbZaYyz0QU5a5vi2OjwoDK_zSFVY6z8DsVgZBBavPXlCO4HgkexBJ4gURkp_nRm4A~
Mandating masks has not kept death rates down anywhere. The 20 U.S. states that have never ordered people to wear face masks indoors and out have dramatically lower COVID-19 death rates than the 30 states that have mandated masks. Most of the no-mask states have COVID-19 death rates below 20 per 100,000 population, and none have a death rate higher than 55. All 13 states that have death rates higher 55 are states that have required the wearing of masks in all public places. It has not protected them.
“We are living in an atmosphere of permanent illness, of meaningless separation,” writes Benjamin Cherry in the Summer 2020 issue of New View magazine. A separation that is destroying lives, souls, and nature.
_____________
* from Christopher Fry, A Sleep of Prisoners, 1951.
Arthur Firstenberg
August 11, 2020
A very interesting post, and certainly well referecned.
Dr Kendrick,
That sounds like “faint praise” to me. I wouldn’t have expected anything more definitive from you, at this point, but I don’t think it’s helpful to make such equivocal statements in the meantime.
Since everyone reads everything you write to gleam meaning from it . . . what do you mean??
Operating theatres, which the studies you reference apply to, are well ventilated with filtered air, one may assume. But sit in a crowded minibus taxi with all the windows closed against the winter wind (although by law they are required to be open), like I have numerous times this past week, and you feel glad that you are wearing a mask, and that everyone else is also wearing a mask.
Also, what about fomites on surfaces? Some of them are from infected droplets. In an operating theatre which is cleaned to sterile conditions they will get removed, but in far less sanitary public places they build up. Masks stop some of the droplets containing the virus, and reduce the viral load somewhat.
As I’ve said before, masks don’t make a big difference to an individual, but a small difference to an exponential-type growth rate makes a big difference to the final numbers of infected and dead in a population.
Hi Gary, Here in England it’s charities who run many of the hyperbaric oxygen chambers. They are not expensive but are healing on steroids. Strokes, bran damage, cancers, joints, wounds, burns any poor healing inflammation yes viruses. The body sets about growing more blood vessels and stem cells. Autistic children arrive with scowls and leave with grins from ear to ear.
You are right, no money for the big boys but my could a lot of money be saved.
Altering aircraft would be easy and at present there are very many aircraft engineers looking for work, also spare aircraft. They could be sent to Covid hotspots, so could lorries set up.
“If we had better treatment for covid…”
Steve-R astutely pointed out 2 very effective covid treatment protocols. MATH is for hospitalized patients and HCQ is best given early with an antibiotic and zinc. Works quite well. I’m aware of at least 3 other effective protocols. Of these, the most remarkable one that’s extraordinarily effective, simple, and affordable involves a steroid inhaler. Japan, Singapore, S. Korea, and Taiwan started using this strategy back in March for early treatment and all of these nations have had low deaths (e.g.Taiwan only 7 deaths). In contrast, in Western nations, institutional policy makers were instructing physicians to give patients with mild to moderate symptoms only palliative care. Patients were told to stay home, take a Tylenol/acetaminophen, and tough it out.
In March, Dr. Richard Bartlett of Texas independently began giving early to mid stage covid patients the steroid inhaler Budesonide via nebulizer (to fully penetrate affected lung tissues). He added an antibiotic and zinc for good measure but found the steroid to be the “silver bullet”. Well over 400 patients later, all patients fully recovered including some who were at significant risk with comorbidities, cancer, and at an advanced age (90s).
Below are links to 1) Bartlett’s website with the protocol and a case study paper with citations; 2) an excellent interview; and, 3) a clinical and scientifically detailed discussion with Dr. Mobeen Syed.
Note overlap of mechanisms of Budesonide with HCQ. >> Sharply lowers inflammation (reason HCQ is used for autoimmune disorders Rheumatoid Arthritis and Lupus), both antiviral, and both antithrombotic (prevents clot formation).
http://covidsilverbullet.com/
Dr Richard Bartlett interview (HIGHLY recommended for layperson perspective)
Bartlett and Syed
Thank you CP for the two links to Dr Bartlett, what surprising and delightful interviews. I think everyone would hope their own doctor would be like him and Doctor Syed.
What is remarkable is the fact that Dr Bartlett in using his training and compassion trying to help his patients stumbled on what looks like an effective protocol for treating early infection of Covid19
He also seemed a little nervous in what he had discovered.
It wasn’t a mandated treatment, he wasn’t following guidelines, would he get into trouble?
When he discovered other countries were using similar treatments he figured to hell with it, let’s get the information out there.
Every doctor I’ve ever met has been kind, compassionate, professional, but do they have a free hand to try out different treatments in an emergency like this, using their instincts and medical judgement?
I suspect not.
I don’t know what answer I would get from my GP if I went down with Covid19 and I asked him to consider prescribing me Budesonide and a nebulizer.
What is going on here?
What was wrong with Dr Richard Bartlett’s interview?
Was he violating Medical Practice?
Why has it been pulled from Youtube, this is a disgrace against, Science, Medicine and Free Speech.
Does anyone know where we can see the Censored Video?
Are you sure about your O2 kills viruses hypothesis. Could it not be equally the case that O2 saturated tissues increase natural cellular immune function.
Sorry, I haven’t got the background to answer that for sure. There’s no doubt that the viruses perish when tissues and blood are very high in oxygen. Maybe someone else would care to explain. I use the chamber, speak with other patients and have generally good technical understanding.
Hi Robert,
Here is as many references as you could wish for.
The Role of Hyperbaric Oxygen Treatment for COVID-19: A Review/SpringerLink
https://link.springer.com/chapter/10.1007/5584_2020_568
Over 50 refs for bedtime reading. Thank you for those, Agate.
Excellent article. My sentiments exactly. The Swedish were criticized in the beginning for their approach, and perhaps things could have been handled better for the elderly care homes, but in the end I think they did many things right. One caveat, though, they have a very good universal health care system and capacity which might not have been the case in all countries. However, I think we will see the same curves going down everywhere eventually, putting into question many assumptions made about the disease and especially the economic cost of a total lockdown.
I guess for the elderly homes they just ‘followed WHO recommendations’.
How the hell is it possible by the way that souvereign countries sign an agreement to implement the invasive ‘recommendations’ of a private party, financed by China and Gates, with no democratically chosen genocidal ex-terrorist leader into national law?! As described in the WHO International Health Regulations 2005!
because their institutions are corrupt from the inside
The trouble with these one issue thingys is that it just gets people staring at the dot. Don’t look at anything else, just keep staring at the dot. Keep all your attention on the dot. Let’s all talk about the dot.
I like to find the humour in things. I wonder if the whole response to the pandemic was made up by some yankee doodle?
You have a lockdown, you get the population to practice separateeism, the population can only come in to contact with one another through glass (or plastic) screens, the population must wear masks (closer Clarice). I wonder if everyone will have to start wearing orange jumpsuits soon?
It could be considered a bit of a cheek to implement all these things when you consider the population has bailed out the casino once again on a massive scale.
Oh well.
Ray: Good! In the U.S. we have seen the most massive transfer of wealth in our history from taxpayers to phony-baloney companies like Moderna, and convicted felons like GSK and Astra-Zeneca, among others, thanks to Trump’s ignorance (I am a Trump supporter, as the opposition is even more ridiculous; they make Boris the Clown look like a genius.).
Trump may be portrayed as ignorant, but https://youtu.be/zCJSH0vparQ shows a politician who has a fair grasp on reality, and answers questions directly. How often do we see that from the mealy mouth weasels?
I forgot to mention the ridiculous looking zombies asking the questions, perhaps they are yearning for their vaccine.
AhNotepad: These are examples of the famous American sheep. But they exist everywhere.
AhNotepad: I simply meant ignorant of scientific and medical issues (he takes a statin, for example). But this is true of the general public. The lockdown has been a disaster. Other than that, I think he has led us well, despite the best efforts of the swamp to remove him as President. Essential that he is re-elected.
If he could rid himself of all the warmongering bastards that have been put around him then he could continue avoiding all the banana skins that are being put in place to trip him up then I would be more sanguine about another 4 years as he seems war-averse.
The best reason to choose Biden is that the warmongers will have to regroup and spend some time to get into position to put banana skins in his path before they can engineer more global terror.
He comes a across as a bit of tw@t, but he hasn’t gone to war with anyone and that has to be good – if not a first!
Trump is the only one who is addressing the medical cartel with new laws to reign them in. He has reduced drug prices by allowing them to be procured abroad, put in legislation to have pricing transparency and I believe one more. No wonder they hate him. And don’t underestimate how he is upsetting their apple cart by promoting hydroxy.
When they did the ’08 bail out didn’t they say there could be martial law without the bail out? They should have called the latest bail out the SCARE act rather than the CARES act. 🙂
I’ve begun to wonder if the financial system is nothing more than a fleecing mechanism. In the UK people are big on calling people sheep, a term I hate, but when you start looking closely you can see this sheep notion appear in all sorts of places. The first appearance I can see starts very early, before you were born, when granny picks up her knitting needles and knits woolen booties and clothing in readiness for the new born lamb.
Years ago I’m pretty sure I’ve heard people refer to MPs as the speaker’s flock.
There are endless examples of sheep related things hidden in everyday life/activities, mostly disparagingly. It gets worse the closer you look.
I think we need to wait a bit longer (like maybe 6 months) before we can say for sure that COVID is over in Sweden. The Swedes certainly took a brave stance and it looks as if they were right. Like many people in this country my family has take antibody tests (mine provided free of charge by the NHS) and all were negative. Is it possible that we have immunity anyway? I wouldn’t like to bet on it.
It could be if they take steps to ensure that all their citizens eat a healthy diet and maintain levels of important immune system strengthening vitamins and minerals. And prepare to keep the vulnerable safe of course – once bitten and all that.
“Is it possible that we have immunity anyway? I wouldn’t like to bet on it.”
…… well Ian: you just hide indoors and keep away from everyone; and wear a mask in your car and stuff like that; long as you don’t have legislative power to impose isolation on others.
“I think we need to wait a bit longer (like maybe 6 months) before we can say for sure”; good on you; no evidence to support what you say; good on you.
Do we really normally wait 6 months to be able to say that the flu season is over? No. So why with this flu? Normally in the Netherlands there are 6,400 excess deaths from flu each year.
This year only 400. Plus 6,000 from ‘corona’. Just add up those last two numbers please…
HDB – Very interesting. Links would make that even more interesting.
Well Tom – frustration / rant really.
“COVID has at present killed less than 6000 in Sweden. It is very unlikely that the number of dead will go above 7,000. An average influenza year in Sweden, 700 people die of influenza.”
The average number of deaths in Sweden is a figure around 90,000.
I am convinced that the figure for the 2020 calendar year will be well below 7,000 above average, mainly because so many of the COVID deaths are people who would die within months anyway.
So the 2020 number will be something like 3,000 above average and be similar to bad flu years in recent decades.
Also to assess the real impact on society, you need to multiply the deaths by the life expectancy of the deceased (eg a 10yo child is not the same as an 80yo).
Flu is more deadly to children than COVID (median death age 82), so I think COVID is nowhere near as severe as the media is claiming.
One may add that the Swedish authorities omitted to protect the vulnerable. But unlike the rest of the (Western) world the authorities admitted their mistake. With a proper protection of the vulnerable the death toll would have been (much?) lower?
“proper protection of the vulnerable”
Hi Enrico; this has been a mindless chant, that reeks of virtue signalling and little else. So we lock up the elderly in care homes; no sunshine; no exercise; no contact; lock them in their own rooms; see no-one else; no visitors allowed; pass them food through slots in their doors; keep them like that for a year? 18 months? (Ian Roselman thinks we have to wait till at least winter to see if the rona has gone); so let’s keep them locked up and isolated for 2 years, to be really safe; to show we care; is that a long enough period of safety? to show our virtue?
That would be ‘improper’ protection of the vulnerable. Proper protection takes thought and proper levels of funding.
No, no, no and no. You don’t lock them up. You properly ventilate their rooms and if possible let them see visitors outside (I know… Sweden… 🙂 ) And above all: give them prophylactic hydroxychloroquine, ivermectin or even quercetin with a bit of zinc sulfate. Oh, and loads of vitamin D3. 10,000 IU/d, preferably in two doses as free floating D3 is very good for you.
Actually I wonder whether we couldn’t prevent the seasonality altogether by giving everybody high doses of vit D3 whole year through. That would prevent this kind of panic and make us less vulnerable for these bio-security scams.
Sorry, meant to say
The average number of yearly deaths in Sweden is a figure around 90,000.
well Jeff: Dr Rushworth above says
“A country with an annual death rate of around 100,000 people.” pistols at dawn?
Sweden has for long been The “bad Boy” during this Covid insanity!
Thank you Dr. Rushworth, and thank you Dr. Kendrick for posting this.
Thanks for the article. I’ve made a note in my calender to come back and check, whether these predictions were borne out.
Dear Malcolm
I really enjoy reading your blogs and like the fact that you offer an alternate and questioning view. My first impression upon reading the communication from the Swedish doc is he is using death as his measure of impact. The scientific literature is growing that this virus is debilitating and leaves scars with long-term respiratory, cardiac and neurologic symptoms which are not entirely understood. My point is, it isn’t just about whether the virus kills you. He may not in his position in an emergency department be seeing critical patients anymore but does he have an involvement with the follow-up or what happens post ICU? Other health professionals have to deal with patients with long term outcomes and may think prevention or avoidance is better than rehab.
I got the impression he thought lots of 80-year-olds are going to die anyway so the stats are misleading. I may have misinterpreted but I have many friends in their 80’s who lead active happy lives who I would be mortified if I contributed to their early demise so the economy could continue, or that I could still have my morning latte’, go to bars and dine out.
I live in Melbourne Australia and we are in lockdown trying to protect people. The latest surge or second wave has been with the younger generation. They are getting sick and whilst many recover often it is not before they spend 2 weeks in ICU. A debilitating pneumonia may not kill you unless you are old but many survivors describe how sick they are and how long they take to recover.
I ask is it okay to let the populous get so sick and for what gain. The disease is highly contagious, think of the loss of productivity if a large section of the community is at home sick. Is it really good to overwhelm hospitals and ICU’s and intubate people. At its peak in Italy if you were over 60 you didn’t go on a ventilator and were palliated. I am biased as I am over 60.
I reiterate “Death is not a good measure of how bad the pandemic is (unless you live in the U.S.A. or Brazil who think 150,000 deaths is ok)
I don’t think we will know which strategy is best for many years to come and a vaccine may not happen.
I know people die everyday but for the time being I would prefer that I am not one of them due to COVID and don’t really want to roll the dice and take a chance that it won’t kill or maim me.
Sadly, death is probaly the only even vaguely accurate measure we have. The rt-PCR test is unreliable and can’t really tell if you have the virus or not. If people with symptoms bad enough to require hospital treatment were counted, that might be a better measure – but you still wouldn’t really know whether they’d been ill with this virus or something else like bacterial pneumonia. Just counting “cases” ie people with or without symptoms who’ve had a positive test is probably the worst measure to use.
Thank you – I have the same thoughts you do. However, I’m in the USA and we (at least the sane among us) don’t think 150K deaths is ok at all. I’d like to add to your assessment one more item, and that’s that if 6000 people died in a country of 10M, that would be the equivalent of 200,000 people dying in the US. That’s just not ok. I realize we’re going to get there anyway because our leader is a giant orange baby and we’re stumbling through this and making it up as we go along. But no one in the US would – at any point – decide that 200K deaths is a fine price to pay, nor should they. But, great for Sweeden – glad it’s worked out for you, I suppose. I envy you your health care and your leadership. Thanks Malcolm for publishing this – it was worth the read.
The reason for most of the deaths is the lockdown policies, it has little to do with the effects of a virus, real or imaginary.
“The scientific literature is growing that this virus is debilitating and leaves scars”
Geoff: so many folks just want to go milking this business for ever and ever; folks get issues after flu; it is just that it is not hyped and now it is an industry to run all sorts of tests and report differing values.
“I live in Melbourne Australia and we are in lockdown trying to protect people”
well that is a big waste of time Geoff; many are alarmed at the extraordinary way the police are behaving; there is much data:it does not work; house-arrest only makes politicians feel good;
“The disease is highly contagious,” that is just what the media encourages you to say Geoff:
“At its peak in Italy if you were over 60 you didn’t go on a ventilator” Oh Geoff, this is all rubbish: the “Italian” problem was all just Lombardy: around Milan; famous for the worst air pollution in Europe; they lost 25,000 from ILI (influenza-like-illnesses) in 2016 and everyone just yawned and kept going. 68% of Italian deaths in Lombardy; 16% of I’s population. Sicily 8% of I’s population and 0.5% of mortality. You would have done ok in Sicily Geoff!! You are far more likely to die of cancer, or heart disease …….. PS take 5000 IU Vit D each day.
And the areas most affected had been given the dubious benefit of a new (novel?) 4 strain flu vaccine – including a new H1N1 strain. With hindsight and an understanding of the US Military study of vaccine interference that showed a 36% increase in susceptibility to a CoV infection among those – healthy service personnel – who received the flu vaccine the high levels of infection and death could have been predicted.
UK also used this vaccine last year
Pity that we will never see any stats on who had it and who had Covid.
There seems zero evidence of any link between the flu vaccine and Covid. New Zealand is a Popper Black Swan contradiction of this idea. Also, in the U.K. the vaccine is offered to over 50s but COVID deaths only rise steeply in the over 80s.
So if you have any evidence of this theory then say what it is.
Whether flu vaccination could be making people more vulnerable to other health issues is an area worthy of investigation.
I understand flu vaccination was pressed upon the elderly at first, but when that was seen to be not very effective it was pushed upon the rest of us, and continues to be pushed on the elderly, they even get their own turbocharged version now.
And as I’ve raised in other comments, ‘the authorities’ are now blatantly admitting they’re vaccinating children against flu to protect the elderly, and already have plans to do likewise re coronavirus vaccination, children are expected to bear an ever-increasing vaccine load. In my opinion this is unethical.
It seems to me annual flu vaccination is a con, this should never have been implemented. Likewise coronavirus vaccination. Turns out pushing annual flu vaccines was all about preparing for a pandemic, like what’s happening now…
The objective was to increase the use of seasonal flu vaccines so that production capacity would be in place in the event of a pandemic. But when seasonal flu vaccines are so questionable, why should a fast-tracked experimental pandemic flu, or coronavirus, vaccine be expected to be magically effective for all?
Here’s the evidence, a report produced by the World Health Organisation, published in 2006, titled ‘Global pandemic influenza action plan to increase vaccine supply’: https://www.who.int/influenza/resources/action_plan_vaccine_supply/en/
The WHO report is very interesting reading. It’s the blueprint for the global influenza vaccine industry, and the ultimate goal to vaccinate all nearly 8 billion of us… And seems like that’s coming to pass now, at Bill Gates’ behest.
According to the 2006 WHO report, countries are being encouraged to “develop an immunization policy to increase demand for seasonal vaccines” and “motivate industry to develop greater capacity for manufacturing vaccines”, i.e. press upon people a generally useless vaccine for a virus that is mutating all the time. And we have no idea of the long-term consequences of this annual revaccination.
To put deaths in context…
In Australia, so far 266 deaths have been attributed to Covid-19, 181 of these deaths are in the state of Victoria. Population of Australia is 25.5 million.
Most of these deaths are in the age groups 70-90+, i.e. 236 deaths. The breakdown is: 70-79: 66 deaths; 80-89: 104 deaths; 90+: 66 deaths.
It’s clear most of the deaths attributed to Covid-19 in Australia have occurred in the elderly, who are likely to have comorbidities. There needs to be more information provided on comorbidities for deaths across all ages.
The breakdown for other age groups is: 60-69: 20 deaths; 50-59: 7 deaths; 40-49: 2 deaths; 30-39: 1 death; 0-29: 0 deaths.
To further put this in context with mortality in Australia, according to Australian Bureau of Statistics data, “44,079 doctor certified deaths occurred between 1 January 2020 and 28 April 2020 and were registered by 31 May. This compares to a baseline average of 42,507 over the past 5 years. The highest numbers of deaths were recorded in the weeks ending 24 March (2,657), 31 March (2,776) and 7 April (2,746). Counts of deaths in those weeks exceeded historic averages by 624 in total, indicating that there may have been excess deaths during those weeks.”
In regards to excess deaths, I wonder how many of those might have been ‘lockdown deaths’, i.e. due to consequences of the lockdown, e.g. impediments to accessing health services, suicides etc?
References:
1. Coronavirus (COVID-19) current situation and case numbers. Australian Government Department of Health.
2. Australian Bureau of Statistics. 3303.0.55.004 – Provisional Mortality Statistics, Jan-Apr 2020.
“There is no second wave without a 2nd virus.” (Ivor Cummins)
What you have in Australia is just the 1st wave finding a new part of the population due to seasonality.
I find it appalling that also your government refuses to heal its affected population with hydroxychloroquine or ivermectin, with a macrolidic antibiotic and zinc++. It’s just criminal.
This cure is empirically proven to work and any RCT of sufficient statistical significance would be highly unethical due to the huge death rate in the control group. Just accept it.
You don’t need an RCT of 20 with a ‘control group’ of 10 jumping out of a plain to be ‘scientifically sure’ that parachutes actually do work.
The problem in the USA, which seems to drive this anti-hcq madness, is that if they accept this cure, no Emergency Use Authorization (which is Orwellian for: no need for thorough testing) can be issued for any other new and highly profitable drugs.
Geoff
The answer is not lockdown but better treatment. Lockdown kills. You should try reading some of the articles about that. I wonder how many of those left debilitated were put on respirators? For most people it is a big mistake. Why not start demanding of your doctors and politicians that the 4-6 highly effective treatments that I have read about be made available? Good treatment leads to fast recovery and little debility.
And don’t forget most of those healthy 80-year-olds will recover and not die.
Perhaps the average person in Sweden is much healthier than in the US where being way overweight, obese and diabetic are much the norm
Maybe that’s part of it. We should lock everyone inside until we find a vaccine for coca cola, twinkies, and similar nasty stuff.
It seems there’s another receptor, apart from ACE 2) through which the virus can enter the cell. I forgot the name of it but it seems to be carried more by fat cells. That would explain the higher severity of the infection in obese people.
Yes, cd147.
https://www.evolutamente.it/ace2-cd147-and-covid-19-a-tale-of-two-receptors/
Yes, it’s a much larger problem than covid 19 for all the reasons you gave as well as the veryinteresting podcast given by Sasca Stone interviewing Dr. Zach Bush. There is a bigger agenda.
Great post. I had the pleasure of going to college in Sweden in my wayward youth (is there any other kind?) and would love to go back with my family.
Yesterday was my youngest’s 10th birthday. I posted a picture of her and three of her friends about to gorge on donuts (yes, even low carbers let their kids eat treats) in a park. A friend posted something snarky about social distancing. It took a lot of self-control not to post a comment back that poked at my friend’s unwillingness to take care of his physical health and how this change would be more powerful than browbeating children into distancing themselves from one another. (He has fatty liver disease and is obese.)
In less snarky, happier news, I have a client who has lost 40 pounds on a ketogenic/carnivore diet since the start of the pandemic. So very proud of him!
Perhaps tell him:
People in glass houses shouldn’t throw stones 🙂
Children need to play. Period. And they are in no danger from this! Your friend has lost his mind.
“ Shutting down completely in order to decrease the total number of deaths only makes sense if you are willing to stay shut down until a vaccine is available.”
I thought the idea, at least originally, was to reduce the number of cases to relieve pressure on the NHS. Not least because our government was so ill-prepared.
Is there an argument for say, those who have retired (that would include me) to ‘shield’ and let the rest of the population get on with their lives and emerge into the sunlight once infection rates are sufficiently reduced?
There is an argument for stopping listening to the crap narrative from governments via the MSM. Watch UK Column instead and find out what’s going on.
I’ll give it a look, thanks
I like the idea of magical herd immunity, but we’re not seeing it in the US. We’re 6 months in with fatalities of 160,000+ and projections for 300,000 dead before December. In a two year period, the Spanish flu killed 675,000 Americans. While the author suggests it’s “nonsensical” to compare Covid-19 to other major pandemics, without a significant interruption (an effective vaccine, improved treatment, etc.) we’re actually on target to eclipse one of the most severe pandemics from recent history. https://www.npr.org/transcripts/899881918
One, I think we are reaching HIT, but it’s occurring state by state. I don’t think New York deaths have hit the floor based on distancing and masks.
Two, when Spanish flu hit, US population was less than a third than present; meaning the number died would have to be adjusted to about 2 million currently.
Three, we are the most unhealthy society in the history of the planet. We have to fix this part on a structural level. There will be more viruses and resultant catastrophes if we don’t. (And the cynic in me says we won’t bother tackling this because it is deeply rooted in profits generated by medical and food industries. Plus… it’s hard to change.)
Four, there is active restriction on the Hydroxychloroquine + azithromycin + zinc treatment that works to prevent the full-blown Covid-19 if administered early enough
Five, the most expensive healthcare provision in the developed World.
Seven, I am skeptical of those numbers and all mainstream projections have been overblown.
The projected deaths come from the murderous protocols of not using hydroxychloroquine, and getting as many as possible on ventilators. That way the hospitals get paid more.
Sweden are still socially distancing and are even considering localised lockdowns, Their leading epidemiologist stated this on BBC Newsnight yesterday. This is Anders Tegnell, they guy that came up with the whole ‘herd immunity’ strategy. He’s since admitted that this strategy was the wrong approach: https://nationalpost.com/news/world/top-epidemiologist-admits-he-got-swedens-covid-19-strategy-wrong
“He’s since admitted that this strategy was the wrong approach”
no he did not; that was the wicked MSM manipulating what he said; where did you come from Swampcreature?
Swampf0etus ?? U want to be taken seriously ?
I wonder to what extent, if any, the relative racial homogeneity and the effect of having socialism as a safety net has made it better, particularly given how hard people of color, who are more often people of poverty in America, are stricken? I also wonder if the Swedish people are less frequently obese.
Yes, excellent and informative post. The gentleman just oozes common sense from every pore.
Dr Kendrick, I really appreciate you entertaining the occasional guest post. It takes some pressure off of you (at least I hope it does) and provides some different and useful perspectives. Bravo!
Dr Rushworth said, “The reason we test for antibodies is because it is easy and cheap. Antibodies are in fact not the body’s main defence against virus infections. T-cells are. But T-cells are harder to measure than antibodies, so we don’t really do it clinically.”
Yes, we look for our lost keys where the light is better, not where we actually lost them.
By the way, the doctor has an interesting blog and a plain-spoken way of explaining things (I’ve read his blood-pressure entry). I like him already.
“I like him already”.
So do I. Indeed, since the beginning of 2020 I have come across all sorts of intelligent, sensible, open-minded and decent doctors online.
How come most of those who become rich and famous are such selfish lying jerks?
Anecdotal. Yes.
It’s always amazing to me, the degree to which people are willing to decree what’s what in the face of, as the the writer himself indicates, a challenge so new and little understood. This, from that single viewpoint, his particular hospital experience notwithstanding.
It’ll be interesting, one way or the other, what he says in his blog in a couple or three years – maybe even this Winter when people, particularly in the Scandinavian countries, will be sheltering from cold and snow. Indoors. Together.
As has been said – it’s a very large experiment. Endpoints not tallied yet.
Not saying he’s wrong. Or right. Just, the endpoints are not tallied yet.
But at lest the Swedes will have had a chance at getting some sort of immunity whereas we won’t, as we’ve all been isolated and masked, and many will have no job and no money for decent food or heating. How is that a good or sensible thing?
Ask the Swedish elderly how they feel about getting some sort of immunity.
Oh, wait . . . the ones that would have been most eager to answer that question –– they’re dead. Nevermind. No need for a job, food, heating.
That seemed a heartless and ill founded comment, can you say how you think it has helped?
Since when is truth heartless? Facts are what they are, nothing more. A little jolt of reality in the face of the self-satisfied conviction only otherwise displayed by religious converts can only be helpful.
Sometimes help can be painful.
Where are your “facts”? A self-satisfied conviction is not a substitute, nor is “a thought experiment” in the form of “Ask the Swedish elderly…….”. There is no evidence that “a jab” will give any immunity, whereas there are several treatments that would allow recovery. If you don’t believe there are you can read about them elsewhere on this blog. Better than a self-satisfied conviction that a jab or a lockdown is the solution to covid 19.
JD,
Quite simply, what would you have done to defeat death and nature herself? Lockdown kills, and it kills all ages. There are no good solutions. Killing people of all ages and ruining their lives to save some elderly is not the strategy of a sane society.
Your post is not only mean spirited but actually silly.
You got one thing right: there are no good solutions.
Try sorting out the sanity here:
Mid May:
Most of the 3,698 people who have died from coronavirus in Sweden so far were over 70, despite the fact that the country said shielding risk groups was its top priority.
Sweden, with 10m inhabitants, has kept more of society open than is the case in most of Europe.
“We did not manage to protect the most vulnerable people, the most elderly, despite our best intentions,” Prime Minister Stefan Löfven admitted last week.
The Swedish Public Health Agency told the BBC that 48.9% of deaths were care home residents up to and including 14 May.
…as in many European countries, relatives, staff and union officials have shared concerns that protective clothing arrived too late, and that some staff may have gone to work at the start of the crisis despite showing symptoms of Covid-19.
“They told us that we shouldn’t send anyone to the hospital, even if they may be 65 and have many years to live. We were told not to send them in,” says Latifa Löfvenberg, a nurse who worked in several care homes around Gävle, north of Stockholm, at the beginning of the pandemic.
“Some can have a lot of years left to live with loved ones, but they don’t have the chance… because they never make it to the hospital,” she says. “They suffocate to death. And it’s a lot of panic and it’s very hard to just stand by and watch.”
Mikael Fjällid, a Swedish private consultant in anaesthetics and intensive care, says he believes “a lot of lives” could have been saved if more patients had been able to access hospital treatment, or if care home workers were given increased responsibilities to administer oxygen themselves, instead of waiting for specialist Covid-19 response teams or paramedics.
“If you need care and you can benefit [from] care, for example, or oxygen for a short time, you should have it. Like any other age group in the population,”
Late June:
Even more detrimental to Sweden’s credibility is the fact that a large portion of deaths has occurred among the elderly—the very people the strategy was meant to protect. To many, this is proof that Sweden’s strategy has failed. Even Anders Tegnell, Sweden’s state epidemiologist and the architect of the light-touch strategy, has admitted that too many people have died and that, if he’d had the information available today back in March, he might have supported stricter measures within certain sectors of society. However, Tegnell still maintains that his overall strategy has not failed and that no one knows exactly what measures should have been taken.
Of course, it would be easy to dismiss Tegnell’s comments about “potential for improvement” as an abdication of responsibility. But a closer look reveals a more complex reality. Some criticisms of the Swedish COVID-19 response may still be premature, and others should rather be directed at mistakes made long before the current health crisis—namely the decline of central government oversight and, especially, a decadelong neglect of Sweden’s elderly population.
On May 6, a report showed that in Stockholm County, residents had been infected in 212 out of 400 nursing homes. An ensuing report showed that as of June 1, 2,036 people age 70 or older had died from COVID-19 in nursing homes across the country, while an additional 1,062 who died of the coronavirus received professional care at home.
In the case of Sweden, a report from one of the country’s largest labor unions shows that 40 percent of its members working at Stockholm nursing homes are unskilled workers employed on short-term contracts with hourly wages, while 23 percent are temps. That means younger people working multiple jobs, which means more points of contact and higher risk of transmission. Certainly, a lockdown would have reduced the risk of these workers getting infected while having drinks or traveling on crowded buses, and it would also have kept family visitors—some of whom may have been asymptomatic—out of nursing homes.
Sweden’s 5,161 fatalities from COVID-19, as of June 23, represent a death toll of 511 per million inhabitants, compared to 46 in Norway, 104 in Denmark, and 59 in Finland. Swedes, and the rest of the world, are now wondering why Sweden failed where its neighbors did not.
…by the end of April, authorities admitted to failure, with Health and Social Affairs Minister Lena Hallengren stating: “We failed to protect our elderly. That’s really serious and a failure for society as a whole.”
JDP, like elizabethhart, I don’t understand your expectations. Knowing what we know now, it seems hydroxychloroquine as a prophylactic would be a very useful prevention. Unfortunately there are plenty of politicians and pharma paid “scientists” who say it’s toxic and doesn’t work, but then toxic level doses, late in the diseases progress, is no use. The correct doses, with zinc, early on means most people recover. That wasn’t known early when the panic first started. So there is an effective, preventative treatment, which those with vested interests are trying to stamp on.
So, basically, they deliberately killed their elderly just as we did in UK. But at least they had the decency to apologise, which the NHS did not. And they’ll still have an economy, unlike the UK. So sounds better to me
JDPatten,
I don’t think it is fair to focus on Sweden’s policies which were identical to nearly every other country. Care homes have the same problems everywhere – lots of staff who often work in more than one place. Norway has smaller care homes and thus fewer were infected. Every year many elderly are lost to the flu, so it is a given that more of them will be lost but the big issue for me was the premature closing down of hospitals that were not overwhelmed.
What exactly do you want JDPatten? What response do you expect to this virus?
In response to this virus, this is what’s happening in Melbourne, Australia – do you think this is a proportionate response? This is from the Institute of Public Affairs website:
This week, the Premier of Victoria has imposed what is by far the greatest incursion into our basic liberties that we’ve ever seen on Australian soil. Almost five million people are under curfew. Private property can be seized by the Police Minister for any reason. Police and even the army can enter your home without a warrant, and stop you in the street to check that you’re carrying the permit that allows you to leave your own home. And worst of all, businesses have been closed, jobs have been destroyed, and Victorians everywhere are losing hope. Many shops that have shut their doors will never reopen. Many people who’ve lost their jobs may never work again.
This is from the video on this subject on the IPA website: Research by the Institute of Public Affairs suggests that stage four lockdown will rob mainstream Victorians of almost 3.2 billion dollars a week in lost income, prosperity and living standards. And we can expect as many as 300,000 jobs to be lost. Why are we being put through this? Is this cruel and undemocratic lockdown really proportionate to the risk? Will the poverty and mental crisis be worth it?
Again JDPatten, what do you want?
elizabeth,
It’s not a question of what i “want”. As anna said, there is no good solution. Yet. I have hope – says me the optimist.
It’s a question of supporting people who are wracking their brains in the Real World trying to figure this thing out. It’s still so little understood, but real efforts are being made. And I’m certainly NOT talking about political efforts.
This guy, for example:
And this fellow:
What I would like is for it to be acknowledged that that there is a long way to go still. Things have been done wrong and will be again in the way forward. Recule pour mieux sauter.
JDPatten,
I find it odd that you won’t give an opinion on the intelligence or lack thereof of the lockdowns which are so draconian, and also very willy nilly from place to place. Have you read articles on how the lockdown really affects populations? Instead, you seem too focused on the abstruse points of study – which is fine but I have heard of at least 4 very accessible treatments that actual doctors who are treating actual covid patients are using with great success. But from you – silence. Do you want solutions or not?
Here is a link to some thinking. https://youtu.be/6RDffMCAujg I have posted it as separately before I saw this moe appropriate place.
Are you quite finished, anna?
I won’t argue with someone who seems to have such strong emotional attachment to her convictions.
I won’t try to reason with highly opinionated people when there’s not enough intelligence to have opinions.
I will tell you that I’m doing all that seems reasonable to me to avoid this disease.
If I go out to shop, it’s as if I’m taking my partner with me. Same exposure. If my daughter is forced to teach in her school, she is virtually taking her partner with underlying conditions with her. I think in terms of the most vulnerable in my cohort. I lock myself, and mine, down. No problems. Masks, distancing – fine.
No need to reply. Just read my initial note again, from Aug 7, above. Done.
“I won’t argue with someone who seems to have such strong emotional attachment to her convictions.
I won’t try to reason with highly opinionated people when there’s not enough intelligence to have opinions.
I will tell you that I’m doing all that seems reasonable to me to avoid this disease.’
As this is a site that is probably read by many who do not go on to post here, then statements may deserve a response so people can have a, hopefully. balance in views so they can come to their own decisions without undue pressure. It could reasonably appear the writer of the above (I am not referring to anna m) also had a strong emotional attachment to their conviction. And maybe there is little point in attempting to engage in reasoned argument.
anna m does however have enough intelligence to have an opinion. All that seems reasonable to avoid this disease may differ from one person to another so some may believe masks will reduce transmission of the virus, despite the size of a virus compared to pores in a mask being the equivalent of trying to carry grains of sand on a tennis racket.
The Centre for Evidence Based Medicine has a word to say about that https://www.cebm.net/covid-19/covid-19-masks-on-or-off/
AhNotepad,
You seem to feel that certain views, such as mine, are in need of “balance” through the forceful application of your own which, of course, are incontrovertible. Welcome to the world of teeter-totter.
I think you’ll find ultimately that the virus nor COVID-19 cares the least about balance.
What I worry about is what the casual reader here might take away, having read the convictions of someone whose sources of knowledge are so carefully chosen.
Who is to balance the great self-declared “balancer”?
JDPatten: Please list your sources of knowledge, whether carefully or carelessly chosen.
JDPatten, you say “What I would like is for it to be acknowledged that that there is a long way to go still.”
So are you expecting lockdowns to continue indefinitely? For people to be masked and hindered from leaving their homes and associating with others, and under curfew indefinitely? For society as we know it to fall to pieces?
Is that what you want?
JDPatton has accused me of being way too strong in my opinions, but the way I saw the situation is that JD insulted the commentariat of ignorance repeatedly, but then his own opinions needed clarification for logic, and he could not produce anything of use. I tried to get the logical conclusions from his remarks, and apparently there is none.
(Good grief. Let me try this again)
Of course I’m not putting out opinion. That’s the point. There is not enough clear knowledge to form a coherent opinion. That’s true of Fauci who has, indeed, stated that his suggestions and advice (not mandates) throughout the COVID-19 problem have been based on the best information he has had at-the-time. It’s in constant flux. That “information” has been incomplete, misleading, suggestive of other known viruses, and just plain wrong.
The same is true of Fauci’s boss Francis Collins, of Deborah Birx, and of the many virologists and epidemiologists who work in those labs, and of the many many who work in the private sector.
But these people are out there thinking, searching, trying to get a handle on this elusive thing. They’re certainly better positioned than I.
I am ignorant of way too much to have consolidated notions as to what this is and what to do about it. I think it’s true of virtually everyone here.
So, if you perceive this as insulting, that’s on you.
I’m more worried about folks putting hardened convictions out there as obvious “evidence”, that probably have as good a chance of being wrong as being right.
That, my friend, can be dangerous. Concerned people are reading and listening, ready to take on what they want to hear as true. We’re all vulnerable to that, more-or-less.
If you want to talk about politics and mandates, etc, I’m outta here.
Ha! governments put out hardened convictions all the time. According to them, lockdown, anti social distancing, isolation, masks, have all “controlled” the virus. Now Fauci, using his best up-to-the minute information is suggesting goggles will have to be added to the armoury.
Well your post was certainly an excape from what appeared to be your convictions of vaccines and masks were the answer, or are you now saying that was never what you said?
As this blog seems now to contain a lot of political influenced comment, I wish you well in your new found sites. Or did you not mean you were really “outta here”?
Calm yourself, lad. I’ve always been here for the actual medical content. Since before Roman numeral I.
Show me some of the many accelerated trials starting to come in now and we could conceivably have a conversation. I mean actual randomized controlled trials on COVID – which the subject seems to be now and for awhile – not observationals, not theories from other social media.
(The phase III trials on covid vaccines are not in yet, so that’d be premature.)
Science.
I’m certainly not here for the political content, nor to discuss what governments do.
Yes, except COVID long ago stopped being, primarily, a medical issue, and has turned itself into a financial, moral and political issue. Almost no science underpins the decisions that have been made.
anna m: He has painted himself into a corner, and refuses to admit it. The full genome of neither SARS “virus” has ever been sequenced, so we really don’t know the significance of what the “tests” are finding, and the rtPCR test cannot be correctly used as a diagnostic tool. There have been excess deaths in some parts of the world, but we really don’t know the causes, and there must be more than one cause. Some are clearly iatrogenic, due to ignorance or incompetence, but the demographic affected makes this an unusual infectious epidemic. Coming later in Spring is also unusual. But it clearly has ended, as the Fat Emperor’s graphs show.
JD,
That is fine if you want to leave it at that. You worry a bit too much that people have to be protected from free discussion. Everyone knows that we are all giving our best opinions and no one is expected to be taken as an expert. I think we all know that.
As for Fauci, you give him the benefit of the doubt and I do not. He has been in this area of expertise for 40 years. If he doesn’t know by now whether face masks offer significant protection then he is a fool or incompetent. He gave us his honest assessment a few months ago – healthy people should not wear them, they don’t make much difference and have downsides, and would mostly make people feel better emotionally but could also give a false sense of security. That is also in complete agreement with the many scientific studies done for decades. Done on, you know, viruses. Albeit the flu virus is about twice larger than the corona and so masks would therefore be even less likely to be effective for it. Obviously “they” decided to change the agenda and promote masks so he went along with it. This is called politics. It isn’t really science. Could that be possible?
Hi anna: possible explanation of what is happening to medical scientists
A dubious treatment (or idea) can be promoted by a charismatic person, ie a bandleader. The more people that jump on the bandwagon the more effective the treatment will appear. All politicians are now on the mask bandwagon. We are all susceptible to the “bandwagon effect”, perhaps politicians depend on it.
There is no need for so many people to be dying from COVID-19.
Dr Paul E. Marik, MD, FCCP, FCCM, of the
Eastern Virginia Medical School in Norfolk, Virginia
has a protocol that has a 95% success rate. He can’t get main stream media to listen to him.
COVID Protocol(updated March 24, 2020)Paul E. Marik MD, FCCP, FCCM
Click to access COVID-ProtocolPaulMarikMD-1.pdf
Full interview with Dr. Paul Marik
CW
I’ve noted that Sweden has similar rates to Italy, Spain and France, (all of whom also have similar rates of vaccinations for the over 65’s.) I know that at some time France made HCL widely available. I saw something to the effect that nations with freely available HCL had CFR’s of 30 or 100 despite in some cases rudimentary health services. BTW, I read that Green Tea has a similar but less effective chemistry as HCL.
Switzerland accidentally performed an experiment with HCL by banning it on 27th May and reinstating it 13 days later. Judge the results for yourself.
Some data suggsts that Covid-19 fatalities are loosely connected with vaccination rates for the over 65’s.
How refreshing to read something in line with what I have believed from the start. This virus SARS-COV-2 is a virus, a bad one, but still a virus. As such it will run its course and another virus, or another strain will come along. We have had viruses before, we will have them again. But this is the first time the world has been shut down because of one, and everyone has been made to look ridiculous wearing masks as an everyday occurrence. Masks are more likely to cause problems with continual use breathing excess carbon dioxide.
Thank you so much. It is refreshing to hear a voice of reason in a world of dictate.
One can’t extrapolate Sweden’s result to other countries. Sweden’s death rate has petered out at 574 per million of population. I calculated the death rates for the UK and the hard hit New England states.
UK – 698
New Jersey – 1784
New York – 1295
Massachusetts – 1264
Connecticut – 1244
Rhode Island – 958
The results in New England were after lockdown measures. I find it hard to believe that various restrictions aren’t required to keep the spread under control. The current US forecast is for a total of 300K deaths by December 1 without enforcing mask wearing or 230K with it.
So areas with lockdowns did worse than Sweden, which is why you can’t extrapolate – it would show that we destroyed our economy for nothing. All the stats show that death rates followed the same pattern regardless of lockdowns; a surge a week or two after lockdown started followed by a rapid fall – Sweden had a smaller surge, presumably because it didn’t have a lockdown.
A fly lands on your nose. So naturally, you fire a double-barrelled shotgun into both your feet.
The fly goes away. Obviously it did so because you shot your feet off.
Yes, KJE. And here are some data for New Zealand, a country whose PM has been lauded for her attack on the deadly disease. Lauded, as I see it, for a myopic fixation on one issue. In such a world anything that get’s in the way is likely to receive a Maggy like “No, No, No!”
https://www.nzherald.co.nz/business/news/article.cfm?c_id=3&objectid=12337073
The US forecast deaths for no masks is unsupported by fact. It certainly has not been made taking into account the report on the CDC website https://wellnessforumhealth.com/nonpharmaceutical-measures-for-pandemic-influenza/ which says the non-pharmaceutical interventions have no statistical significance, ie, they don’t work. What would work is hydroxychloroquine as a preventative measure, but the tyrants don’t want that.
Richard; one can only talk excess deaths: the US is now famous for massaging the data to call everyone who dies, as dying of … it is breathtaking to see you believe the US data. The only surety seems to be that living in a red state is much healthier than in a blue state: rates from the blues are up to five times those of red states: so time to move to a safer state!!
Terry Wright: This is indeed a very interesting anomaly. I suspect one of the main factors is that Democrat-controlled states are generally more densely populated. Also, they all adopted the most draconian measures, and some of the Republican-controlled states did not. We do know that the death-rate spike in the U.S. occurred within a week or so of the lockdown orders, peaked, and declined to background rates after about three weeks. This is a clear indictment of our government’s response; that it was the fear induced by media and government panic which caused this spike, not the ‘Rona.
We have a small shrub which we commonly see on our hikes: the gooseberry (Ribes). The berries look just like the artist’s rendering of the ‘Rona. They are now ripening to a rich reddish-burgundy color. We laugh every time we see one, and now call it the ‘Rona berry! They are good made into jam, but you need gloves to pick them.
So the whole point of whatever you are quoting here is to enforce masks, which is a horrible agenda and is a propaganda piece for it. Masks are a filthy habit and do little or nothing to avoid spread. Try not believing whatever the mainstream media puts out.
I seriously want to scream when I hear this, knowing we are living in a state/country that is COMPLETELY ignoring these facts. I feel imprisoned by ignorance, “religious” bullying about masks, denial about the falling death rate, the absence of hospital crises and the COMPLETE absence of acknowledgement of science. Add to that the rising unemployment rates, rising depression rates, failing businesses, sad cries of the isolated elderly and really–I cannot comprehend that the masses are quietly taking this up the tailpipe as though there is NO alternative. And whatever you do—do NOT present an opposing viewpoint! You will be quickly silenced, your right to free speech turned into a hate speech/racism or any number of other titles for simply saying “How about we present real facts, the actual numbers, the falling death rate and the GOOD news”!!!! We are a world completely turned upside down! Thanks for helping me realize I am not actually crazy for seeing this the way you do. A great article by this doctor. Keep it coming Dr. Kendrick–I await your blog posts as a drowning citizen in need of a life preserver!
Judy, whatever you do, don’t go to Melbourne, Australia. They have declared a “state of disaster”. Why? Eight people in care homes have died from or with covid, One was 50, and the others were in their 70s, 80s or 90s. But the madmen are ruling Australia
Mate, you couldn’t get here even if you tried. I live in Melbourne CBD. Police and army personnel walking around waiting to pounce on anyone not wearing a mandatory muzzle. I can only go outside to exercise for 1 hour a day. Must not break curfew between 8pm and 5am. Can only go out to purchase groceries once a day, and must never go beyond the 5km radius of my apartment. Luckily my son is deemed an essential worker, so if he has the correct paperwork filled out by his employer (Nazi Germany anyone?), he is ‘allowed’ to go beyond the 5km limit to his place of employment. This is the only human contact I have now. Unfortunately I can not see my daughter and 3yo grandchild, nor my brother and sister, nor my elderly mother, nor my friends.
I am lucky enough to still have a job working from home, but when we have our online meetings, all anyone can talk about is today’s case count and deaths. They are actually waiting for the MSM press conference announcements. Their mind set is of complete fear for most of them. I have given up trying to get them to even consider another point of view. I’m shouted down as a tin-foil-hat conspiracy theorist. The MSM has done an outstanding job of selling this BS.
So I do not share the same sentiment as [Geoff Magrin F.A.I.M.S] comment further up the page. How long does he think his 80yo friends are willing to see the rest of their life pass before them locked up in their homes? Six weeks? Sixteen weeks? Sixty weeks?
I’m horrified by the political situation in Australia in relation to the handling of this virus. Elected representatives of the people have grossly over-reached in exerting control over those they are meant to serve. And now unelected individuals, i.e. Federal and State medical officers, and various academics, are influencing policy with little or nothing in the way of accountability.
There is something really rotten afoot in Australia, and this has been building for some time. This is so much about ‘the vaccine’, and plans to impose this on the entire population. The groundwork has been set, with the coercive Federal No Jab, No Pay vaccination law implemented in January 2016, and No Jab, No Play laws subsequently implemented by the States. These coercive vaccination laws were campaigned for by the Murdoch newspapers, News Corp, which is also a corporate partner of the Murdoch Children’s Research Institute, which is involved in vaccine research and development, a massive undisclosed conflict of interest.
Coercive vaccination lobby groups such as SAVN and Friends of Science in Medicine were at the forefront of the campaign for coercive vaccination, and were privileged by representation at the Senate Hearing on this matter.
And in 2015 the Australian Biosecurity Act was enacted. My reading of this Act indicates Australians could be compelled to have vaccination in an emergency, e.g. coronavirus vaccination, with the penalty for refusal being five years imprisonment and/or a $63,000 fine. I’m seeking clarification on this matter.
It’s shocking that such legislation could be slipped through the Parliament without the general public being consulted.
These are very grim times indeed, and it’s not just about the virus…
Glenn, thanks for posting about the living death in Melbourne. As for the elderly, the older we get, the nearer we are to dying, but the way elderly people in Melbourne are treated would result in law suits against the government if the same was applied to prisoners locked in solitary confinement. I hope someone finds a way to take these ne’er-do-well power crazed politicians to court where their crimes can be exposed.
AHN – I know I’ll get thumbed down for this but we cant put all the blame on politicians. They depend on the “experts”, appointed through “proper” procedures, and trained to figure this sort of thing out. If much of their funding comes from the largesse of vested interests that might influence decision making, the and that’s not good. (Is there a law that requires decision making to be in the public interest punishable if the decision has been proven to deviate from that overwhelming obligation – for whatever reason?) How can a politician go against the professional advice and live to tell the tale ? If he’s brave he or she will try. Trump for all his faults appears to deal with nonsense but gets slaughtered by the media. Politicians are so because they listen to the people (cue argument), act in accordance with electorate’s wishes & societal concerns while weighing up all the variables to get a line of least resistance. If the population is misinformed and experts either (let’s say it) bribed or protecting their own patch to exclusion of all else then bad laws will follow unless the lawmakers are inspired with common sense and political heroism. The latter might see them cast among fools.
Jerome, I agree with your post, but the politicians are quick to claim the credit when things go well. They are quick to blame identifiable others when things go badly. They are prepared to blame the whole population if they can’t identify anyone. There is plenty of information about this low consequence infectious disease, but politicians almost everywhere seem to believe the same thing, why can only a few countries get things roughly right, while most are on a course of total destruction of the human spirit?
Jerome, I think you have identified a key point. What this epidemic has highlighted is that – as Carl Sagan wisely pointed out – “We live in a society exquisitely dependent on science and technology, in which hardly anyone knows anything about science and technology”.
In particular, our political leaders (and most of our business executives too) know very little about science and technology. Most of them are profoundly ignorant even of basic mathematics.
Meanwhile we have very many clever, creative, experienced scientists, engineers and doctors. While some of them will be wrong about any specific issue, there must be some practical way of consulting them as a community to find out the truth.
What we have all learned this year is that our leadership is hopelessly disconnected from our technical expertise. Why has policy completely ignored the advice of such experts as Dr Kendrick, Dr Ioannidis, Dr John Lee, Professor Sunetra Gupta, Professor Giesecke, Professor Denis Rancourt, Professor Carl Heneghan, Tom Jefferson, Ivor Cummins… and of course the 30 experts cited by Off Guardian as long ago as March and April?
Our political leaders are clearly unable to follow “the best scientific advice” because they don’t understand the first thing about science. How could a person who knows no mathematics judge the validity of a complex proof in number theory?
The Chinese political leadership consists largely of qualified engineers, scientists and mathematicians. It is likely that their average IQ is as much as 35 points higher than that of our leaders. See Frans Vandenbosch’s essay “The Dictatorship of The Idiots” at https://mailchi.mp/cf6863e85eb1/mars-fibs-cancer-detection-taiwan-having-a-chinese-baby-7208420?e=4e445d69e8 (honestly – that is the proper URL!) about three quarters of the way down.
What do you think about this…?
Coronavirus: Victoria facing years of mandatory masks and restrictionshttps://www.news.com.au/world/coronavirus/australia/coronavirus-victoria-facing-years-of-mandatory-masks-and-restrictions/news-story/7b2b9fccb48f9c0b5c62af3769d7c3c5
Just one point (as there are too many) the idiot Dan Andrews seems to understand nothing about disease transmission. Hope-Simpson should help him. Second comings are usually less virulent than the original. If not, we would all have been wiped out millennia ago by self-amplifying pathogens. The politicians and the unelected imposers had better have good protection, or they might not be long in this world.
Hi elizabethhart: premise > voters want smart leaders. Conclusion > I was elected, therefore I must be smart. Cognitive distortion.
Re the situation in Melbourne, have you seen this article Madness in Melbourne, by Jeffrey A. Tucker of the American Institute for Economic Research: https://www.aier.org/article/madness-in-melbourne/
Click on his name on that article for other articles re lockdown. I haven’t read them all yet, not sure he’s onto the global vaccination agenda that’s so much a part of this.
AhN, don’t forget that one recent – tragic and totally unexpected – death in Melbourne was… a Centenarian….
Yes, there has been a 30-something also deceased, but as usual, no information is likely regarding his metabolic health..
Speaking to my son about COVID-19 this morning, before reading the Swedish doctor’s submission, I said that I really would like to move to Sweden. It appears they are imbued with . . er . . um . . What is that we seem to have misplaced or forgotten about in the mists of past times ??? . . . Oh I remember: “Common Sense”
Well you’ll have to move to Sweden before December 31st 2020 assuming you’re British otherwise you’ll need a visa.
I have to admit, I’m totally flummoxed by Sweden. Even my family members that live over there can’t tell me what they did or are doing. But I’m hesitant to say it’s over there. I predict it’ll get worse again before it gets better.
And what seems to work for Swedes doesn’t seem to work well for the US. Follow a doctor out of McAllen, Tx. He went from 3 covid patients in his hospital to doing nothing but seeing covid patients and “treating STEMIs” according to him.
The RGV (where McAllen is) hits 1,000 deaths (and this happened very quickly):
https://www.newsbreak.com/news/1612169940418/gonzalez-laments-valley-passing-1000-covid-deaths
Morgues and funeral homes getting hit hard:
https://www.newsbreak.com/news/1612547578009/extraordinary-high-rate-of-covid-19-deaths-in-the-valley-straining-morgues-funeral-homes
They’ve had to use their convention center as a covid hospital:
https://www.healthleadersmedia.com/welcome-ad?toURL=/covid-19/now-hospital-facility-mcallen-convention-center-begins-taking-covid-19-patients
As for everyone getting immunity, I’m not sure about that. We (CT, USA) were on lock down and still lost 4,000+ to the virus. But this means we have plenty more people who can get it, as they haven’t been exposed.
And I don’t even know how you test this. The Tcell issue is one I don’t fully understand. Some say 99% of people have antibodies if you do the correct test. Others say people get Tcell response but no antibodies. It’s not clear what this means, as there is no test outside of a lab that can test for Tcells.
And serology is a two-sided sword: its predictive value is low when the prevalence of the disease is low:
https://www.cdc.gov/coronavirus/2019-ncov/lab/resources/antibody-tests-guidelines.html
You have to get a second, orthogonal test to rule out covid.
I personally am withholding my thoughts about Sweden until Spring of next year and also until we can adequately test to see what the true immunity is. Until then, I don’t know well Sweden has done or is doing.
And of course, we all look through our own lenses and filters. Looking at Sweden, you can also get a pretty bleak picture presented to you, if you choose to look through that type of filter:
https://www.usatoday.com/story/opinion/2020/07/21/coronavirus-swedish-herd-immunity-drove-up-death-toll-column/5472100002/
“And I don’t even know how you test this”.
Yah. We are facing extinction at the hands of a disease which has no unique symptoms and for which there is no halfway reliable test.
Like the fellow who still had his grandfather’s axe. His father had replaced the handle and he himself had fitted a new blade – but it was still the original axe.
Extinction event by means of reaction to disease you don’t know you had until you are tested.
All my life there were drills. Now its gone live.
No one can escape a problem that is generated by their own reaction, to fear they are in it – given belief and priority over all else.
For the very attempt to escape from a false premise is its reinforcement.
And having invested so much emotional energy in its drama is to inhabit a protected identity gotten from reaction.
Another way to see this is of invested illusions being ‘reeled in’ for deconstruction, for the only ‘immunity’ or ‘resilience’ is the extension of love. Only love identifies truly by giving of itself, That is, one has to extend love to know one has it, and to be willing to receive as the law or nature of its sharing.
Masking in virtue is generated on fear of lovelessness, and runs as a contagion that does not actually share of communicate but runs as fear of love, transparency to life, relationship and communication. Fear says “Keep apart to stay together” for to fear locked into lie, separation is salvation from undoing.
In a time of open attack on love, we might discern the mask from the truth. It isn’t the mask that locks the mind in fear, but the power given it as a means of defence.
I could have used the term ‘world’ for mask – except there is a real world to inherit and share in as the gift of love. How do we live or love in a falsely framed world? We don’t – but we can mask in symbols of love and life and defend them. Love casts out fear, but masking in love locks the fear in. Love of truth is the true foundation of science as the willingness to uncover the already true.
BobM,
You have to be incredibly cautious about media stories about CV-19.
One example is the story about bodies piling up at morgues. I read later that this was entirely because the coffins of CV-19 victims were held back to be handled in special facilities!
1600 people die per day on average in Britain (without CV-19) and the death rate attributed to CV-19 never got near that – so why else would there be problems burying/cremating the dead?
I agree, spring 2021 will reveal all, but where will the economy be by then, and will we ever get the kids back to school again?
Where will the structures and regulations of social order be then, and will we even be allowed a say in what ‘our kids’ are taught, or trained in? Will kids and the permission to have them be a matter of state dictate? Does a god of ‘control’ mask in powerlessness?
Very impressive.
I look forward to read more from Professor Rushworth.
I wish my country had even one doctor like him.
We need clear thinking more urgently than any vaccine!
Thank you. Very interesting. Take a look at the restrictions in Victoria, Australia. Insane.
Tell me about it! I live there.
Very interesting
Thank you
Hallelujah……..common sense at last
Interesting article. One problem the U.K. had/has is that there isn’t any spare capacity in the NHS. The last winters in the U.K. have been a struggle with scheduled procedures being cancelled, really long waiting lists and patients being treated in corridors.
One of the rationales for the lockdowns in the U.K. was to prevent hospitals being overwhelmed and with zero spare capacity that was a real risk. If you only have 15 ventilators what do you do if 30 patients need them for example.
It might be very different if there was spare capacity in the health system and I wonder if Sweden had that luxury.
You mean which lucky 15 are going to be put on a ventilator that has an 80% chance of killing them?
without the ventilator they had a 100% chance of dying so 80% is better is it not?
Sorry, completely wrong. Ventilators probably killed more people than they saved.
So what you’re saying is the hospital clinical teams chose a treatment that they knew would ‘probably’ kill the patient? That’s quite a statement.
You are a man that loves a straw man argument. I never used those words. They are your words. Please try again. I have no interest in playing debating team games. Doctors thought ventilators would be a good thing. It turns out they were not. For most people
A clarification which is helpful with a side order of insults which is unhelpful.
There was no insult, that was a mild response given you had done a Channel 4 Kathy Newman “so you are saying” tactic. You can expect this to not go down well.
Hi Dr Kendrick, thank you so much for your blogs they are really appreciated! I have just come across this article which I thought that you and your fellow followers may have an interest in.
https://www.townsendletter.com/article/online-covid-19-ards-cell-free-hemoglobin-ascorbic-acid-connection/
Or did they? perhaps if they’d been treated with Math+ or HCQ early or even given oxygen in another way, they might have had only 5% chance of dying. Who can tell? But keeping on doing things that don’t work is one of the definitions of either madness or stupidity
Con – you are putting words in people’s mouths. The SUN newspaper might be recruiting. Only saying !
Cón, where do you get the idea the UK NHS has no spare capacity? most hospitals are nearly empty at present.
I have to ask have you ever been to an NHS hospital? If the NHS wasn’t overloaded, the private sector wouldn’t exist.
I work in the NHS in hospitals. The overloading of the NHS, with COVID, has nothing whatsoever to do with the private sector.
I was talking about the NHS before COVID. Those that could used the private sector to sidestep long waiting lists in the NHS. Pre COVID, long waiting lists, staff shortages, lack of hospital beds, last minute operation cancellations were reported on and having experienced all of these myself, I believe this to be a true picture. This was way before COVID.
The original point was whether Sweden did well simply because it had a better health system when COVID came along. Sweden for example has about 39 doctors per 10k, the U.K. is something like 23 per 10k. A crude metic I know.
Well we splurged on extra hospitals and intensive care beds equipped with ventilators ….. and then mothballed them all!
Cón Ó Brolcháin: Good point. Austerity has resulted in both Italy and Spain partially dismantling their hospital capacity, so they were and are unprepared for increased demand, and apparently in Lombardy privatization has reduced access to primary-care doctors.. Germany, on the other hand was and is well prepared. Don’t know about the UK, but in the U.S., in most places, we are reasonably well prepared. Even in New York, with the arrival of the hospital ship Hope to the harbor, only a few patients were treated there.
This is sadly what many of us have suspected right from the beginning. Some of our politicians and ‘experts’ have a great deal to answer for. How can they sleep at night? If they are in any way decent, perhaps they don’t.
“How can they sleep at night?”
Psychopaths experience no remorse or pity.
“If they are in any way decent, perhaps they don’t”.
If they were in any way decent, they wouldn’t have reached the top under our system.
Herd Immunity?
Sent from my iPad
>
Nice one, Swedish doc! Problem is, it’s sane, it’s rational. Won’t do, I’m afraid.
The puritans have take over and they love it.
One good (ish) thing I’ve noticed is that the newspapers in the UK headed by the Guardian and the Independent (anyone remember when they were good newspapers?) have seemingly stopped minding Sweden’s business, willing the country to fail. And checking on twitter it’s much more difficult to find the screaming “Sweden, you don’t know what your doing.”
Any attacks are now very different in tone.
“Changing America
@ChangingAmerica
·15m
It might be tempting to think that Sweden had the right idea in how it handled the coronavirus. But the truth is much more complex.”
“Changing America analyzes the problem with holding up Sweden as an example.”
I think it will eventually be the young who bring us to our senses. They and the low paid are the ones who are most suffering economically as a result of this madness. There will be a breaking point.
And I predict that sometime in the future politicians will come out and say “We knew. But we didn’t know how to get out of the mess. I wish I’d had the courage to say ‘enough'”
I’m really pleased about masks though. There’s plenty to be found on the streets; I pick ’em up, wash ’em and sell ’em for 10p. I’m planning on becoming the first Mad Mask Millionaire.
If the Swedes had been keener to wear masks, their unimpressive deaths per million might have looked better.
Inexpensive, accessible device provides visual proof that masks block droplets
“We confirmed that when people speak, small droplets get expelled, so disease can be spread by talking, without coughing or sneezing,” Fischer said. “We could also see that some face coverings performed much better than others in blocking expelled particles.”
Notably, the researchers report, the best face coverings were N95 masks without valves—the hospital-grade coverings that are used by front-line health care workers. Surgical or polypropylene masks also performed well.
But hand-made cotton face coverings provided good coverage, eliminating a substantial amount of the spray from normal speech.
On the other hand, bandanas and neck fleeces such as balaclavas didn’t block the droplets much at all.
“If the Swedes had been keener to wear masks, their unimpressive deaths per million might have looked better.”
Martin, sorry, but that is nothing more than a belief. No reputable research exercise has been able to find any statistically significant evidence for the benefits of masks. The only way people know they might have been exposed to the deadliest virus in human history, is to get tested.
Martin,
I watched a medical video demonstration about masks which praised the N95, but said they are rated to be worn for 2.5 hours. They did not say if that was because they get saturated and no longer perform or if it is that people should not have their breathing blocked longer than that. N95s are difficult to wear. In 23 years as a nurse I only wore them on rare occasions that we have a patient who had or was ruling out for TB. I believe it is dangerous for the public to be encouraged to wear them because they restrict your oxygen more than the other masks.
And St. Thomas in Charleston, West Virginia is forcing its employees to wear two masks. How many masks do you think it would take till they can’t breathe at all?
peter downey: You won’t be the first, but I hope you get rich at it! Carpe diem!
Gor bless you, Gaz!
It is very heartening to hear the good news coming out of Sweden, after all the criticism it received for being one of the few countries to adopt what seemed to be a rational, sensible and proportionate approach to the COVID-19 outbreak. I agree with most of the points that the good Doctor makes, but I believe that he is missing one very important point: the role of Vitamin D in the apparent “herd immunity” now being observed.
I believe the trend in the new cases of COVID-19 and severity of illness is further evidence that COVID-19 is a seasonal illness, and the seasonality is dependent upon the Vitamin D status of the population. Sweden is at a higher latitude than the UK, so it is a bit later on in the year that Swedes can receive enough UVB from sunlight to raise their Vitamin D levels from their Winter lows. It must have taken until the end of June before enough of the population reached protective levels of Vitamin D to achieve “herd immunity”.
Although the current trend seems to vindicate the Swedish approach to dealing with COVID-19, Sweden must beware the possibility of a second wave in the Winter, when the Vitamin D levels across the general population will fall, unless the public is made aware of the need to top up with dietary Vitamin D or supplementation. If a large percentage of the population becomes Vitamin D deficient or insufficient, herd immunity will be lost and the most at risk groups – the elderly and Somali-born citizens – will be the hardest hit again with serious illness and death.
If vitamin D from sunshine was a reasonable prevention then we would not be seeing such high numbers in Florida, Texas, Mexico and Brazil where normal attire has lots of skin showing.
… most likely smothered in sunscreen and so preventing Vitamin D synthesis
Hi Ann/Mike: Apparently D3 from sunshine is stored mainly in fat cells. Liver and kidneys convert the D3 into active form. Could be that obesity coupled with metabolic dysfunction prevents release of D3 from fat cells. Adipose tissue does more than just storing fat.
Mike Price, there are many reasons why vitamin D levels are low everywhere:-
https://vitamindwiki.com/tiki-index-php?page_id=11523
That list also doesn’t mention factors such as obesity and darker skin tones.
High numbers of what? Cases (possibly without symptoms, so healthy people with dodgy test results) or deaths?
Vitamin D status is complex. For example, I live in Adelaide, Australia, a sunny country. But I seldom get direct sun exposure. Being of Irish descent, I have very pale skin, and had some very severe sunburns after I arrived here as a kid from the UK in 1970. In the years after we were warned of the risk of skin cancer due to sun exposure. I’m outside regularly walking, but always covered up, wearing a hat and sunscreen. Now I’m careful to take vitamin D and C supplements, as I was regularly prone to respiratory ailments. Interesting that children too might not get much sun exposure as they’re pressed to cover up and wear hats when outside at school. And of course elderly people in aged care facilities might not see the sun often, and might be more inclined to cover-up – are they taking vitamin D supplements? We should have more independent and objective research on vitamin D. However, it seems a lot of the dollars are being gobbled up in the ‘race for the vaccine’ that is being led by Bill Gates…
Mike Price, high numbers of what? You might expect high numbers of cases, if you do lots of tests. When the tests are unreliable, what does this tell you? Nothing of use.
Mike Price: High numbers of what? We do know that in Florida the reported numbers are largely fraudulent. Show us the data which says that excess deaths in these four places are above what would normally be expected. We also know that, according to the CDC, in the months of April and May SIDS deaths dropped 30%, as concerned parents kept their precious infants out of the hands of the pediatricians. Bit of a silver lining to this nonsense.
Not necessarily true, darker complexions are less able to create vitamin D from sunlight. Also around the equator daylight is approximately 12 hours all the year round. The trajectory for a viral infection is longer and shallower than in the higher latitudes, according to Hope-Simpson.
People in such areas tend to avoid sunshine because of the heat, and are also likely to deploy sun cream.
You might assume that the likes of Finland would have low vitamin d levels due to lack of sunshine but no. Quite the opposite. When the sun does shine, they get out in it and are also encouraged to take supplements.
Here in the UK we’re heading into the dregs of summer and by the end of September the vitamin d levels bolstered by sunshine will be depleting and we’ll see a major surge.
belinda@leeks.com.au
On Fri, 7 Aug. 2020, 8:32 pm Dr. Malcolm Kendrick, wrote:
> Dr. Malcolm Kendrick posted: “7th August 2020 A doctor working in Sweden > as an emergency care physician contacted me to discuss all things COVID-19. > He has also written a blog, which can be seen here. I asked if I could > reproduce it on my blog as I felt it was a fascinating pers” >
Thanks Malcolm, I have shared this on Facebook.
Kind regards Nic, Sydney
On Fri, 7 Aug 2020 at 20:32, Dr. Malcolm Kendrick wrote:
> > > > > > > Dr. Malcolm Kendrick posted: “7th August 2020 > > > > A doctor working in Sweden as an emergency care physician contacted me to > discuss all things COVID-19. He has also written a blog, which can be seen > here. > > > > I asked if I could reproduce it on my blog as I felt it was a fascinating > pers” > > > >
Yo U-Who Lulu, Thought you might find this short essay about Covid interesting!
On Fri, Aug 7, 2020 at 3:32 AM Dr. Malcolm Kendrick wrote:
> Dr. Malcolm Kendrick posted: “7th August 2020 A doctor working in Sweden > as an emergency care physician contacted me to discuss all things COVID-19. > He has also written a blog, which can be seen here. I asked if I could > reproduce it on my blog as I felt it was a fascinating pers” >
Thank you Dr Rushworth for the article and Dr Kendrick for publishing it on his blog.
I think a key point is ‘hidden’ in plain sight near the very end of the article: ‘If only 6000 are dead out of five million infected, that works out to a case fatality rate of 0.12 percent, roughly the same as regular old influenza, which no-one is the least bit frightened of, and which we don’t shut down our societies for.’
No-one is the least bit frightened of influenza. People should be – it’s a killer. We make (or should make) strenuous efforts to keep it out of our elderly care homes each year. Sometimes we don’t succeed in this.
Yes, influenza is a killer, but we don’t find it necessary to destroy our economy to prevent it or kill thousands of other people from CVD, cancer, etc – nor should we. Decent treatment is what we need and it seems to be something the NHS is bad at. Polypharmacy for the elderly, lack of sunlight and fresh air and mental/social stimulation, and poor diets don’t help with either flu or cv19
The whole Covid-19 issue has been thoroughly bedevilled from the start by discussions about poorly-defined terms.
Mike C observes that inluenza “is a killer”. Yes indeed – for elderly and ailing people, who have been dreadfully let down by the government, the NHS, and some care homes.
But Dr Kendrick is – obviously, knowing whereof he speaks – right in the broader case. As I keep seeing recently, for healthy people under 45 dying from Covid-19 is less likely than being struck by lightning.
So for the population as a whole, Covid-19 has no more impact and causes no more deaths than “regular old influenza”. And that is really what government policy should focus on.
“But Dr Kendrick is – obviously, knowing whereof he speaks – right in the broader case”.
Apologies to all – it was Dr Rushworth who said that in the present article. However, as Dr Kendrick saw fit to reproduce the article with apparent approval, I hope that I have not misrepresented his view.
Hi Mike C: so many say this ” we should make strenuous efforts to keep it out of our elderly care homes each year.”
we can look earnest; emanate good intentions through every pore; look determined;
but what do we do please? Lock them all up; ban their carers from leaving the homes for the entire winter; make them resident? Stop all visitors? Lock each old person in their room all day for all the winter? (You can’t be too careful, you know!) Feed them through slots in the door; I keep thinking how I can raise the standards of care so we are seen to be showing enormously high standards of care; if these folks should die of a broken heart or isolation, then that is a small price to pay so they don’t die of flu surely?
Hi Terry, No. Certainly not lock them up. My mother died in a care home about three years ago and before that the highlight of her summer days was sitting in the garden chatting with friends and family.
I think we’re actually reading from the same page – but I may be trying to emphasise (perhaps poorly) a slightly different sub-plot.
Nasty bugs are not something the care homes can do much about – other than making sure that staff are fully aware and not penalised if they need to take time off for sickness. It’s certainly not something that government should try to address by regulation – except to make sure there is medical care capacity. What it means is that if you (personally) have a ‘flu you (personally) should use a bit of common sense and try not to spread it around – and especially not take it in to see your relatives if they live in care. The same is true of this damn bug which has been doing the rounds recently. It too is a killer – for some. Try not to catch it and if you do, try not to pass it on. If a nasty bug does get into a care home then the right thing to do is care for the poorly in hospitals – our recent NHS policy seemed to be the complete reverse of this.
People don’t want their elderly relatives exposed to nasty bugs: So if you’re feeling crook give the visit a miss this week – and maybe next week too. Your elderly relatives still won’t live forever, but it’s not up to you to speed them on their way.
By going for extreme lockdown we’ve ruined not just our own, but other countries’ economies – and that means people’s livelihoods. We call our employment ‘earning a living’ for a reason.
Although it is nasty (around as nasty as ‘flu) this damn bug is not Ebola. It is not an existential threat for the country. However, extreme lockdown is.
I’ve been struck by two extreme positions taken by media reports on elderly people’s deaths during this epidemic: On the one hand stories about evil people who ‘dump’ their elderly relatives in care homes where diseases can spread like wildfire. On the other hand poor multi-generation households where elderly relatives are exposed to bugs which the rest of the family can perhaps shrug off. We can’t have it both ways – though that does not make for a good media story.
Whipping up terror in the population? That sells column-inches (OK showing my age a bit too much there).
Really, how can people in aged care facilities be effectively protected from viruses? And there are lots of viruses… It’s my understanding flu vax started off for the elderly, and it isn’t effective and has been palmed off on everyone else, with it even being admitted that children are being flu vaccinated to supposedly protect the elderly, which I think is wrong.
And if infected people are moved to hospitals, how do you treat people with infectious diseases in mainstream hospitals? How do the logistics of that work in preventing spread throughout the hospital (and aged care homes)?
How is Sweden handling things in aged care homes now? I wish they would share some advice because it’s a shambles in Australia, particularly Victoria. How do you protect the elderly without cutting them off from the world? And this ‘protecting the elderly’ is such an abstract idea, when thinking of the practicalities of dealing with people who may have dementia and other serious health issues. And perhaps it’s difficult to get staff for aged care homes? I don’t think it would be an easy job…
There’s been 352 deaths over the past six months in Australia attributed to Covid…352 deaths in a population of 25.5 million… Many of these in the elderly who have lived beyond life expectancy.
At the risk of appearing callous…I’m struggling with the shock and horror being expressed in the media about people over 80 and 90 dying, supposedly of Covid. They’re even reporting deaths of people in their ‘100s’. Is it reasonable to get hysterical about people dying at this age? It seems there’s an expectation of eternal life now?
And despite all the keening and wailing, millions of elderly people remain alive…
Consider this ABS information: “Over the 20 years between 1999 and 2019, the proportion of the population aged 65 years and over increased from 12.3% to 15.9%. This group is projected to increase more rapidly over the next decade, as further cohorts of baby boomers (those born between the years 1946 and 1964) turn 65.”
I’m finding it difficult to understand what is going on, the over-the-top response to this virus, at the expense of the majority of the population, seems to be grossly disproportionate to the risk, and yet so many seem to be buying into this caper, it’s really bizarre…
elizabethhart: How right you are. Shocking and frightening how many people in this world behave like sheep. In California all the stores have become mask Nazis, except Walmart. They reversed their mask Nazi policy due to public pressure. Not my favorite place to shop, but I’ll be shopping there, as I’d rather not starve to death.
For those who haven’t seen it. http://Www.lockdownsceptics.org.
Why don’t children, particularly pre schoolers, become very unwell? By all accounts they should do as their adaptive immune system is itself immature, depending primarily on the innate immune system instead.
I recall seeing a number of expert doctors and scientists suggest that it is precisely the innate system that knocks back Covid in most cases.
“depending primarily on the innate immune system instead.” as everyone should;
Vit D Up-regulates the innate; and Down-regulates the adapative; (cytokines and antibodies)
so get some sun; take some Vit D; rely on the innate for resistance; keep invaders out.
Absolutely
Higher levels of melatonin may help.
If you scale up by a factor of 6.5 the Uk and Sweden’s Covid deaths are not dissimilar. (The UK’s numbers are being investigated, have they been exagerated?)
Uk 66 million population 46000 deaths – Sweden 10 million 6000 deaths
The UK locked down and there’s no denying that that has been economically appalling.
BUT, as others have said, the dust hasn’t settled yet so drawing conclusions is premature.
In addition, are the following differences between the countries relevant?
Sweden has 25 people per sq km the UK has 275
There is a very different ethnic mix. I believe the UK has a high proportion of vulnerable people.
Is the Swedish population healthier generally than the UK’s?
OF the European countries, Sweden has one of the higher rates of migrant / refugee intake from Africa, people particularly at risk of inadequate sunlight-generated Vitamin D. These in turn are over-represented in their COVID mortality.
I was going to say something very similar Jeremy. Ths is interesting and for the longer term encouraging but I don’t see how we can draw conclusions on the Swedish data in relation to the UK without a far better understanding of the demographics and also of any differences in areas such as healthcare, the provision of PPE and even cultural differences which might affect the spread of disease.
Stockholm is densely populated. I don’t think people per square mile is meaningful overall because if the cities are where most people live then the fact that there are large empty areas doesn’t matter much.
Just come across a wonderful example to show how the madness has gripped.
On Facebook, there was an article from The Guardian:
https://www.theguardian.com/us-news/2020/aug/07/south-dakota-bikers-rally-coronavirus-pandemic?utm_term=Autofeed&CMP=fb_us&utm_medium=Social&utm_source=Facebook&fbclid=IwAR27e3Ihq2pbjkkROax7TT5zBFP63d57aIoWw_BxiBam5H4dQkMQPrpWzz0#Echobox=1596831267
This received a lot of comments shocked at the behaviour of these people.
But these people (unless they’re sending in bus loads of people from care homes) will be relatively young or young and healthy. I believe the chances of having a covid death from this group are very small, certainly smaller than any of them dying from a road accident at this annual event in Sturgis. Of course! So, I googled and found this:
https://www.sonsofarthritis.com/blogs/news/history-sturgis-motorcycle-rally-wrecks-accidents-deaths
I posted this on Facebook. I expect to receive a number of LOLs and cute one liners in response.
I am 80 and would like to become naturally immune to covid-19. Supplementing with 5,000iu D3 and paying more attention to low carb, seed oils and visceral fat. Perhaps the current dietary guideline is the biggest risk factor.
It’s really interesting comparing one outcome with another isn’t it? Many clever thoughts. It would be so easy to spend all day thinking about it.
Changing the subject for a minute, as you seem a switched on bunch, can anyone tell me what a distraction burglary is please? I’ve tried looking it up on the internet but can’t find anything.
As I understand it, a person gains access to a house by saying for example, that he is fixing the water mains,and needs to test the occupant’s kitchen water supply. As the occupant leads the person into the kitchen, a second miscreant walks in and rifles the house.
This is correct. I used to know an elderly woman to whom this happened. When she caught wind of what was happening, she chased both miscreants out.
Thank you for the reply, Frederica, that makes sense.
I was in the garden yesterday topping up my vitamin D, watching the insects come and go, enjoying the flora. There was the most beautiful butterfly feasting on my busy lizzies, flitting about, it held my gaze for so long that I didn’t see a huge wasp land near my arm. The wasp was just about to pull off its sting when I noticed it and swatted it away.
I thought to myself I’m lucky these insects weren’t interested in the sandwich I’m eating or else I’d have to find a method of keeping them away.
Nothing but torrential rain today.
Slightly off topic. The region of England where I live was one of those least affected by the virus, even taking the official figures at face value. I work in an office in the local hospital. For over a month from June, once outpatients started coming into the hospital again for tests, we all had to wear surgical masks all day because we were seated less than six feet apart (now we are separated by plastic screens instead). No one is allowed to use fans because they blow germs around. There is no air-conditioning, so what it must be like on the wards I hate to think. Masks are obligatory in the (wide) corridors, and anywhere you don’t “belong”, and if you forget you are usually “challenged”.
And yet, a couple of weeks ago we were encouraged through official hospital channels to attend a local BLM protest.
Aileen, I was talking to an office worker in a private hospital in Cambridge. They are all forced to wear masks all day, and stay in separate rooms. Most of them have oral thrush.
Hi AH, it’s all just completely bonkers. I’m not surprised about the oral thrush. Makes you wonder how many dental problems will be caused.
My God, why? In England??? There is a world wide revolution afoot.
The totalitarians are coming.
The propaganda is so obvious. I cannot fathom how anyone doesn’t see it.
Anna, nor me, but most people don’t seem to. They tend to disappear very quickly if you say anything that goes remotely against the official narrative. I once used the word “obfuscation” (a bit irritably, I admit) during a staircase conversation with someone I usually get on well with; they just turned around abruptly and left. I’d think it was me reading too much into it, except that something similar has happened on a number of occasions. Goodness knows what people are reading and listening to (well, I can guess …). I suspect one or two might be sympathetic, but they aren’t going to admit it. Too dangerous, though I really can’t believe I’m saying that ☹️
Humorous and true cartoon of the real Bill Gates (3 min.):
The zealots run around screaming about “isolate” and “protect”
Here is an interesting tweet about a convent https://twitter.com/plaforscience/status/1292088277504266240 where 10 of 11 nuns tested positive for our chum, the rona.
One could say it calls into question the test and the religious zealotry of isolate to protect.
“The coronavirus has managed to enter a cloistered convent, that of the Brígidas de Lasarte-Oria, in which eleven of the twelve cloistered nuns who reside in it have tested positive for Covid-19. Fortunately, all of them are “asymptomatic”, according to what the mayor of this town, Agustín Valdivia, has informed EFE.”
So their priest must be a super spreader – isolate him!
No mention of what is called “Long Covid”.
New Zealand entered Alert Stage 4 lockdown on Thursday 26 March 2020.
We move back to Alert Stage 1 on Tuesday 2 June 2020.
We had 1,569 confirmed cases of Covid-19, and 22 deaths from Covid-19 as of today 9 Aug 2020. We have NO community infection.
New Zealand estimated resident population is provisionally 5,002,100 on 31 March 2020.
This is the information about confirmed and probable cases of COVID-19 in New Zealand.
https://bit.ly/3a7jxIB
You may draw your own conclusion from these numbers.
I, for one, am glad to live in New Zealand.
Back in panic stations now: New Zealand racing to track down the original source of the new coronavirus outbreak: https://www.abc.net.au/news/2020-08-13/new-zealand-racing-track-down-source-coronavirus-outbreak/12555718
I wonder if they are in panic again, or whether it is just the MSM doing it’s melodrama crap shoot.
elizabethhart: My question: Are any of these “cases” actually sick?
I must say, your blog is incredibly well written, in English, for someone who is Scottish.
Thankyou
I suspect there is a parallel between CV-19 testing and the efforts to detect super-low concentrations of pollutants in rivers, or even drinking water.
Just because we can detect extremely low concentrations of stuff, doesn’t mean these measurements are relevant.
Clearly a respiratory virus has to be breathed in before the immune system can get to work – however good it is. Thus testing people to see if they have the odd virus in their respiratory system may tell you nothing more than simply testing inert surfaces, or the air itself for virus particles.
Analogously, people look for incredibly tiny amounts of polluting chemicals, and correlate these measurements with disease, but often this involves trawling the data for correlations, which is always problematic.
In both cases we have not yet learned how to use such information intelligently – we make the measurements because we can.
I think that without PCR virus testing, the world would have handled CV-19 in a far more intelligent way.
Are we into Einstein territory here?
“Not everything that can be measured is important and, not everything that is important can be measured”.
Steve-R, your posts are usually pretty good. What is the point you are making? I assume there was one.
There is always a point Ah, but these days it often fails to survive the posting.
However…
We are able to measure single molecule levels of particles of dubious origin in healthy people and on the basis possible destroy their livelihoods by forcing them to quit working albeit temporarily – I think that this measuring is actually unimportant and should be stopped or highly restricted to people with symptoms (unrelated to oxygen depletion or CO2 toxicity due to mask wearing, or at the very least require a community nurse to check every 48 hours minimum for symptoms.
On the other hand we are unable to measure the ‘fear’ and ‘worry’ that will inevitably destroy lives by ‘causing’ stress and depression – also in essence immeasurable without brain biopsies (see e.g. Robert Sapolsky and Peter Gotzsche) – and suicides.
Steve-R, thanks for the explanation. The point you made about bout fear and worry is one of the most important aspects in my opinion. I goes further than many people think, I suspect. I was talking to someone who teaches the A level groups in a UK school. I asked how things were working out. Most of the work recently has been done on-line, and that was ok, as far as it went, but from the students point of view many were finding it “soul destroying”. I wonder if the idiot politicians understand this. I also heard for example in one school, all the school had to have maths taught in a single “bubble”. This means all of the age groups in the school, all at the same time. Another example of organised insanity which will be unmanageable. Thank Boris the Buffoon for not stopping it, and implementing something realistic.
CO2 toxicity due to masks – really?
Eric, depends if your happy with breathing CO2 at a concentration of 37,000ppm. This is not just some figure plucked from the internet, this is what I measured with a calibrated gas analyser.
I posted a little back of the envelope calculation below the CO2 video. You can measure that number pretty much everywhere in your airways while breathing out.
What counts is the volume of air trapped behind your mask vs. the volume you inhale, which is 1:10 to 1:30.
And another poster pointed out that the sensor will likely be cut off from fresh air during inhalation because the mask wraps around its openings. Those measurements are bad science for the gullible.
Apparently Covid is really bad for people in “care” homes. 50% of people over 85 reside in “care” homes. To predict your future look at your TG/GLUCOSE ratio and linoleic acid consumption for starters. This pandemic might be the “Keys Effect” when heart healthy butter was replaced by partially hydrogenated seed oil margarines, promotion of 0% fat foods, labelling meat and cholesterol as bad, and promoting consumption of grains. A vaccine will preserve the dietary status quo.
Only if it works.
“Clearly a respiratory virus has to be breathed in before the immune system can get to work”
Actually, no.
“Now, scientists at the University of KwaZulu-Natal have published a detailed reconstruction of how the virus spread from ward to ward and between patients, doctors, and nurses… on the whole, patients infected few other patients directly. Instead staff members spread the disease from patient to patient and from department to department—perhaps sometimes without becoming infected themselves. “We think in the main it’s likely to have been from [staff] hands and shared patient care items like thermometers, blood pressure cuffs, and stethoscopes,” says Richard Lessells, an infectious disease specialist at the KwaZulu-Natal Research Innovation and Sequencing Platform and one of the study leaders. He and the other authors found no evidence that aerosol transmission contributed to the outbreak.” — https://www.sciencemag.org/news/2020/05/study-tells-remarkable-story-about-covid-19-s-deadly-rampage-through-south-african
I would like to see a lot more information on exactly how people get infected. Why, for instance, do we sanitize and wash our hands if the virus is an aerosol? How does it get into us if it gets stuck to our hands?
Note also that infected surfaces can get that way from virus-containing droplets settling on them, something which masks will ameliorate somewhat, an aspect of mask wearing never mentioned or tested for AFAIK.
Martin
I have the same questions. Why did the cases perk up after a bit of relaxation, since I would have thought that prolonged semi isolation would have led to the virus running its course.
Here’s a recap of my questions
My son caught it, his wife and children didn’t
What is the mask position, useful or not, no pileons please
Flu vaccine, kills you or not in the presence of Covid 19
The most dangerous viral infection in the history or humanity, justification please.
Perhaps cases didn’t really rise after some relaxation, but more tests were done, therefore finding more “cases”, some of which will be real and some false.
Very Interesting Martin!
Here is some more food for thought:
In Rancourt’s paper that I have posted before, he examines randomized controlled trials with verified outcomes and concludes that respiratory viruses are primarily transmitted by aerosols, and not objects, surfaces, or touching the face etc. He also shows how aerosols are not blocked by masks (cloth, surgical, or N95).
https://www.rcreader.com/commentary/masks-dont-work-covid-a-review-of-science-relevant-to-covide-19-social-policy
The CDC published a paper in May of 2020 that concludes that hand washing, and environmental and surface cleaning don’t do any good to prevent the transmission of respiratory viruses. They say that these things can help with other pathogens, just not respiratory viruses. They also say “Our systematic review found no significant effect of face masks on transmission of laboratory-confirmed influenza.”
https://wwwnc.cdc.gov/eid/article/26/5/19-0994_article
Also, the WHO says that there is no direct evidence masks prevent respiratory viral infection. https://articles.mercola.com/sites/articles/archive/2020/08/03/no-direct-evidence-masks-prevent-viral-infection.aspx The fact that masks do not prevent respiratory virus transmission makes a strong case in my mind that aerosol are more likely responsible.
I envision aerosols as fine mist particles that are breathed deeply into the lungs, while respiratory droplets get stuck before reaching deep into the lungs, which can explain why masks block respiratory droplets, but don’t stop people from getting sick with viruses. My own personal experience is that I have noticed several times after going to the gym I have felt like I picked up a virus, even though I washed my hands thoroughly several times and and was very careful not to touch anywhere on my body. I also was not in close proximity to anyone or notice anybody coughing or sneezing, which makes me believe more in aerosol transmission.
I wonder if the authors of the study you posted avoided the aerosol transmission route because it is politically unpopular and would negate the push for mandatory masks? The public health narrative is carefully crafted to instill as much terror in the populace as possible, and mandatory masks pave the way for mandatory vaccines. Now that we know there are very effective and simple preventions and treatments with near 100% success, no one needs to be afraid of this virus anymore.
“I would like to see a lot more information on exactly how people get infected.”
Yes. The great unanswered question about COVID-19 is, How is it transmitted? You can find support in literature — and people have posted examples of it on this blog — for almost any manner of transmission.
My own guess is, It is transmitted in a variety of ways, but ultimately transmission requires a susceptible target. And while the demographics suggest who might be most susceptible, we can’t reliably predict who will become sick and how sick they will become.
We have a long way to go before we really know enough to “control” or even manage a respiratory pandemic. Beware of strangers bearing easy answers.
You could have stopped at ‘Beware of strangers’.
We have been through this one already, in a previous post Martin: you have posted this before;
they couldn’t work out what happened; as so often happens with these “tracing” games;
“We think in the main it’s likely to have been from [staff] hands and shared patient care items like thermometers, blood pressure cuffs, and stethoscopes”
… that means: we don’t have a clue, but we need to say something so let’s blame the BP cuff. It can’t answer back.
Not that many in this crowd need convincing, but here’s an example of what’s wrong with the news media.
From UPI:
“Asymptomatic COVID-19 patients as contagious as those with symptoms”
“Aug. 6 (UPI) — People with confirmed COVID-19 who don’t have symptoms of the disease are as contagious as those with symptoms and may need to be isolated to prevent spread of the virus, according to a study published Thursday by JAMA Internal Medicine.”
So they talk about viral load, quote some data from the study, and leave the implication, you know, that lock-downs of asymptomatics may be necessary.
But, they ignore an important section from the study itself:
“Although the high viral load we observed in asymptomatic patients raises a distinct possibility of a risk for transmission, our study was not designed to determine this….It is important to note that detection of viral RNA does not equate infectious virus being present and transmissible. For a better understanding of the viral shedding and potential transmissibility of asymptomatic infection, large rigorous epidemiologic and experimental studies are needed.”
CYA disclaimer? Maybe. But UPI at least ought to report that the study team hedged its bets.
I suppose hedging doesn’t earn eyeballs or click, does it?
Is it possible that earlier regular influenza can build up immunity for even covid? Would then regular vaccination make the immune system stronger or weaker regarding covid?
Håkan, there are problems with vaccines, and there are plenty with the flu vaccine. No vccine has ever proved to be “safe and effective” using a RCT. Flu vaccines fare as badly as others in their efficacy, despite the manufacturers claims. You don’t need vaccines to have immunity, and having the vaccine does not mean you will be immune.John Bergman on youtube has videos on flu jabs. It might be worth a look.
Malcom here is an another medical doctor’s opinion.This time from Melbourne in Victoria, Australia.
( I wonder if anyone here has been keeping up with the situation in Melbourne ? It is now under a stage 4 lock down after getting up to 750 infections per day.)
This Australian doctor working in one of the A & E dpts. set up for Covid patients in Melbourne, has a very different opinion to yours and the Swedish doctor.
https://www.abc.net.au/news/2020-07-17/coronavirus-melbourne-doctor-suppression-or-elimination/12462518
Hi Bill;
everyone is confusing “cases” with people being unwell; this test is meant to find tiny particles of virus; the virus can be dead; you might still get a positive result; if the virus is killed in the nose, and the person is unaware, that is what used to happen.
When I see ABC, I am already clear it will be a screecher’s article: full of melodramatic language; hyping everything.
“after exposure to a presymptomatic colleague who caught COVID-19” …… so here is a well doctor; staying in a hotel for a couple of weeks, all expenses paid; after being close to another doctor; who also was asymptomatic; but the test for the latter was positive; this article is a month old; so both of them were asymptomatic; phew.
this is all getting very silly. “Each time this pandemic slips out of control”; the only thing getting out of control; is folks’ sense of balance.
The doctor in that article, Aaron Bloch, says: “As a frontline doctor in Victoria’s fight against the virus, my view is that the rate of health care worker infection is unsustainable.” https://www.abc.net.au/news/2020-07-17/coronavirus-melbourne-doctor-suppression-or-elimination/12462518
I don’t mean to be flippant about the risks healthcare workers might face with this virus, but are there stats on recovery rates for healthcare workers after the virus? Are they ok? Are they likely to be immune and return to work?
Also, Dr Bloch says “Now is the time to reassess our strategy. To ask, do we open prematurely and risk this happening again? Or do we grit our teeth and lock down until we have eliminated the virus?”
So he’s calling for elimination – what does that actually mean? What does it entail? Lock down for how long? With what restrictions?
I read his article and couldn’t make heads or tails of it. What does he want?
It is SO refreshing to read about another way of approaching this disease. I believe we are denied open dialogue about alternatives in the US, all under the guise of “science” that reeks of politics and dogma.
I agree with you, Linda Halcon. Especially if we’re talking Dr. Fauci. Politics and dogma doesn’t begin to explain the way that guy bounces from one “theory” to the next on an almost daily basis. People are to a point where they don’t know what to believe anymore. I say avoid the damned face masks and get on with life. If you get sick, deal with it. The people where I live that are throwing the biggest fits of all are the people who are wearing masks!! It’s gotten to be a religion and I don’t like it one bit. I’m in my mid 60’s and I’ve never yet worn a mask. Thank God I live in a state where we have choices thanks to a gubner who isn’t afraid to speak her mind and listen to people. She also has the President’s ear, which never hurts either!
Thank you for this interesting article. If the doctor’s observation is right (some kind of herd immunity based on T-cell response) what is then the explanation for the huge differences in death rate per country? Metabolic health?
One reason is the variability in the way data on deaths is collected from one country to another. Some countries record only deaths that have been *caused* by the virus, others like ours seem happy to record anyone who dies after ever having tested positive as having died of COVID.
My husband and I have arrived on Jersey, Channel Island. We had to have the swab test on arrival. It hurt the back of our throats. All others we spoke to experienced the same pain even though there were many different operators. So the experience varies. I’m sure they were gentle with my very elderly mother in her care home.
We proved negative for current infection although we still suspect we had It over Christmas 2019.
We have made exemption cards for wearing face coverings. You don’t have to have a medical reason or medical approval to do this. Our particular reasons are 1. We wear hearing aids which could get dislodged and 2. Wearing a covering would cause us severe distress. People seem unaware of their rights (and ours!).
And anyway, what about all the breathing in of your own carbon dioxide! I think a few people taking alternative action encourages some others to behave less nonsensically. It was good to see some reasonable behaviour on the ferry.
https://www.gov.uk/government/publications/face-coverings-when-to-wear-one-and-how-to-make-your-own/face-coverings-when-to-wear-one-and-how-to-make-your-own
Actually Tish, You will discover that you don’t need an exemption card at all. I have been in many shops by now, and nobody (staff of other customers) has said a word. Try it – just put your card out of site and see what (doesn’t) happen!
We are always told that these tests can’t hurt us, but by now I am suspicious. Suppose for example, someone breathes in one or two viruses from the environment and then because of the test, some of these get pushed into the blood system, whereas otherwise the nose membranes would have dispatched them.
The mere fact that these tests have to be done this way suggests they are looking for something that may never multiply.
You are quite right David. Exemption cards are not necessary but may be helpful in asserting your wishes and rights on public transport. To use one elsewhere I would find too cap in hand and demeaning, it being our choice and right not to wear a face covering. Even so, the ferry people said their rules were more stringent than the UK government’s, it being a private concern!! But a chat with the boat’s manager enabled uncommon sense to be exercised – there were very few passengers and so it was hard not to be naturally distanced anyway. And quite ridiculous wearing a face covering on an open and pretty empty deck of a large boat, though some did. Very healthy!
Since we think that face coverings, social distancing and excessive hand washing, etc., could interfere with natural immunity of any bugs doing the rounds before the winter, wearing face coverings would infuriate us and cause us “severe distress”! Perhaps not the severe distress the gov envisages but severe distress nonetheless. Our rights eroded, our beings controlled – intolerable. Having to have a swab was bad enough. That’s where we draw the line.
Ok, so Sebastian’s theory is that Sweden has nearly achieved herd immunity. How is it then that new infections are still increasing in Sweden, by 33% compared to the week before? And in Spain, Italy and the UK, all of which had roughly the same deaths / capita as Sweden and by his math should also have achieved herd immunity, they are increasing, too.
Here are the current numbers, as average new infections and deaths over the last 7 days and change rate. Very roughly, the UK, France, Spain, Italy have the same number of inhabitants, Sweden 1/6 of these countries, and Germany 4/3.
https://www.spiegel.de/wissenschaft/medizin/coronavirus-infizierte-genesene-tote-alle-live-daten-a-242d71d5-554b-47b6-969a-cd920e8821f1
France 1400 10 +36%
Germany 877 7 +33%
UK 900 53 +18%
Spain 3700 unknown +60%
Italy 360 7 +28%
Sweden 270 4 +33%
Fortunately, the number of deaths are down pretty much everywhere. UK is still a little worse than Sweden per capita.
Why do we have this huge increase even in Southern Europe, where people should be getting plenty of Vitamin D right now, and many have had the disease? Why are Italy and Spain so different?
Birmingham ED doctor Dr Ron Daniels explains in a video on Twitter that despite the rise in cases, they aren’t serious enough to be admitted to hospital, are mostly in younger age groups with very mild or no symptoms, and are just clustering in areas that weren’t originally affected badly. His theory is that as herd immunity is reached, the places that weren’t exposed to the virus as a result of lockdown will inevitably start to show increased ‘cases’ but that it isn’t something we need to worry about necessarily.
Just measuring ‘positive cases’ doesn’t mean much unless they prove to be serious enough to be admitted to hospital, plus the regular reports we’re seeing of the actual PCR test kits being withdrawn for various reasons (contaminated, faulty etc) makes the testing process seem even more suspect. Also Professor Carl Heneghan of Oxford University has been very vocal about explaining why the number of false positives will increase as the virus diminishes due to the nature of the test.
If asymptomatic or mild cases are discovered by increased testing (ie not testing people because they have symptoms, but using the ‘Track and Trace’ system to find ‘Covid contacts’) it’s likely because they DO have good levels of vitamin D etc and that the body is actually doing a very good job of dealing with the infection – and increasing ‘herd immunity’ levels.
https://www.thetimes.co.uk/article/covid-wards-empty-as-virus-death-toll-plunges-bvm0mxl2n
Dr. Daniels raises valid points, but he is wrong on the state of North-Rhine-Westfalia. That state was the site of the first large outbreak within Germany, after an infected couple visited a Carnival festifal. And looking at the new infections on a county basis, it is still the Western counties that have the most new infections, even if a few of the Eastern counties are also showing an uptick n cases.
https://www.spiegel.de/wissenschaft/medizin/coronavirus-infizierte-genesene-tote-alle-live-daten-a-242d71d5-554b-47b6-969a-cd920e8821f1
You can’t know what the numbers of cases are doing when you use unreliable tests.
You use maths to give you a bounded estimate given the error margin of the tests.
Probably because the rt-PCR test sucks. Being “infected” really isn’t important if you aren’t ill. The test could be picking up old infections, including colds and similar flu-like illnesses or perhaps the so-called “novel” virus is actually some RNA/DNA that many people have had for a long time, but no one had tested for previously. No one really seems to know how viruses spread and why some people get ill and others don’t.
KJE: The nose. Immune factors in the nose bar the door to the entry of pathogens. If they manage to enter, the adaptive immune system attacks. Good metabolic health, a healthy micro-biome, sunshine and fresh air, remaining active, and a sunny disposition keep us healthy. What have our governments done over the last thirty years or so? Told us to fill our bellies with cheaply-produced and nutrient-deficient carbohydrate pseudo-foods and toxic vegetable oils. Avoid the sun. Shove drugs into everyone at the earliest opportunity. Why anyone trusts what political leaders or government agencies say is a mystery to me. A miracle so many of us have survived this onslaught.
“How is it then that new infections are still increasing in Sweden, by 33% compared to the week before?”
Eric: you are confusing positive test results; to an uncertain test;
with people being unwell;
Let me explain: they are different. Quite different: We have an epidemic of “case-itis” at present; we have never screened for viruses, as we seem obsessed with doing over our little friend, the rona virus. We could test for parvoviruses; rhinoviruses; adenoviruses; RSV; and so on and so. We could run around screeching at finding viruses that are causing us no problems.
If they have increased testing that is your answer. Here in the US, labs in Florida had an error in which nearly everyone tested positive. Also, the threat of opening the schools has suddenly resulted in nearly 100,000 children suddenly testing positive. Our teachers unions really don’t want to open. The protests have not resulted in any waves of infection, But Trump’s rally did. Reports all over from people who signed up for the test but gave up and went home, then getting letters that they are positive. And in California I heard they are going to pay people 1200 dollars if they test positive. What a bonanza! But the governor says California cannot afford to pay the extra unemployment. We have a lot of politicians that I hope find themselves needing a new career.
I would never volunteer for a test unless I was experiencing symptoms. My trust in this process has reached rock bottom.
I cross my fingers that Trump gets back – primarily for World peace – but I also hope he will set up an inquiry into COVID to get at the truth – rather as Epstein’s activities, and the “Russia hoax” are being exposed.
I would never volunteer for a test. If I was threatened with a test, that is assault, as I would feel threatened. If I was forced to take a test, that is battery. That is a criminal offence.
The problem with your argument that
while a large number of people were
infected and only a small number died
is the lasting side effects of the Corona
infection, a number of people
who had the Corona don’t continue to
lead normal lives and curse the day
they were infected, a lockdown would
have spared these people from continuing
to suffer, if you were one of them what would say
Thank you, awaiting your reply
Prof Shraga Don,MDPhD
Surely you absolutely need to try to get a balanced approach to an ‘epidemic’ such as this one. While there is so much disruption from lockdown, people have not been treated for cancer or heart problems, children are missing out on school, businesses are going bust – all putting enormous stress into people’s lives, etc. Stress means illness.
Since none of the COVID statistics seem to have been gathered carefully – not even the death rate – I do wonder about these long term damage claims. Since the COVID cases are hugely peaked in people over 75, and possibly in those who already had medical problems, I can’t help wondering if the ongoing problems of COVID patients reflect their poor medical condition going into the disease.
What I know for certain is that as a 70-year-old, I would rather take a slightly greater risk and have had no lockdown, rather than what has actually happened here in Britain.
It looks like the coronavirus will be with us for a number of years at least, and may become a permanent feature of life on Earth. In other words, you will get exposed to the virus eventually.
By self-isolating, wearing masks, etc, you gain time before getting infected. If you are proactive, you can use that time to build up your general health and immune system via nutrition, supplements, sunlight, exercise etc. If you’re Elon Musk you might even manage to escape to Mars ;o)
If you are not proactive, you can hope that they develop better methods of treatment, better drugs, or even a vaccine. But the way the medical profession disagrees about a simple protocol like HCQ/zinc/antibiotic, it doesn’t look like we’ll ever get a cheap and effective treatment that is generally accepted.
Regarding a vaccine, the Covid “long-haulers” worry me. Since even mild infections can result in lasting after-effects, what does that imply about a vaccine? It seems to me that one is in danger of becoming a vaccine “long-hauler” if using a vaccine that hasn’t been tested for several years.
Another thing that needs sorting out is a test to determine who is naturally immune, and if infected whether and for how long one remains immune thereafter.
There is treatment that could also be a cure. It just require one or two doses at most. Has been proven in vitro with one dose kill the virus in 48hrs and in a hospital setting in very critical patients were it reduces mortality. But is a cheap drug with decades of use with a proven record to work with relative safety for a host of conditions. But as it will negate the narrative for the panic and the control you will not hear much about it. But thinks that don’t work like respirators and expensive drugs are tooted as vital, while we wait for the salvation the vaccine.
US Trial Finds Drug Cuts Coronavirus Mortality 40%
https://www.newsmax.com/us/ivermectin-covid/2020/06/09/id/971417/?oRef=mixi
The FDA-approved drug ivermectin inhibits the replication of SARS-CoV-2 in vitro
https://www.sciencedirect.com/science/article/pii/S0166354220302011
Not to mention there are countless of natural remedies, supplements, foods, lifestyles that are immune enhancing and antimicrobial.
Why would you use a known toxic chemical – I thought I remembered it from stories about its use in freeing farmed salmon of lice infestations – when you could used safer drugs?
Prof Shagra,
You make a valuable point. I think the question we need to ask is – what treatment did these people receive? The conventional treatment with ventilators, etc. is a nightmare and lasting adverse effects would not be unusual, assuming they survived the treatment!
Those that are treated properly don’t report lasting side effects that I am aware of. These treatments include HCQ + zinc + zithromax, and also the MATH+ Protocol and more. Also, HCQ + zinc is being used very successfully as a prophylactic in high risk people such as frontline healthcare workers. Vitamin D is a powerful preventive measure, as studies show the only people that died from COVID had low vitamin D levels, while those with high vitamin D levels don’t even get sick.
Vitamin D:
https://articles.mercola.com/sites/articles/archive/2020/07/09/optimal-vitamin-d-levels-for-coronavirus-crisis.aspx?cid_source=dnl&cid_medium=email&cid_content=art1HL&cid=20200709Z1&mid=healthrtlucm20200709z1&rid=912432641
HCQ + zinc:
https://www.newsweek.com/key-defeating-covid-19-already-exists-we-need-start-using-it-opinion-1519535
MATH+ Protocol:
https://covid19criticalcare.com/treatment-protocol/
Prof Shraga Don,
Your concern for the suffering of a minority of COVID patients is honorable and touching.
I am not a fan — and there are few such fans on this blog — of imposing harsh suffering on the less-impacted majority of COVID patients — and those not impacted at all — in order to spare the suffering of a small and vulnerable minority. Those people should be protected if possible. But if the cost of protecting them is disastrous for the majority, it is immoral to do so.
The young and middle-aged families who cannot work have also suffered and will also suffer long-term consequences of lockdown. The people denied medical treatment have suffered and will suffer long-term consequences of lockdown, including sometimes, the risk of premature death. They, too, will curse the coming of COVID. This is not a matter of giving up a vacation or two or a few “toys” for the benefit of others. It may be the difference between a reasonably secure economic future — with all the attendant broad social benefits a strong economy provides — and living out life in perpetual economic and medical uncertainty..
The terrible effects of the lockdowns have been widely documented and discussed. They are as bad as chemotherapy and radiation for advanced cancer, barbaric treatments in use because The Powers That Be don’t have anything better. Maybe a hundred years from now, with greater knowledge, people will look back and wonder how we did this to ourselves.
Yes, your concern for the suffering of a minority of COVID patients is honorable and touching…but misguided.
Nice summary LA_Bob, we’re desperately in need of some sense of proportion on this issue. Society is being turned upside down by the response to this virus, it’s likely there’s also a larger and more sinister agenda going on.
come on Shagra: “is the lasting side effects of the Corona infection, ” …. I can’t find you on google; are you real? .. claiming an MD? This old bogey of “lasting effects” is continually churned out by the media: any illness; any traumatic injury; can leave folks with problems; the flu can leave folks debilitated; glandular fever is famous for leaving some with long-term tiredness; on its side, is that no-one believes they can keep it away by house-arrest or wearing things on their faces.
I cant find him either
Come on doc prove you exist
I never did believe he was a doctor because I haven’t seen one who talks that way.
Mr Chris and anna m: You can find him on LinkedIn and see where he is now and has worked previously, if you want to check him out with those employers…
dear mr shraga, we don’t know if anybody died of infection with “the coronavirus” because there are no validated test. Even if you believe that this virus exist (I don’t), you cannot assume anybody was actually infected, because the tests do not have any significance.
If I would find this fact out, and then know that I have been wrongly diagnosed and wrongly treated with toxic untested chemicals such as remdesivir, which is a dna chain terminater similar to AZT, (that has killed hundreds of thousands of AIDS patients), then I would probably ask somebody to tie me up to prevent myself from physically harming the doctor that did this to me.
Bart,
If the virus doesn’t exist, then what are the little yellow thingies in the image in this article? (Yes I know virus particles are not really yellow. They have been artificially coloured to highlight them.)
https://www.smh.com.au/national/scientists-discover-many-people-unexposed-to-coronavirus-have-immune-cells-for-covid-19-20200818-p55mw2.html
If viruses didn’t exist you would have to invent them to explain the virus-like infectious behavior. Are you saying only the Covid virus doesn’t exist, or are you denying there is such a thing as a virus?
From Sunday 29 March, public gatherings and events may have a maximum of 50 participants In Sweden
Is that a policy relaxation or an additional restriction?
Something else seems to be different in Sweden. And this is not an attempt at irony! I’m just trying to figure out what is going on.
There seem to be almost no cases in schools, with the exception of one school that had an exchange with Italy. This is in contrast to findings in other countries.
Also, the number of kids and adolescents per capita is almost the same in Sweden and in Finland, but Finland had a much lower total number of covid cases and closed its schools for nearly two months:
https://www.zeit.de/gesellschaft/schule/2020-08/corona-sonderweg-schweden-schulen-offen-virusuebertragung-kinder/komplettansicht
In reply to Tom Welsh comment Aug. 9, 2020 9:07. (No reply options, neither comment nor email)
The informed counsel you refer to including the solid Dr Kendrick who we all lay claim to and whose research and advice is not contaminated by mal influencing capital, do not that I’m aware, orchestrate conferences where a whiff of serious money and privilege permeates the stage with the promise of excess, intoxicating, pointing with more than just a nod to the stock market and the lucrative lucre that’s just a few accelerating share prices away all combined with bonding of the bountiful in to the wee small hours, the dizzy little Davoses where the drinks are free and relationships of all sorts develop & mature and mutual back scratching is in everyone’s interest. No – quite sober and boring actually, bonding is not lubricated but the work falls under the radar basically cos no big bucks are teasing anybody. The message, clean and honest doesnt attract media, is it because of a dearth of showboating or marketing?. But do I notice the Telegraph headlining with stuff that had appeared on these pages just a few days prior?
Maybe, maybe not but we live in hope. Yes yes we do – despite the juggernaut of fear & BS.
The Daily Telegraph exposes more of the issues than most, and it does not censor reasonable comments. I’d advise everyone here to switch to the DT – at least while this crisis continues.
Hi Jerome! I think I agree with you, although I’m still working out your comment. It’s nice to have poetry in a blog for a change… 😎
Dear Dr Kendrick
I saw this great article on twitter but a few had commented that he is a fake as not much online presence other than his blogpost so I’ve resisted sharing it.
Can you confirm that he is a practicing doctor?
Also how do you think this whole thing is going to end? My mental health is really suffering with each passing day and more ridiculous measures
Regards
Leila
Sent from my iPhone
>
I wouldn’t expect many ordinary doctors (unless they are selling something or trying to be TV celebs) to have much online presence – they’d be too busy doing their jobs. I’ve never seen a single GP from my practice online – doesn’t mean they aren’t, but I’ve never seen them nor would I expect to.
And here is a nurse’s perspective. She works in a major hospital in Richmond in Melbourne, Victoria. It is not pretty folks. https://www.news.com.au/lifestyle/health/health-problems/coronavirus-victoria-icu-nurse-kelsey-daviss-desperate-plea/news-story/3ab8ea767e4ba286b43c6c1db7c978ee
Billinoz, there may be some truth in that article, but it is littered with statements such as “Ms Davis has watched the highly contagious virus tear through people of all ages and from all walks of life. This should raise demands for an investigation, not a feed from a MSM news outlet which are Known for sensational stories rather than sober fact.
Re the nurse’s perspective you provide, “ICU nurse Kelsey David’s desperate plea”.
Ms Davis says: “I’ve cared for patients with COVID-19, male and female, from people in their 30s to those in their 80s,” she wrote. “Some with lots of comorbidities, some with none. Fit and healthy. “COVID-19 doesn’t discriminate.”
That sounds quite dramatic and alarming for people of all ages.
Looking at the current statistics on the Australian Government’s Department of Health website, there have been no deaths in individuals under 30. Two deaths are currently reported in each of the age groups 30-39 and 40-49. Nine deaths in the age group 50-59. 21 deaths in the age group 60-69. The rest of the deaths, 311, are in individuals over 70, most of these being over 80. That’s in a population of 25.5 million. (Note: There’s a discrepancy in the figures on the government website between the Total COVID-19 cases and deaths by states and territories table and the COVID-19 cases by age group and sex graph, but you get the gist. And the figures will change.) https://www.health.gov.au/news/health-alerts/novel-coronavirus-2019-ncov-health-alert/coronavirus-covid-19-current-situation-and-case-numbers
At this stage, I don’t think the fatality statistics fit with Ms Davis’s statement “COVID-19 doesn’t discriminate.”
It would be useful to have factual information on how well people of all ages recover after Covid.
More on nurse Kelsey David’s perspective, her ‘desperate plea’ and her suggestion that “COVID-19 doesn’t discriminate.”
That article was published on 11 August 2020 on the Murdoch-run News.com website.
On 10 August 2020, the Murdoch-run The Australian newspaper obligingly informed us that the Victorian government was launching a “confronting COVID ad campaign”.[1]
According to The Australian article “The Victorian government has launched an ad blitz highlighting the dangers of the coronavirus in a bid to bust myths surrounding the highly contagious disease. Unveiling the campaign on Monday morning, state Premier Daniel Andrews said the ads, which feature coronavirus survivors as well as healthcare workers, would run on ‘every platform conceivable’…Mr Andrews said the ad blitz was about drumming home the message that the coronavirus does not discriminate. “This is about trying to tell a story to as many Victorians as possible that this virus does not in any way discriminate between people based on age, based on their otherwise healthy status,” he said.” (My emphasis.)
The campaign seems very keen to portray the virus as being a threat to the young, e.g. “There have been two Victorians in their 30s to die from the coronavirus”.
We’re not told if these Victorians in their 30s had pre-existing health issues.
And there’s also the story of Sarah and Sam, two midwives who in the ads tell “of how they were ravaged by the disease”. We do seem to be hearing a bit about that now, it will be interesting to hear how widespread are these after effects.
Seems like the Victorian government is very keen to alarm the community about this virus with its ‘stories’, across all ages – is this justifiable and ethical?
Reference:
1. Victorian government launches confronting COVID ad campaign. The Australian, 10 August 2020. (This article may be behind a paywall.)
I have a hypothesis that I would like constructive criticism on, regarding SARS-COV-2.
The following are the axioms that form the basis of the hypothesis.
a) young children are least affected in the main
b) the elderly with comorbidities are most affected
c) younger people with comorbidities are also affected, particularly those that involve inflammation.
d) young children have a less mature adaptive immune system, depending more on the innate immune system.
My hypothesis is that the innate immune system is perfectly capable of disposing of the SARS-COV-2 virus through the pattern matching “primitive” immune response with minimal involvement of the adaptive immune system, which is why children, particularly those of infants school age, are less affected.
All of the nasty signs and symptoms of CoViD19 are as a result of the adaptive immune system going into inflammation overdrive, pneumonia, cardiovascular, abdominal pain and diarrhoea, and the Kawasaki type disease in some children.
Fever is an inflammatory response.
Maybe, the last thing we need is for the adaptive immune system to be triggered by a vaccine, who knows what it may unleash.
All of this is based on my understanding.
Hi JohnC; as many of us have come to read about resistance/immunity recently, I would agree with you; eating lots of carbohydrates and lots of wheat, appears to increase the inflammatory state. Ditching sugars and starches appears to help greatly to reduce inflammatory markers.
Terry Wright: Also vegetables (except in the concentrated form). Especially the cruciferous ones, and the nightshades. I feel so much better having ditched them all. Nuts, too. I think the harms outweigh the benefits. So I eat lots of vegetables in the concentrated form. Pork belly or steak and three eggs for breakfast, along with a bit of seafood. Steak for supper, sometimes with cheese. Organ meat (liver, heart and kidney) twice a week. I feel fabulous. No tests, but it is clear to me that I have reduced inflammation.
Hi Gary & Terry; another reason to avoid vegetables
https://www.independentsciencenews.org/health/regulators-discover-a-hidden-viral-gene-in-commercial-gmo-crops/
7 years old
Hi Jeremy: More recent stuff about edible vaccines that could be in your future. There could also be benefits in non GMO medicinal plants such as cannabis. Doing some personal research at the moment.
https://allianceforscience.cornell.edu/blog/2020/05/gmo-tomato-as-edible-covid-vaccine-mexican-scientists-work-to-make-it-a-reality/
Here’s a long but interesting read. Covers everything but Vitamin D, which some readers point out in the comment section.
My take is that if the immune system gets it right in the beginning or is tamped down early enough, it won’t get out of hand. So I would expect a vaccination to help because it helps the immune system make short work of the virus.
Hi John: Apparently innate and adaptive systems are highly integrated. My understanding is that reaction to SARS-COV-2 virus will depend on health of immune system. Vaccinating someone with a defective immune system could produce antibodies, but do nothing about preexisting conditions that could be more important to final outcome.
Can anyone offer any thoughts on this guy?
Leilla,
My hunch – for what it is worth – is that the whole thing will grind on until sometime in the winter, when people realise that the hospitals aren’t swamped with CV-19 patients because most of us have behaved in ‘risky’ ways and picked up weaker versions of the virus – or even full-strength versions that couldn’t fight our Vitamin D supplements – and everyone will be ready for the analysis of what went so horribly wrong.
Alternatively, after Nov 3 is past, the whole problem will fade away.
David Bailey: It’s not going to fade away. The Oligarchs have the public by the short hairs, and they’re not going to let go. We must fight these tyrants with tooth and nail till our dying breath.
Another gripe from me but this time about my poor 97 year old mother who is locked up in a UK residential home. She has extremely poor eyesight, hearing and short-term memory.
During the lockdown she developed a large squamous cell carcinoma on top of her hand. She has now been seen by a dermatologist and plastic surgeon and will have surgery for it. The problem is everyone has told her it is cancer and she is unable to distinguish a serious cancer from a less troublesome one. Cancer to her is one big thing. You might expect that with her impairments she would be happy to have her life ended, but no, she wants to go on and has become very upset.
Secondly, It seems that every time she meets a healthcare professional she is asked if she wants to be resuscitated. A CPR/DNAR form is already in place and that caused her anguish and nightmares at the time. But it doesn’t stop people asking what her wishes are. With her dreadful hearing and poor concentration she can’t understand and is convinced that everyone is wanting to “do me in”! She even wonders if her loving family is in on it. The residential home cleaned her room and she thinks they are getting ready for the next resident. What with lockdown and Mum’s impairments it seems impossible to set things right.
When we meet with a very elderly person for the first time it is easy to think they have more awareness and ability than they have. People need to spend time with them to recognise any shortcomings. Surely healthcare staff should be aware of this and be more sensitive when talking to the elderly.
It may be health-service-correct to tell everyone what is wrong with them but it would often be kinder to consult with relatives first. And it’s not just very old people who can feel threatened by conversations about resuscitations. Our 75 year old neighbour who had a heart attack and said he wanted to be resuscitated had pressure on him to revoke his decision. He was so distressed he put in a complaint.
How typical are these experiences I wonder?
Sweden reported over 4000 new covid-19 cases in July (worldometers.info), and yet Rushworth saw none of them in his Stockholm ER (which I don’t doubt). How could this be? Were the 4000 cases elsewhere in Sweden? Were some in Stockholm but did not cause symptoms requiring ER? etc.
It is quite simple really Richard; if you test people who are not complaining of any problems; but you still do a test; some of those tests will be positive: in a previous post, Dr K explained that if the incidence of the virus is perhaps 1:2500, nearly all the “positives” will be FALSE POSITIVES:
meaning each test has an inevitable FALSE POSITIVE rate; it will call some positive, when the person is NOT positive.
So from this you get cases: nearly all are asymptomatic; ie no complaints. A few might have a runny nose for a day, or a sore throat; but they do not need to trouble a hospital, which you say, is where Dr Rushworth works.
“Were some in Stockholm but did not cause symptoms requiring ER”; you have got it one there Richard; the vast majority of “cases” are asymptomatic; ie they feel fine; we could test for all sorts of viruses; in our craziness, we probably will; we will find viruses that live on us, that cause no problems: Richard, you are probably covered in viruses but you are fine; you could test positive for adenovirus, rhinovirus, parvovirus etc etc.
The world is going madder and madder and obsessing about nothing.
This is news to me that there are false positive PCR tests as a widespread problem. Sure, there can always be contaminated swabs and sloppy procedures, and the test will also pick up virus debris for same time after the infection has subsided, but other than these? Do you have any links?
Oxford University professor Carl Heneghan explains the issue of “false positives” here:
https://www.spectator.co.uk/article/how-many-covid-diagnoses-are-false-positives-
And more here about the PCR test – https://uncoverdc.com/2020/04/07/was-the-covid-19-test-meant-to-detect-a-virus/
Stockholm has already had the most infections in Sweden. Perhaps they have herd immunity there.But it is more likely that the new cases are nothing serious. Swedes love to get out in the sun in the summer.
Does anyone know what happens to a cell after it has been infected by a virus. I know it starts manufacturing the virus and pushing out copies, but for how long? How many copies does it make?
What makes a cell stop producing viruses? Does it die? If so, does it come to a natural end of life due to old age, or is there some deficiency due to the virus that causes it to die prematurely?
Can a virus instruct a cell to reproduce itself as well as copies of the virus, thus multiplying the virus’s production capacity? And, incidentally, potentially causing a cancer.
I believe infected cells produce molecules that tell white blood cells they are infected, and basically ask to be destroyed for the sake of the body. The Covid virus has a way of preventing this, apparently. Do other viruses have the same ability to suppress the calls for help?
Cancer does. And that may be how some cancers get a foothold.
anna m, Tom Seyfreid’s work suggests cancer is a metabolic disease and is the result of the mitochondria causing the cell function to go from respiration to fermentation mode.
AH,
Yes, I am familiar with his work. But I think he misses something. Why do the mitochondria become so sick? Cancer behaves like an infection. It takes over the cell, causes mutations in the nucleus too.
anna m, it’s something to do with nutrition I guess. Refined carbohydrates perhaps, but you’d need to ask Tom.
From what I understand it is that mitochondrial DNA does not have the repair mechanisms that cellular DNA has so any damage caused by toxins accumulates at a faster rate than it does in the cell nucleus – that and the higher rate of ‘duplication’ of mitochondria in cells as the numbers change in response to energy demand. There is also the effect of statins damaging the supply of ubiquinol required for healthy mitochondrial function – something recognised in the first statin patent application from Merck who intended combining CoQ10 in the statin pill, but never did.
AH
Nutrition may play a role in general health, carbs certainly decrease general health and perhaps stress the mitochondria. But this view of cancer is not much different than the current paradigm of a lightning bolt from heaven called mutation. I think that Seyfried is absolutely right and has nailed that it is the mitochondria which malfunction and not mutation, but there are a number of diseases which I think from my reading are going to ultimately have an infective cause. So it does not negate that various factors that we know contribute to cancer, including diabetes, do in fact contribute – they do it by rendering the cells more vulnerable to attack and infective microbes are of course opportunistic.
Reading this about the US in general and Florida in particular, I don’t get the impression that the virus has turned harmless:
Was this man offered HCQ + zinc (with near 100% success rate)? No.
Was he offered the MATH+ Protocol (also near 100% success rate)? No.
Was he taught about optimizing vitamin D levels? No.
Politics and greed are what killed this young man.
Wow, someone linked to an article by a weary nurse in Melbourne and she speaks of sedated patients dying on ventilators! I know a few may need that, but it seems Australia has learned nothing from watching the northern hemisphere for nearly half a year!
Everyone should view https://youtu.be/6RDffMCAujg to rationalise the thinking of lockdowns, their own as well as the thinking of others. References are available on tomwoods.com/lockdown
AhNotepad,
I think that is an excellent talk which puts our whole reaction to this virus into some perspective. I’d like to encourage others here to listen too.
https://www.bbc.co.uk/news/health-53741851 London v Stockholm
Sorry, BBC is as trustworthy as wikipedia on statins.
Dr. Rushworth might have a point in that hospitals may be seeing fewer infections, and this is happening elsewhere, too. Let me bore you once more with the link to live data for Germany (might take half a minute for all the graphs to load):
https://www.spiegel.de/wissenschaft/medizin/coronavirus-infizierte-genesene-tote-alle-live-daten-a-242d71d5-554b-47b6-969a-cd920e8821f1
Further down in that graph is a map of Germany with the new infections in the most recent 7 days per county. Then, after graphs of total infections and R-factor, there is another map with the ICU capacity per county.
Let’s take my county, a rural county in the South-West with about 300,000 inhabitants and four hospitals. It was hard hit in March because a local tour operator had several busses coming back from Ischgl in Austria. There was another flare up three weeks ago after a funeral in a mosque. New infections went to nearly 20 / 100,000 (7 days) but are back down to 5. ICU capacity is close to 70 beds (20 free), but only 1 CV19 patient, in ventilation (not sure if invasive). This might not be a straggler from April, because last week, there was one patient in ICU who was not being ventilated.
Let’s look at Ulm, also in the SW, city of 150,000 and home to a prestigious med school with teachng hospital (i.e. they get the difficult cases from the surrounding counties). The area was hard hit in March, there were verious flare-ups in surrounding counties, and right now, the city is quite high with 11 new infections / 100,000 / 1 week. 156 ICU beds, 58 free beds, two CV19 patients, out of which one in ventilation.
Then Berlin, 3.8 million inhabitants, currently at 11 / 100.00 / 1 week infections, was somewhat hit in March and had highish numbers throughout, with a recent uptick. One official was quoted saying that half of new infections are imported from abroad. 1278 ICU beds, 14 CV19 patients, 11 in ventilation.
Oldenburg, in the North-West, city of 150,000, regional center with specialist hospitals. Very low infections throughout the whole crisis, currently at 2 /100,000 / 1 week. Same thing for the surrounding counties it serves. Only recently have there been flare-ups in meat processing plants and agriculture, with some counties hitting 30. 158 ICU beds, 48 free, 0 CV19 patients in ICU! In the neighboring 10 counties, 4 of which had recent flare-ups and still have highish numbers, there is a total of 1 CV19 patient in ICU, but not being ventilated. There is no way this whole region can have build some immunity like Stockholm has. They were virtually Corona-free until July with very few deaths among the elderly. Still, practically no patients in ICU! So has the virus suddenly become benign, even when spreading in a previously almost unexposed population?
Same picture in France, which has about 2x the new infections compared to Germany and a faster growth rate:
https://www.gouvernement.fr/info-coronavirus/carte-et-donnees
We can only see hospitalizations by region, not by county, and there is no regional map of new infections. However, while we can only see ICU occupancy in Germany, we can see all hospitalizations in France!
Paris has about 2500 people currently hospitalized with CV19, the two regions bordering on Belgium and Luxembourg have about 500 each. Numbers in ICU are 187 (compare to 14 in Berlin), 45 and 17. The interesting part is the new admissions (which are probably by day and not week): 5 in Paris, a total of 8 in the rest of the country. Out of these, three new to ICU in Paris and none anywhere else.
So about 1800 new infections / day (7-day average) testing sick in France, but only 18 needing to go to hospital. This is truly puzzling.
Interestingly, the daily admissions are a lot higher today than they were yesterday: 133 in contental France vs 13 yesterday, 15 new ICU admissions vs. 3 yesterday. New infections are 2524, with the 7 day average now at 2000 vs. 1800 yesterday. Percentage of positive tests are also continously creeping up, currently at 2.3%.
Need to keep watching for daily changes.
Several cynics on other blogs are suggesting that the tests themselves are contaminated to ensure the fear level of positive tests is increased. There has to be some reason why the swabs are long enough to reach the cribriform plate that contains the nerve channels accessing the olfactory bulb!
There is no need to contaminate test kits in order to maintain a steady rate of positive results. As has been explained in many places, with the known failure rate of the PCR tests a level of at least 5% positive results would be expected even if no one at all had the virus. (Which, for all I know, may very well be the case).
The fewer people have the virus, the more unreliable the test becomes. I am sure the authorities are well aware of that.
Steve-R: There is a certain president who keeps saying “so I’ve heard” or “people think” to justify spreading falsehoods. Doing it again just now about Kamala Harris’ citizenship.
And those could be the words from the mouth of a certain UK PM, except he can’t assemble the words unless they were on a prompt card from a certain DC, “Hands Face Space” Ring any bells?
Tom, how do you explain the positive rate dipping as low as 1.0% in France and 0.6% in Germany if the false rate is really 5%? This is BS!
177 new hospitalizations in continental France this morning, 23 newly admitted to ICU. I am beginning to believe Wednesday’s figures were way off. Maybe because most of France does not work Wednesday afternoons?
Pick any three digits, put them in front of “new cases” and search.
After having established that surprisingly few patients are currently in ICU in Germany, and that only 1/1000 of the newly infected in France are hospitalized and even fewer admitted to intensive care, it would be interesting to see hospitalizations etc. for the US. I have not crunched the numbers, but they would seem to be way higher.
After thinking some more about this:
– Why are we not reading more that hospitalization rates have gone down almost everywhere as new infections are soaring?
Possible explanations (for the effect, not the lack of reporting):
– Virus has mutated to more infectious but less deadly. It would have to be the dominant strain in Europe as we seem these lower hospitalization pretty much everywhere. This hypothesis would be easy to check.
– More younger people infected. Yes, but surely not all old or co-morbid folks have had this bug.
– Maybe the virus is already endemic, and a large percentage have been exposed to low concentrations, so when they are exposed to a larger dose, they test positive, but their immune system does a much better job dealing with it.
I like the last explanation!
Eric,
I care only about hospitalizations. Testing produces positives. Some are false positives, as I hear the CDC admits a 3% false positive rate. It is also possible, since flu and colds are seasonal, that the infections are milder due to summertime conditions, mostly vitamin D levels.
As to lack of reporting on good news – well that seems to be the agenda.
Anna wrote:
“Some are false positives, as I hear the CDC admits a 3% false positive rate.”
I’d love to have a reference for that, because it would settle a scientific argument I have been having with a friend who insists the PCR test can’t produce false positives, or they wouldn’t use it for testing the well.
Even 3% is more than enough to explain all the scares that are causing fresh lockdowns now.
Some more numbers in yesterday’s bulletin from RKI, page 9:
https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Situationsberichte/2020-08-12-en.pdf?__blob=publicationFile
Positive rate was as low as 0.6% but is at 1.0% now. Number of test has also increased to about 700,000/week from 500,000 a few weeks ago. This number will contain repeat tests. If we ignore this and assume a 0.2% false positive rate, these extra tests will have resulted in 400 extra positives per week or 8 per day, clearly much less than the daily increase over the same time frame.
What may still be the case is more people having gone through an asymptomatic infection and the test picking up viral debris weeks later.
Sorry, 57 per day, still much less than the increase in new cases.
The facts are that the rtPCR test does not detect live virus so even positive tests do not confirm live infection or active Covid-19.
If your ‘friend’ cannot grasp this then he should stick to books with a comprehension level Age 3.
David,
Eric made a good point, if some countries report very low case rates, how can the 3% figure be correct? Unless they are lying in all directions! But your friend needs to read about the actual history of the test and that it is not designed for diagnostic purposes. We use it because we don’t have anything better, I presume.
I found the following from the CDC which admits to false positives but doesn’t give a percentage. However they do discuss the negative effects upon a person’s life fromgetting a false positive. And then I found a 3rd article which discusses that, and by the way, even the PCR test has more and less accurate ways of developing it to get the answer.
Click to access Factsheet-for-Healthcare-Providers-2019-nCoV.pdf
The CDC 2019-nCoV Real-Time RT-PCR Diagnostic
Panel has been designed to minimize the likelihood of
false positive test results. However, in the event of a
false positive result, risks to patients could include the
following: a recommendation for isolation of the patient,
monitoring of household or other close contacts for
symptoms, patient isolation that might limit contact with
family or friends and may increase contact with other
potentially COVID-19 patients, limits in the ability to
work, the delayed diagnosis and treatment for the true
infection causing the symptoms, unnecessary
prescription of a treatment or the…
Click to access Factsheet-for-Patients-2019-nCoV.pdf
What does it mean if I have a positive test result?
If you have a positive test result, it is very likely that you
have COVID-19. Therefore, it is also likely that you may
be placed in isolation to avoid spreading the virus to
others. There is a very small chance that this test can
give a positive result that is wrong (a false positive
result). Your healthcare provider will work with you to
determine how best to care for you based on the test
results, medical history, and your symptoms
And the 3rd article:
https://thehill.com/changing-america/well-being/prevention-cures/496651-false-positive-and-false-negative-coronavirus
Curtesy of the French governement, just click on the age labeled “indicateurs”:
https://www.gouvernement.fr/info-coronavirus/carte-et-donnees
Their positive rate nationwide, and while dealing with local outbreaks, was 1% in Mid-July. This is an upper bound for the false positive rate.
And this places the specificity of two commercial tests at 99.9%, so this would result in 0.2% max. false positives:
https://www.tagesschau.de/faktenfinder/corona-test-117.html
Still, surprisingly high, but nowhere near 3%. After a positive test, usually a second test is taken to confirm.
I wonder if it is possible that even false positives fluctuate. If the test gives a false positive there can be a number of reasons, such as a recent infection with something else, all of which goes down in the summer.
Here is an informal experiment with masks that I think is rather revealing. The video is in English, but the website is Czech.
https://www.zvedavec.org/vezkratce/17219/
The build-up of CO2 behind the mask is quite remarkable.
Clearly most people cope with a mask, but most people aren’t getting CV-19! These masks could easily do more harm than good.
David, that’ Del Bigtree and Son doing the video.
Um, am I supposed to know them – we have never been introduced!
Er, no…., but if you search for Del Bigtree and masks, or similar you will probably find references. Sometimes I don’t provide links as I get attacked for providing misinformation, so if people look it up themselves, they can select which seem the most accurate information.
https://en.wikipedia.org/wiki/Del_Bigtree
Charming fellow. Anti-vaccination activist and conspiracy theoreticist. Filmmaker.
Wikipedia, mmmm….., wasn’t that the outfit that deleted a certain Dr. M. Kendrick? Obviously a trustworthy organisation for a reference, not!
Anti-vaccination is a thoughtless insult, those labelled as such are simply demanding safe vaccines, you know, vaccines that have been properly tested against real placebos in double blinded placebo controlled trials, and then the side effects arising with longer time exposure carefully considered every 2 years as the law in the US required back in 1986 when Reagan gave in to the threats of the vaccine manufacturers and immunised them against any and all consequences arising out of faulty or – heaven forfend – ‘UNAVOIDABLY UNSAFE’ vaccines [NB not once has the biennial review taken place].
But then you probably knew this?
Steve,
yes I did. And I took care not to insult the gentleman.
Oh, no! Surely there are no conspiracies!
David,
Looks like you are right, masks do cause more harm than good. Look at what dentists are saying:
“We’re seeing inflammation in people’s gums that have been healthy forever, and cavities in people who have never had them before,” says Dr. Rob Ramondi, a dentist and co-founder of One Manhattan Dental. “About 50% of our patients are being impacted by this, [so] we decided to name it ‘mask mouth’ — after ‘meth mouth.’ ”
https://nypost.com/2020/08/05/mask-mouth-is-a-seriously-stinky-side-effect-of-wearing-masks/
They got cause and effect wrong. Masks became mandatory in public settings when distance could not be maintained April 15th, but businesses could still decide whether they required masks:
https://en.wikipedia.org/wiki/COVID-19_pandemic_in_New_York_City#Social_distancing_and_face_masks
That must be a super quick detoriation to become a significant and noticable phenomenon by early August. The mechanism given is that people with masks tend to breathe though their mouths, which I don’t believe for a minute.
Then one would expect that the average Joe does not have to wear a mask for most of the day, so it would be specific occupations like hairdressers having this problem predominantly, which the article does not mention. Also, surgeons, dentists, nurses, beauticians etc. would all have lost their teeth long before corona if the effect were this pronounced.
No, people notice their stinky breath under the mask and decide to do something about it. In all fairness, the artcle mentions this, but does not consider it significant.
Eric,
Have you actually not worn a mask? Of course you breathe through your mouth even if you normally breathe through the nose. It is much more difficult to breathe with a mask on and thus the mouth breathing. And many people are required to wear masks almost all day since this outbreak. Surgeons and dentists do not wear masks all day. Nurses wear them only rarely and for maybe 15 minutes at a time. I never heard of beauticians wearing masks on any regular basis. By the way a young girl told me she gets a sore throat by the end of the day. Probably using a cloth mask. They are worse for retaining heat and moisture.
It does annoy me that mask apologists cannot take in the fact that doing something this uncomfortable, and this unnatural, might actually have a downside. Why assume that something which makes most people immediately uncomfortable is without negative consequence? OSHA in the state of North Carolina has restrictions on wearing masks more than 4 hours per day. Also, there are O2 levels below which it is considered dangerous. If you are breathing in air with O2 levels below 19.5% that is considered unacceptable. I have seen articles saying that masks indeed go below this. Likewise levels of CO2 are apparently alarming.
I have come to believe that mask wearing is a filthy habit, like chewing snuff.
Anna, I spent many hours with a surgical mask on Saturday (weekly shopping, and a first in a while, art exhibition). At various intervals, I stopped to see how I was breathing, always through my nose. Hell, I’ve even on occasion forgotten to remove my mask after exiting a shop, and found myself cycling uphill with a mask.
Regarding wearing a mask all day, surgeons and dentists used to wear a mask for long stretches before Corona. Now, at least here in Germany, hairdressers, beauticians and many retail employees have to wear them for their full shifts. All I was saying was that we should have seen mask mouth before, and should now be seeing it first in those professions where extended mask wearing is required, but we aren’t. It simply isn’t plausible that mask wearing will be such a powerful agent of tooth degradation!
Well, Eric, I think you are in the minority if you find masks that comfortable. Many people do not. I wore them years ago when I was much younger and healthier and I always found them uncomfortable. Mask mouth isn’t only tooth decay, which is probably a bit unlikely. Gum disease? Maybe. But one young woman told me at the end of her shift she has a sore throat and this seems plausible to me. Surgeons may have worn them quite a bit, dentists only on and off, if that. Really, prolonged mask wearing, 40 hours per week, is new.
This is the recommended method for performing CPR during the current situation from St John Ambulance
https://www.sja.org.uk/get-advice/first-aid-advice/unresponsive-casualty/how-to-do-cpr-on-an-adult/
Note how the airway is kept clear by a piece of cloth over mouth and nose. Compressions only is normally sufficient, MTM isn’t necessary. There’s also an issue with registered healthcare professionals as they have a duty of care to treat within their competence under their codes of professional conduct, and basic life support is mandatory for all employees within a healthcare setting. We’ve been informed and I believe it came from the resuscitation council that CPR is not an aerosol generating procedure.
JohnC: When I was originally taught CPR (in the ’70’s), it consisted of both chest compression and rescue breathing. Seems to me in recent decades it has become chest compression only, long before the ‘Rona came along.
I’ve only been retired 2 years and my CPR classes always included rescue breathing!
My sister worked for the ambulance service, having retired a few years ago, and said that back then they no longer recommended mout-to-mouth, just chest compressions, for general resuscitation. May be different for medical staff if necessary, but the chest compressions only is the usual First Aid training.
David, seriously? Aren’t you a retired scientist? I can’t believe nobody’s stepped up to debunk this video!
The first number I came across (in a paper from a government lab about air quality in rooms) was that exhaled air contains 40,000 ppb of CO2. Of course, this is a ballpark and will depend on exertion and breathing frequency, but let’s stick with that number.
If the boy is exhaling 50% of the time and inhaling 50% of the time, the time average in the trapped volume is going to be 20,000 ppb. Nothing surprising here. And you can drive that number up be exhaling slowly and inhaling quickly. Frankly, it looked like he was doing anything but breathing regularly. And by the way, you are going to measure that same number if you place a time averaging sensor anywhere in the airways.
So how much of that ends up in the lungs? That depends on the volume of the air trapped behind the mask. If he switches instaneously between exhaling and inhaling, he is going to inhale maybe 0.1 l if we are generous. His breathing volume might be 1 l (he’s a big boy, and it is exciting to be in the studio), so he is going to get an average of 2000 ppm (well, maybe a little more, considering the studio was already at 850 ppm). Not a problem at all, and less so for a surgical mask (smaller volume, less sealing) or a cloth mask.
And it is seconded by everyday experience. I used to wear FFP2 and FFP3 masks (without a valve) long before corona for sanding or spray painting wood. Yes, I’d get sweaty, but never dizzy, even when exerting quite a bit.
The face has a higher volume, maybe 0.5 l and is more open, but I’m sure with the right breathing technique and when you stick the sensor into the path of the exhaled air, you can get a 2000 ppm reading.
It worries me a lot when I see seriously incorrect numbers being cited.
“…exhaled air contains 40,000 ppb of CO2”.
Assuming that “ppb” means “parts per billion”, 40,000 ppb means 40 parts per million, or 0.004%.
But the correct figure is about 4% – that is, 1,000 times more. See, for example,
https://www.biotopics.co.uk/humans/inhaledexhaled.html
https://sciencing.com/chemical-composition-exhaled-air-human-lungs-11795.html
Thank you, typo. I did my math with ppm, which is evident from the steps I described above.
Thanks Eric – that’s a relief!
David,
I just watched the video. It is completely wrong. There is essentially no CO2 buildup behind the mask. When Del’s son exhales, there is a positive pressure built up inside the mask, which pushes his breath over the sensor. When he inhales, there is a negative pressure inside the mask and the airflow does not go over the sensor as it is blocked by the fabric being pulled in on the sensor sides and also the plastic cap on the top of the sensor.
In addition, the volume of CO2 available to inhale is limited by the volume between the mask and the boy’s skin, which is very small.
While there is essentially no CO2 buildup, masks do have big problems, most notably of which is that they don’t work to prevent the transmission of the coronavirus.
Sensor they used – notice plastic cap over top:
https://www.gainexpress.com/products/co22
English version of video:
Eric and Dr John,
I did wonder about some your objections – which is why I described it as an ‘informal’ study, but there must be some sort of continuum between on the one hand, placing a plastic bag over the head(impeding the flow of fresh air completely) and breathing with nothing impeding fresh air flowing in. I agree the numbers aren’t meaningful.
Clearly the mask impedes the flow of fresh air, and the “mask mouth” observations by dentists tend to suggest that masks are a real health issue.
A nurse I know of in the UK had blood tests done after prolonged muzzle wearing, and the results were similar to those who had undergone high altitude training.
First of all, the word muzzle is somewhat biased.
Then, oxygen saturation can be measured with a pulse oxymeter, no need for blood tests.
Lastly, those who have undergone high altitude training would have higher oxygen saturation at sea level. Was that what her tests showed?
I may have been to quick to say this is totally wrong, though I do think we need to question those numbers.
Dr. John H, even if your words were a bit hasty, as a result, I thought about the measurements I made, and I will make some more using different methods and see if it shows a discrepancy, so thank you for the comment.
I posted on the mask mouth further below. By that reasoning, mask wearing seems to act on teeth and gums within a few weeks, so surgeons, dentists, some nurses should have lost their teeth long ago, way before corona, and we should be seeing hairdressers, cosmeticians, police and EMTs predominantly presenting with mask mouth. The evidence is where exactly?
Eric,
That is a fair point – but do we know if nurses and dentists do suffer more dental disease?
The problem is, the evidence in favour of wearing masks to stop the virus seems very weak, and nobody has formally researched what happens if people make a face covering out of more or less anything.
Also, people who are not in good condition are pulled in two directions. On the one hand they could excuse themselves from wearing the mask on medical grounds, on the other, those same people may feel the mask gives them protection.
i totally agree i am a visiting podiatrist with a large number of elderly patients all the government have suceeded in doing is frightening the bejasus out of them and eveeryone else who has not got a functioning brain it seems to me it is not face coverings they have got on but eye pads mind you as it is said there is none so blind as those who will not see gerald
The fatality rate is even lower, if you don’t go to a hospital where they put you on a ventilator.
https://www.thehindu.com/news/national/coronavirus-57-of-mumbai-slum-population-has-developed-antibodies-study/article32216939.ece
Most people died in rich countries and big cities. If almost nobody dies in an indian slum or in italian or greek refugee camps, the not the virus alone is deadly. It looks like it needs the help of doctors and ventilators.
The same virus kills 80-90% of all ventilated patients in the USA but only 20-25% in Germany?
In Madrid almost 9.000 people died. In a provisionally hospital only 17 of 4.000 patients died. So in this Hospital the Virus was less deadly?
This article is very interesting – though parts of it go over my head:
Click to access orient.pdf
It came from Henry Bauer:
https://scimedskeptic.wordpress.com/
David Bailey: “Malice is much less common than incompetence” says it all, and the need, as Dr. Kendrick reminds us, to do something, anything, is pervasive in medicine, when doing nothing at all is sometimes the best course to take.
Thanks David,
Got half way through. It confirms a lot of what has appeared here. This extract is of note ;
“In a pandemic, one would expect the all-cause mortality rate to increase. But for the first part of 2020 through Apr 5, the U.S. all-cause mortality was about 14.92/100,000, a multiyear low.” And confirmed time after time here- “One factor in the fear of COVID-19 could be gross overcounting of COVID-19 deaths.”
David Bailey: very good article. Thanks for posting it.
Psychopath Dr. Fauci has found another way to terrify the public and now recommends masks + goggles + face shield, with zero science to support his recommendation!
“Fauci is now also endorsing the wearing of masks during every influenza season going forward.”
“Guidelines for safer sex during the pandemic include wearing a mask, avoiding kissing, sticking to masturbation and having sex online, even though this means every encounter will be indefinitely stored and could end your career if hacked or shared.”
https://articles.mercola.com/sites/articles/archive/2020/08/12/do-you-need-goggles-for-coronavirus.aspx
Ivor Cummings has some facts regarding the evidence of testing falsifying the true rate of infection;
Nevermind, the vaccine will provide a final solution. It will be safe and effective, and all the safety studies will be done, and the vaccinated will fare better than the unvaccinated, studies on previous vaccines have shown. Er except the previous studies may not have been carried out.
Received today from the Informed Consent Action Network
On July 29, 2020, after months of false claims and objections, the CDC finally conceded that it could not find a single study comparing health outcomes between vaccinated and unvaccinated children and that it “has not conducted a study of health outcomes in vaccinated vs unvaccinated populations.”
Parents, doctors, and scientists have, for decades, demanded that the CDC compare the health outcomes between vaccinated and unvaccinated children. This is, in part, because as the increase in the CDC’s childhood vaccine schedule over the last 30 years from 8 vaccine injections to 50 vaccine injections (plus 2 injections during pregnancy) has occurred in lockstep with the increase in the rate of autoimmune, developmental and neurological disorders in children from 12.8% to 54%.
The demand for this study has grown so great that even the Institute of Medicine (IOM) in 2013 issued a report stating that the CDC could and should perform this study, explaining that it “is possible to make this comparison [between vaccinated and unvaccinated children] through analyses of patient information contained in large databases such as VSD [the Vaccine Safety Datalink paid for by the CDC].” Incredibly, the CDC then spent hundreds of thousands of taxpayer dollars to have scientist, such as Dr. Stanley Plotkin, write a white paper, published in 2015, on how to conduct this simple study.
To find out if this study recommended by the IOM 7 years ago has been done, our legal team, headed by Aaron Siri, submitted a FOIA request to the CDC on June 26, 2020 demanding: “All documents in the CDC’s possession which compare the health outcomes of children that have received vaccines with children that have never received any vaccines.” That same day the CDC sent a letter stating it had placed this request on a “complex processing queue” because the CDC’s office processing this request “expects to receive and review voluminous records in response to your request.”
The CDC then issued another letter on July 6, 2020, this time objecting to the request as “Broad” and “Vague” because it “lacks the specificity needed to assist the agency [to] retrieve the information with a reasonable amount of effort,” thereby again indicating there are so many studies it cannot possibly compile them all. Our legal team sidestepped the CDC’s objection by responding that the CDC need “only provide the first twenty journal articles the CDC can identify which are responsive to the request.”
Incredibly, the CDC responded on July 9, 2020 by making yet another objection stating: “Your request for ‘…the first twenty…’ is not sufficiently quantified to allow the agency to conduct a reasonable and adequate search.”
Our attorneys were now about to have even more fun with the CDC. On July 13, 2020, they responded to the CDC by stating: “To clarify, we are seeking any responsive journal articles up to a quantity of 20 articles. … We have [therefore] now limited the request to up to a maximum of 20 journal articles in the CDC’s possession which compare the health outcomes of children that have received vaccines with children that have never received any vaccines.” Our attorneys also resubmitted the original request again with slightly different wording to make sure the CDC had no escape hatch.
Well, by August 3, 2020, it appears that the CDC had had enough and knowing that we will sue them, as we have done in the past, they capitulated. Behold their response in which they concede in black and white that they had nothing:
A search of our records failed to reveal any documents pertaining to your request. The CDC has not conducted a study of health outcomes in vaccinated vs unvaccinated populations.
It is incredible that this simple study has not been published. Or maybe the CDC did conduct but not publish the study because it did not provide the results they wanted. Either way, the next time someone tells you that it is a “myth” or “hoax” to claim that the CDC has never conducted a vaccinated versus unvaccinated study, you can put this CDC response in their face.
The vaccines on the CDC’s childhood vaccine schedule given to babies during the first six months of life include over 3,500 mcg of aluminum adjuvant, a known neurotoxic substance which can damage nerves and kills cells.
The dangers of aluminum based adjuvants have been well documented. Animals injected with aluminum adjuvant, for example, suffer various neurological deficits. In 2017, ICAN even published a white paper summarizing the science which explains how aluminum adjuvant can cause neurological impairment when administered to babies.
Given the foregoing concern, a FOIA request was submitted to the National Institute of Health (NIH) requesting “copies of any human or animal studies involving the subcutaneous or intramuscular injection of aluminum adjuvant relied upon by the NIH to establish the safety of injecting infants and children with aluminum hydroxide, aluminum phosphate or amorphous aluminum hydroxyphosphate sulfate.”
The NIH engaged in an extensive search that included having the following institutes within the NIH search for responsive studies: the NIH Office of Intramural Research (OIR), the National Institute of Allergies and Infectious Diseases (NIAID), and the Eunice Kennedy Shriver National Institute of Child Health and Human (NICHD).
But despite their extensive search, the NIH finally conceded that “no records responsive to your request were located.” This admission is incredible. Despite injecting babies with thousands of micrograms of this toxic substance, known to cause cellular and neuronal death, the scientific medical brain trust of this country, the NIH, does not have a single study involving the injection of this substance that would support its safety. This may be because all of the studies involving injection of aluminum adjuvant reflect its dangers.
On August 6, 2020, ICAN filed a lawsuit against the CDC after it refused to produce the emails of the CDC’s top personnel involved in addressing COVID-19. ICAN also filed a similar but more involved lawsuit against the NIH for its emails and other relevant documents regarding COVID-19 and a potential COVID-19 vaccine. Just as the pharmaceutical companies will never rest when it comes to promoting and selling their vaccine products, we will never rest in exposing the truth regarding these products.
Obviously, the advocates of vaccination would argue, vaccination is a Good Thing. That is asserted as an axiom, an obvious truth that does not require any proof or evidence. (Exactly in line with the usual behaviour of The Anointed, as examined in Thomas Sowell’s classic “The Vision of the Anointed”. They are the superior ones who Know Best and who tell the broad masses what is good or bad for them. They are often wrong, but never in doubt).
Since vaccination is believed to be a Good Thing, any experiments or surveys would be potentially harmful. What if they showed that vaccines sometimes harm – or even kill – people? That would discourage the broad masses from accepting vaccination, which would (by definition) be a Bad Thing.
As long as they can get away with simply asserting that vaccines are a great blessing and never do any harm, what incentive is there to do any research on their safety and effectiveness?
And think of the lost profits…
Thanks for that, AhNotepad – I hope you keep us posted on that. When I see the numbers of people nowadays with autistic-like symptoms, I can’t help but wonder if this is more than just that damaged babies are saved my modern medicine. The tragedy is, of course, that most of those inoculations are for relatively mild diseases.
If you go to https://www.icandecide.org/ and/or https://thehighwire.com/ you can subscribe to their newsletter and I think you will get the updates directly.
Thanks for posting this
Thanks for a v interesting information/discussion from Sweden. Always good to know what doctors on the ground think about this. I am in general agreement with Dr. Rushworth’s opinion on this matter.
However, I have some queries about this. So as discussed in his blog, on average year, influenza kills 700 in Sweden, but covid has killed 7000. However, IFR, as in most countries, sit at about 0.12, which I think is roughly in line with pronouncements from e.g. CDC. IFR 0.12 is not alarmingly high by any interpretation. But then covid in Sweden has killed more people by an order of magnitude (even if they are old with serious comorbidities and probably was due to pass away at some point this year).
I understand this is probably because number of those infected was much higher for covid than inluenza – do I understand that correctly? So that means covid was far more infectious than influenza?
Do you think that increased mortality (compared to influenza) was at least partially due to lack of protection afforded to those who are more susceptible, such as the nursing home population?
Do you think with covid having killed those who would have died this year months early (which is as you say a terrible tragedy for families who wish to spend even one day longer with their loved ones), that you will see a proportional reduction in deaths amongst these vulnerable population this year (maybe even into early part of next year)? And are there indications of this happening already?
If you were having a public health discussion regarding this, how would you explain to a lay person this discrepancy of IFR 0.12 and order of magnitude higher deaths from covid compared to average influenza year?
Thank you very much, and I really appreciate your informed and considered blog – I have been enjoying your contribution for many years.
August 8th CP posted two interviews with Dr Richard Bartlett.
The first one was pulled by Youtube.
What is going on here?
What was wrong with Dr Richard Bartlett’s interview?
A conscientious doctor talking about how he treated Covid19 patients.
Other countries have followed similar protocols – with great success.
The treatment Dr Bartlett follows is the subject of investigation in medical establishments around the world as a possible route to treat Covid19.
Was he violating Medical Practice?
Why has it been pulled from Youtube, this is a disgrace against, Science, Medicine and Free Speech.
Does anyone have a link to the censored interview?
Can’t believe this…. well I can now
Do a search on brighteon(dot)com
Thank you Glenn…. well it’s there OK.
I find this profoundly shocking and depressing, it seems as Dr Richard Horton said – we have entered a very dark place – can’t find the original quote, maybe it’s been removed.
And thank you Dr Kendrick.
I can’t imagine how much work is involved in just running this blog and keeping on top of readers posts like this one, never mind all the research and writing you do.
You’ve opened up a number of doors into dark places, this one on censorship is frightening, and we seem powerless to do anything about it.
Thank you and all the others who refuse to be intimidated and continue to demand we have the right to the Truth.
Any thoughts on the Australian COVID-19 Aged Care Support Program?
Total amount available: $52,900,000.00
The COVID-19 Aged Care Support Program will reimburse eligible aged care providers for eligible expenditure incurred on managing direct impacts of COVID-19. The Program will run over 2 years from 2019-20 to 2020-21. The Program will assist Residential Aged Care, National Aboriginal and Torres Strait Islander Flexible Aged Care Program and Home Care Package providers that are subject to direct COVID-19 impacts, to deliver continuity of safe quality care for consumers.
Eligible applicants can apply for funding for each impacted service for the periods between the date on which the resident, staff member or client is tested for COVID-19 and the date on which direct COVID-19 impacts are resolved (i.e. no infected or isolated residents, staff members or clients).
Could be beneficial? Or a nice little earner?
Reference: Current Grant Opportunity View – GO3844 https://www.grants.gov.au/?event=public.GO.show&GOUUID=068A9519-03B3-6B9E-7B61126A5ABA12C1&fbclid=IwAR0LuxXg5w0mTJHqOwAcp4nXCpwve90xpoZdI7ygrROzrOrhLVr-cAMgrHg
Completely off topic, but F. William Engdahl is worth reading (concerning U.S./China relations):
https://www.lewrockwell.com/2020/08/no_author/towards-a-us-china-war-the-creation-of-a-global-totalitarian-system-a-one-world-government/
I would argue that German industrial base is far from “hollowed out”. Exports constitute 60% of German economy, if I am not mistaken. It’s higher than China’s, isn’t it?
I can’t help thinking that the key to this pandemic is twofold — (a) shorten the duration of illness among those infected, and (b) shorten the duration of infectivity among those infected. No test or PPE can do either of these (although PPE CAN decrease the possibility of spread from those infected to those who aren’t, so masks, for instance, are reasonable.) But a test without treatment is only a binary outcome — the subject is either infected or not. Is the subject infectious or ill, or both? That’s what you tackle with treatment, as soon as possible.
The idea, of course, is to make sick people better as soon as possible. Sounds like medicine to me.
Jimmy Christian, It depends who’s idea you are talking about. The idea of pharma is to keep people as sick as possible to increase their drugs market. If that was not the case, why do they pay so much money to practitioners to use their products?
“To make sick people better as soon as possible” Yu mean CV19 labelled – to the detriment of all other afflictions and to the economy and to government finances – stupendous cost for minimal effect and maximum signalling.
In case anyone hasn’t yet seen it, look at this article: https://www.cebm.net/covid-19/public-health-england-death-data-revised/
It is by Carl Heneghan and Jason Oke, the scientists who pointed out that the UK government was grossly and inexcusably overcounting Covid-19 deaths by assuming that anyone who tested positive and then died had died of Covid-19.
Especially the second graph. Just gaze at it and let the implications sink in. Since 1st July, the official government figures exaggerated by a factor of *at least* 3. More recently, that factor has risen sharply as the number of deaths has fallen. “As opposed to 100 deaths on the 11th of August, 11 would now be reported; today, whereas 72 were reported, only 15 will be reported under the new system”.
Ask yourself whether it is remotely credible that any half-competent government would make such an idiotic schoolboy error – by mistake.
Tom, thanks for that link. I note it is from The Centre for Evidence Based Medicine. That seems a more honest organisation, which the government should use for their advice rather than Imperial College. I wonder if their name (Imperial) is more about empire building than a historical tag.
Since the UK government has at its disposal huge numbers of civil servants and others, many of whom are highly intelligent and trained to the hilt, I don’t see why it can’t follow simple common sense and continually monitor all information and informed opinion. Why choose one organisation (of extreme ill repute, with an established record of consistent abysmal failure) and pay no attention to any of thousands of other fine scientists and doctors with contributions to offer?
I think it may be yet another example of what has come to called “policy-based intelligence”. In other words, they decide on the policies and then make sure that they are given “intelligence” that justifies the chosen policies. Everything else is steadfastly ignored. (Exactly as in – for example – the run-up to the invasion of Iraq).
This may go some way towards explaining. I have come across Tom Woods in only the past few days, but this lecture seems very on-topic. https://youtu.be/K2_dPLBlvDI The UK government (of occupation) has now “ordered” “committed to” or whatever mealy mouthed phrase they use, over 300,000,000, that’s right THREE HUNDRED MILLION!!! Vaccinations for something that does not yet exist, and the mealy mouthed government spokesman on Radio 4 news says the vaccine is the only way to mitigate against this virus that is now struggling to kill into double digits daily. If they talked to Richard Bartlett, they could probably eliminate most of those deaths. Still, the only to fix the problem is to spend loads of money on an unproven treatment, smacks of the Tamiflu farce.
AhNotepad: 300,000,000? That means five jabs each for every man, woman, and child in the Mother Country?
Gary Ogden – FIVE??? They’d have to catch me first, even for one.
JanB
They won’t have to catch you. Having 5 shots available (actually I think the real figure was 340million but I didn’t want to exaggerate, so a bit more than 5), will allow the use of a repeating dart gun, so you will be driving through with someone taking pot shots to administer the vaccine. They have enough to afford a few misses.
Hi janet; for people afraid of jabs
https://www.technologynetworks.com/biopharma/blog/oral-vaccine-for-covid-19-on-track-towards-human-clinical-trials-335335
To effectively eliminate the virus WHO could incorporate this technology into the food supply on a global scale.
Alternatively people just need to eat proper food and look after their immune system. Then we wouldn’t need this unproved and probably hazardous pharma crap. We don’t have the crap at the moment and governments are finding ever ingenious ways of keeping the numbers up, so the disease is nearly done.
It’s not the fear of the needle, it’s the deep suspicion of any vaccine. I think Ive had my last flu jab EVER. They’d have to catch me for the untested experimental C19 vaccine. I’d sprout wings to avoid it. If they want to put an oral one in junk food then let ‘em. I’d be safe from that too.
Hi janet: our scientists are working on a healthy vaccine for health conscious people. Sprouting wings might be a side effect.
https://www.cbc.ca/news/canada/ottawa/covid-19-research-edible-vaccine-plants-tomato-lettuce-mucosal-immunity-1.5626484
PHE figures – not UK government.
PHE is so close to the government, they can be seen as one and the same in this instance. If not, why does the government take so much notice of them?
“PHE is an executive agency, sponsored by the Department of Health and Social Care”.
https://www.gov.uk/government/organisations/public-health-england
The government may have taken some half-hearted measures to let it argue that PHE is not a government department, but to all intents and purposes it is.
What is the phrase? “Two cheeks of the same arse?”
Quite appropriate, Steve. They have a hell of a lot of cheek, and they have plenty of arses.
“Why is it that there are so many more horses’ asses than there are horses?”
– G. Gordon Liddy
The blue curve (28 day limit) looks as if it is asymptotically approaching zero – which is very encouraging.
Interesting article about aged care homes during Covid:
How Covid exposed the world’s lack of care – UnHerd
https://unherd.com/2020/08/how-covid-exposed-the-worlds-lack-of-care/
Help, anyone! Our doctor’s surgery has just rung us up to say we are eligible for a ‘drive by’ pneumonia vaccination and they have pencilled in appointments for us. Husband queried the fact that there are different types of pneumonia, but the recepeptionist obviously had no idea what was being offered.
I am not medically qualified, and of course the decision is yours to make. But I cannot see why anyone would want a “pneumonia vaccination”. Just avoid Arctic conditions (not hard in the UK at least right now) and don’t get drenched.
Thank you for those thoughts, Tom. I’ve now found this interesting scientific appraisal which appears to come to more or less similar conclusions: https://www.sciencedirect.com/science/article/pii/S0954611111002423
I now recall that I caught double pneumonia (i.e. in both lungs) at the tender age of 12, in a way that surprised me at the time.
It was summer, oppressively hot, and I was coming North from London to Glasgow by sleeper. Having settled down in the top bunk, covered by only a sheet, I still felt stifled – so, being young and foolish, I opened the little top window as far as it would go and promptly fell asleep.
In the morning – hey presto, double pneumonia! Being young and healthy I threw it off after a week in bed (which I thoroughly enjoyed, reading stacks of books and being waited on – as my mother put it – like the Shah of Persia). No antibiotics or other treatment were needed.
I had double pneumonia when I as 19 or 20. I spent a month or so before Easter starting up a new stables while living in a damp touring caravan with a paraffin heater. It was snowing, and we spent a lot of time cleaning out out cow byres with ancient straw in them. I got so tired that I often didn’t bother to eat. I never did find out whether it was bacterial or fungal, but I bet the the combination of stress, bad diet, cold and manky straw had a lot to do with it. It wasn’t actually that bad – i just thought my asthma was worse than usual
Incidentally, I like the idea of a “recepeptionist”. So many of those people seem to be gloomy and lethargic… 😎
A happy slip of the keyboard obviously. It must have been the shock of a pro-active approach from the surgery. Never ever happened before, though in another authority my 97 year old mother in law is also suddenly receiving unasked for attentions as to her diet and bone density. Good heavens! I thought they’d rung us up to self-isolate because other half had been for a haircut and had to fill out a contact and trace form 🙂
OMG, medical equivalent to drive by shooting? 😬
Oh I like it! Actually that’s what the prospect rather felt like. Apparently everyone over 65 needs to be PPV-ed unless one reads this research paper: https://www.sciencedirect.com/science/article/pii/S0954611111002423
I guess I’d not go ahead if it was me – not without knowing in advance exactly what it was for!
Yes, no preliminary discussion with any of our doctors. Mind you, we do our best to avoid them. Am suspecting this is a ‘second wave’ covid effect. We’ve never been approached for vaccination before, this despite both of us being age-wise ‘eligible’ for several years now.
An here’s me still juggling the letter from the health centre ‘inviting’ me to have a shingles jab.
I was booked to have a shingles jab, but then it was delayed for some reason, then back in December, I asked if the nurse who was going to take a routine blood sample could do that as well. I was told no, that had to be given by a specially trained nurse, who was away! Of course, before that was arranged, the CV-19 nonsense arrived. I’ll probably have another vaccination for anything by now – I am utterly disgusted by the medical profession (with very honourable exceptions, such as Dr K, of course).
Think I’d struggle to get a date to suit.
My thoughts too, Jerome. Thank you.
Dr. Mercola has written a few great articles about the pneumonia vaccine a while back. Here is one: https://articles.mercola.com/sites/articles/archive/2012/05/22/pneumonia-vaccine-shown-to-actually-increase-bacterial-infections.aspx
If you would like to learn why vaccines are unsafe and best avoided, Andrew Wakefield recently made this outstanding docu drama movie about it, which I highly recommend: https://1986theact.com/
Dr John H – many thanks for this link. I do follow Dr. Mercola, but hadn’t checked his site for PPV.
Tish Farell: I say cancel the appointments. The pneumonia vaccines are among the most problematic. No licensed vaccine has ever been properly safety-tested, and post-marketing surveillance is weak at best. To avoid pneumonia, or any other infectious disease, enhance your immune function. Avoid any foods with sugar, flour, or vegetable oils (except special occasions). Eat lots of high-quality animal foods and animal fat. Reduce carbs to the lowest levels tolerable. Get out in the sun. Avoid social distancing and masks like the plague. And most importantly keep an extra-sunny disposition.
Lots of sound advice, Gary, thank you.
Ask them if they are also offering fries with that.
Here is the viral interference paper (from the flu shot given to Department of Defense personnel):
https://www.sciencedirect.com/science/article/pii/S0264410X19313647?via%3Dihub
“Conclusions
Receipt of influenza vaccination was not associated with virus interference among our population. Examining virus interference by specific respiratory viruses showed mixed results. Vaccine derived virus interference was significantly associated with coronavirus and human metapneumovirus; however, significant protection with vaccination was associated not only with most influenza viruses, but also parainfluenza, RSV, and non-influenza virus coinfections.”
What are they saying? It seems it doesn’t interfere, unless it does.
You have to read to practically the last paragraph to get to ‘the beef’.
This is the relevant section
‘The odds of testing positive for individual respiratory viruses by vaccination status were also examined (Table 5). The influenza vaccine was sufficient at protecting all influenza virus results tested for at a significant level except two (Influenza B Victoria and Influenza coinfections) (Table 5). Both Influenza B Victoria and Influenza coinfections had reduced odds in the vaccinated cohort, but not at significant levels (Table 5). Examining non-influenza viruses specifically, the odds of both coronavirus and human metapneumovirus in vaccinated individuals were significantly higher when compared to unvaccinated individuals (OR = 1.36 and 1.51, respectively) (Table 5). Conversely, all other non-influenza respiratory viruses had decreased odds in the vaccinated population, including significantly decreased odds ratios in vaccinated people with parainfluenza, RSV, and non-influenza virus coinfections (Table 5). Additionally, the odds ratio in the no pathogen detected cohort was significantly higher in vaccinated versus unvaccinated individuals (OR = 1.51) (Table 5).
From https://www.sciencedirect.com/science/article/pii/S0264410X19313647?via%3Dihub A paper in Vaccine pub Elsevier called ‘Influenza vaccination and respiratory virus interference among Department of Defense personnel during the 2017–2018 influenza season’
Since there has never been an RCT on a vaccine, I take all such studies with a large pinch of salt.
Not only a large pinch of salt, I am now in need of a good whiff of smelling salts to bring me round from total collapse following attempts to make sense of the statistical mumbo-jumbo. Time for a refresher from “Doctoring Data” I think.
“Shutting down completely in order to decrease the total number of deaths only makes sense if you are willing to stay shut down until a vaccine is available. That could take years. NO COUNTRY IS WILLING TO WAIT THAT LONG.” (EMPHASIS ADDED)
Hello! Over here…United States of America…land of the idiots and home of the criminally insane.
You should change up your associates. I estimate only 30% are insane. They just make more noise.
The GPMB global preparedness monitoring board, might call it a subsidiary of WHO produced its annual report for 2019. Can be down loaded as a PDF. Link here https://apps.who.int/gpmb/annual_report.html
On page 39 the 2nd of four short paragraphs in the bottom half of the page is as follows –
“The United Nations (including WHO ) conducts at least 3 systemwide training and simulation exercises including one covering the deliberate release of a lethal respiratory pathogen”
This is without any footnote to explain how this is contained or controlled so as to put people’s minds at ease and is a reckless statement to release to an already worried population to say the very least.
The next 2 paragraphs go on to refer to mobilising national and international actions and convening through the UN general secretary high level meetings with international health, security and foreign affairs officials to determine next steps basically.
Very careless misuse of words indeed.
Journalists need to seek explanations from Mike Ryan and or any other WHO spokespersons in order to get the assurances and explanations we deserve.
Has the US just hit a new high on the hysteria meter?
Wisconsin’s Department of Natural Resources now requires that masks be worn during at home Zoom meetings:
https://www.kansascity.com/news/nation-world/national/article244861827.html#storylink=cpy
Well, Dr. John, I suppose it indicates that we are all being very well behaved and obedient children.
Honest to god, the world has gone quite mad.
Yes, quite batty.
Even worse, Dr. Mercola reports that states are requiring that students be fully vaccinated even if take all of their classes online!
https://articles.mercola.com/sites/articles/archive/2020/08/18/virginia-requires-student-vaccination-for-online-learning.aspx
The world is being run by psycho’s. Tom Woods on the psychotic US police state. They’re not? Why does Los Angeles police department need a submarine? (Please anybody, don’t try to justify it).
“Why do the LÁ police need a submarine?” Because LA County has a coastline about 150 miles long, longer if you include if you include the Channel Islands. Drug cartels often dump drugs on the sea bottom to be picked up by fishing boat. Bodies are dumped at sea too. There are also wrecks that need to be found.
Is this a misinformation channel? I saw a video https://youtu.be/h0EDK1Rr_ng that was “recommended” by utube. Being gullible, I have seen some other videos by Upward Look TV and in some ways they pander to my paranoia, as did the title of this one initially. The problem with this one is the facts seem a bit less like fact, and more like propaganda. Infrared thermometers, as I understand them, measure the infrared emitted by a surface. They do not fire pineal gland damaging infrared beams at the head. Some thermometers use a small laser to shine a spot to indicate roughly where the temperature will be measured. So what opinions do others have?
I don’t see any problem with the infrared temperature measurement as an exercise. The results may be rubbish, as my Testo thermometer showed I was about 31ºC, a cool lizard, have I been shape shifted? One thing I don’t agree with is pointing a gun like gadget at peoples” heads. I might react with a kick in the nuts.
I can’t find any contact details for Upward Look TV, and the nearest possibility is Upward Look, which seems to be associated with Ellen G Whyte, of Seventh Day Adventist Vegan fame, and eating meat encourages self abuse etc. So the youtube channel looks to be of poor quality. About the level of a Fauci.
According to the instructions that came with mine, you have to hold the thermometer only 2-3cm (1 inch) from the face or, yes you’ll register as dead or a lizard. You also need to have been indoors for 30 mins, at rest for at least 10, and various other things also affect reading – so being measured outside a pub is pretty pointless. Apparently wearing a lot of makeup or greasy sunscreen will also give you low reading (so useless for hen nights), so there you go.
The world has been ascribing a wide range of symptoms to Covid19.
Is this not just highlighting symptoms caused by viruses in general but not generally ascribed to them? Symptoms / conditions perhaps sheltering under the term “Idiopathic”? Should we be thinking “idiopathic so it’s maybe viral?”
Maybe after this virus we will learn to better recognise the influence of other viruses and improve diagnosis and avoid inappropriate treatment. No, I’ve just seen the pigs flying over again.
Great article!!
I am alone here in London thinking it’s all madness, and that lockdown made no difference to death numbers but certainly screwed our country for a long time to come
Terrible mistakes by government and still making awful decisions as in this quarantine nonsense
Sue, it is madness, but deliberately so. If you haven’t seen it, have a look at ukcolumn.org for the analysis. What they say is not refuted, but some self-opinionated group called “news-guard” has given them a red warning rating as they could be spreading misinformation. Funny that, when all the figures they use are taken from UK government published data.
Another source is Vernon Coleman who will have another video on youtube tonight, if youtube hasn’t censored it.
The first part of https://youtu.be/uqla0O8t1Sw tells why so many have died in the UK because of the inhumane actions of the dictators johnson, cummings, hancock et al.
Then there’s the economic insanity https://youtu.be/541bajR4k8g. Tom Woods has a load of revealing videos.
Now we know why democracy works and autocracy fails – it is such a shame that we needed to re-learn this obvious truth. Most people know that they haven’t encountered a single instance of this disease, yet the measures to contain it are ruining the country and wrecking people’s lives.
Yes, David. Most people think that the UK and USA are democracies. Yet they are just as much dictatorships as any other nation. It’s just that here, the governments stage elections periodically in which the people can vote to switch to another of the tiny pool of authorised “dictator candidates”.
Finally !
Thank you and please keep us updated.
The Swedish doctor acts as if flattening the curve is pointless because the same number of people will die eventually either way. That is not true.
First of all, when hospitals are overwhelmed, patients get inferior treatment; when the curve is flattened, hospitals/docs can give more, better care to each patient. Second, doctors (in NYC at least) learned a lot in the first months. In the beginning, they told people who got sick to stay home unless they had breathing trouble. In time, they realized that covid 19 was unlike other respiratory illnesses in that people could have very low oxygen without realizing it. So doctors began advising people to monitor oxygen at home and go to the hospital if their level reached a certain number, regardless of how they felt. Bringing people to the hospital sooner meant they began treatments earlier in the course of the illness, and that, too, improved outcomes. Doctors also adjusted various hospital protocols as they learned more: eg waiting longer to put people on ventilators, putting people in prone positions to stimulate oxygen flow, etc. All these factors increased patients’ odds of surviving. So flattening the curve meant fewer people died in the end.
Another thing to consider: In NYC, the first wave of infection caught everyone by surprise – nobody knew covid 19 was spreading until many people were already infected. Once older/vulnerable people began to realize how widespread and dangerous the virus was, many opted to stop going out. In my extended family (and in the families of my friends), the older people are avoiding exposure. The younger people do chores that involve more risk of exposure. The young people also wear masks and distance when they are around older/vulnerable family members and friends. I suspect the same thing happened in Sweden – and is still happening: Older/vulnerable people witnessed how covld 19 affected their peers and decided to hunker down till there is a vaccine – hence slowing down case/death rates.
Even if Sweden were some wonderful exemplar (which I don’t buy), countries are different. Sweden is small, homogeneous, relatively well off, with good social safety nets. The US is diverse, features enormous income inequality, had vastly inferior social services. Millions of Americans lack even basic health insurance. So any infectious disease is going to take a greater toll here. If the US had done what Sweden did, the results would have been very different.
One last point. I get very tired of people dismissing the deaths of older/vulnerable people. 700 died of flu, 6000 of covid. Why not flatten the curve and protect the vulnerable till there is a vaccine. My mother is 90 and still living a happy, full life surrounded by her children and grandchildren. She has quite a few friends in their 80s and 90s who are also still leading meaningful lives. Among my husband’s family, a number of people, despite being young and fit, have diabetes; in my family, several young people have autoimmune disorders. In the US generally, research has shown that people of color and poor people are much more vulnerable to this virus than the rest of the population. I don’t agree with the doctor that it’s reasonable to sacrifice a disproportionate number of the vulnerable so those born healthy/able to afford health insurance can go out to restaurants, etc. (PS The people who actually die from covid 19 are not the only victims – surviving family members suffer emotionally and often materially, too – as when a child loses a parent/provider, an older person loses a spouse, etc.)
Lisa, you say: “I get very tired of people dismissing the deaths of older/vulnerable people. 700 died of flu, 6000 of covid. Why not flatten the curve and protect the vulnerable till there is a vaccine.”
Why should there be a vaccine? I’m questioning whether it’s appropriate for Bill Gates and his WHO to be leading a very expensive ‘race for the coronavirus vaccine’.
As I raised in a recent rapid response published on The BMJ, there are suggestions that “A vaccine against Covid-19 may not work well in older people who are most at risk of becoming seriously ill and dying from the disease…” and this “may mean immunising others around them, such as children”.
As children do not appear to be adversely affected by SARS-CoV-2, I don’t think it’s ethical to vaccinate them to supposedly protect the elderly.
Apparently they’re already vaccinating children against flu to protect the elderly, how on earth did this get by ethics?
You can read my BMJ rapid response via this link: https://www.bmj.com/content/364/bmj.l108/rr-4
Do you think it’s ethical to vaccinate children to supposedly protect the elderly?
“First of all, when hospitals are overwhelmed, patients get inferior treatment…”
Hospitals were NOT “overwhelmed” in Sweden, nor in the UK – on the contrary, many of them were vertually empty as they had stopped all normal treatment and had few (or no) Covid-19 patients either.
As for New York, there were special circumstances there.
“Frontline Nurse Speaks Out About Lethal Protocols”
https://www.lewrockwell.com/2020/08/joseph-mercola/frontline-nurse-speaks-out-about-lethal-protocols/
“Heroic Citizens Going to Local Hospitals and Fact-Checking the LYING MSM”
https://fromthetrenchesworldreport.com/heroic-citizens-going-to-local-hospitals-and-fact-checking-the-lying-msm/265045
Lisa, the vaccine, ah, the vaccine will save everybody, the vaccine for which Billy Gates has just gained immunity, not for the disease, but for legal immunity from prosecution if it kills or otherwise harms people. A vaccine which has been developed so fast, to combat a disease so dangerous you only know you might have it if you get tested with a test that was never intended as a diagnostic test.
Lisa,
There are at least 2 cures for COVID available now with near 100% success (HCQ + zinc & MATH+ Protocol). Because these are cheap and effective, they have been banned on behalf of the drug companies who want to sell us a very expensive and likely unsafe vaccine instead. Ventilation is a death sentence and is largely responsible for the high number of deaths, particularly in places like New York. Vitamin D is a highly effective preventative, especially needed for people of color. Very, very few people need to die from this, and no one needs to be afraid of it anymore.
If you want your family to be safe and healthy, then fight for health freedom, not for the drug companies.
MATH+ Protocol:
https://covid19criticalcare.com/treatment-protocol/
HCQ + zinc:
https://www.newsweek.com/key-defeating-covid-19-already-exists-we-need-start-using-it-opinion-1519535
Vitamin D:
https://articles.mercola.com/sites/articles/archive/2020/08/17/impact-of-vitamin-d-on-covid.aspx
Dr John H, thank you for some reality to counter the poorly informed fear mongering.
Dr. John,
What about budesonide? Have you looked into that yet?
Well said, Lisa.
Not to mention that even (American) football (not soccer) players are getting Myocarditis from Covid-19:
https://bleacherreport.com/articles/2904115-report-at-least-10-big-ten-football-players-have-heart-condition-myocarditis
How bad is this? I assume they will fully recover, but only some time will tell.
I also hear a lot about “long haulers”, who have sequelae that can last months. How prevalent is this? I haven’t seen a good analysis. I think it’s way down on the list of things to analyze.
As for Sweden, I can’t even tell what they did, let alone try to analyze it.
Hmmm, football players, unhealthy lifestyle, steroids, over training etc. 10 out of how many sports players in the world?
Lisa,
Two things. First, flu vaccines are somewhere in the neighborhood of 50% effective and this one will be untested and is anyway a new and different type of vaccine than has ever been used. Also, it is not for sure a vaccine will be developed at all. Life cannot be put on hold for a vaccine that may not materialize.
Second, flattening the curve should have taken about 3 weeks but lockdowns, especially prolonged ones, actually kill more people as well as destroying lives. Can I guess that your own income has not suffered? Those in favor of lockdowns always speak as though they are the compassionate ones with the moral high ground. That is hardly the case. It is actually unspeakably selfish to demand that young people and strangers sacrifice their livelihoods, the psychological health, even their physical health for unknown people, mostly old.
Anyway, I am getting tired of the fear when we already have therapeutics that work. If people are so concerned, instead of harrangueing people to wear masks and keep their children locked up for months on end, why not start demanding that these game changing therapeutics be used immediately?
Yes, most of the people in favour of lockdowns seem to be those whose income is not affected, esp those who work in the pubic sector and are being paid often full salary to stay home and do very little, or those who are furloughed from large private companies (and don’t realise that they’ll be made redundant soon), so getting as much money for doing nothing (as they save on travel and lunches). The small businesses and self employed are being decimated, and those who’ve been working all along understand that, for most people, it’s not all that serious and so want to get back to normal working
KJE,
The problem is that if we don’t get our economies running again very soon, there will be cascading failures. How long can all these white collar workers continue to be paid when there is no productivity and no tax base?
I agree that we have therapeutics that work – at least as well as anything that is being proposed and certainly very much more safely – but it is getting harder and harder to get the message out.
I gave an online product review on the zinc ionophore Quercetin but the company selling it emailed to apologise for being unable to print the review because I had used the word Covid-19.
I fear that we are going to be forced into agreeing to be GMO’d – as Vernon Coleman has put it – with completely unknown consequences. It is to be hoped fervently that, if this is planned as a cull of the population by the ‘entitled’, then as in Douglas Adams’ Golgafrincham ‘B’ Arc episode, those who devised the plan perish as a direct result of ‘unintended consequences’.
Future hind-sight
https://www.kevinmd.com/blog/2020/08/how-will-future-generations-remember-covid-19.html
Massive fatigue lasting months seems to be a common occurence, even in a significant percentage of those who did not need to be treated in hospital.
https://www.theguardian.com/australia-news/2020/jul/17/most-covid-19-patients-admitted-to-a-sydney-hospital-in-march-still-have-symptoms
https://www.zeit.de/wissen/gesundheit/2020-08/fatigue-corona-spaetfolge-muedigkeit-erschoepfung-covid-19
I wonder what the economic impact of that is, and supposing a country just let the virus run wild, how that would compare to the cost of a lockdown.
Eric, I wonder what will be the economic impact of implementing probably annual coronavirus vaccination with fast-tracked experimental vaccine products across the entire global community, most members of which are so far apparently not at risk from this virus, particularly the young.
I wonder what ‘unintended consequences’ (or possibly intended…) might result from this ill-considered and rushed response to a virus.
I was not talking about vaccines, though I think a well tested vaccine would be a good way out.
What I was saying is that nobody is looking at the economic impact of those survivors with long term issues, especially not those lamenting the economic impact of lockdowns. It is also interesting to see that countries with no or soft lockdowns took an economic hit that was only a little smaller. And early reopening in the US is turning out to be a boomerang.
Eric,
Gee, you support the lockdown no matter what. No argument about the much greater fallout fazes you. Now you worry about the economic result from a handful of people who may carry longer term issues on the economy but not the 30% unemployment! Are you grasping at straws?
By the way, it is likely that many of those suffering longer term consequences were not treated well, or even were on ventilators, whereas now we know how to treat covid early before symptoms like that get out of hand.
The fear of covid is really over. A couple more of our governors recently quietlydropped their bans on hydroxy. Maybe they realize the lawsuits that may result from knowingly letting people die without existing treatments. Do you think governors and mayors ought to be telling doctors what to prescribe?
I was not talking about vaccines, though I think a well tested vaccine would be a good way out.
It would also be a first.
If only we had effective prophylaxis or effective treatment for full-blown Covid-19.
Well duh!
The reason we are not letting the lockdown loose has nothing to do with our purported inability to deal with the virus, and everything to do with profit in the pharmaceutical sector.
Doctors everywhere should be outraged that they have been prevented from following their vocation without interference from purse-string holders.
Time to have a close look at the pandemic preparedness simulations, e.g. Event 201 held in October 2019, and also check out this article: Two decades of pandemic war games failed to account for Donald Trump: https://www.scientificamerican.com/article/two-decades-of-pandemic-war-games-failed-to-account-for-donald-trump1/
From where I’m standing, a new virus is a huge business opportunity…tests, medications, vaccines…etc, etc…
While many suffer in oppressive lockdown, others reap rich rewards… Just think of all those hastily cobbled together multi-billion dollar vaccine contracts being signed now, some people are going to make a motza out of this, whether a vaccine ever eventuates or not…
Seems this virus has been made to fit the bill for a massive over-reaction – is this really the way it should have been handled?
What appears to be seriously lacking is independent and objective infectious diseases specialists to consider the best course of action, does such a being exist? Perhaps Anders Tegnell fits the bill?
Unfortunately, it looks like this area of public health has been hijacked by the vaccine industry and it’s acolytes in academia and the medical establishment, with the wholehearted support of governments and the corporate media.
It’s the medical industrial complex gone mad, and it’s having very serious repercussions for our political systems, i.e. the undermining of liberal democracy with encroaching medical tyranny.
Myocarditis developing weeks after CV infection. Makes me wonder if the huge peak of heart disease in the 1960 – 1980s was due to some unreconized epidemic:
https://jamanetwork.com/journals/jamacardiology/fullarticle/2768916
Many people have thought the same thing. The main problem with this hypothesis is that countries like Japan had very low rates of heart disease during all of that period.
Yes, that is where you have to engage in some more twisted handwaiving. Having visited Japan many times since the late 90s, I can say that Japanese adore food and are still overall slim and healthy, in spite of Western foods such as pizza, fast food joints and viennese style cakes being available everywhere. It is easy to extrapolate that their food was yet healthier 50 years ago. And apparently, soy and sesame oil and white rice are not so bad when consumed in moderation and embedded in a generally healthy diet.
Im am guessing that Thailand, Vietnam, Indonesia, Singapore, Hong Kong were similar during that time?
Were the Japanese possibly protected by a diet high in fish and seaweed? I would have thought that they would have quite high Omega 3 levels.
what a land of perfection you conjure up Eric; everyone well and healthy; please dream on; T2 diabetes is becoming increasingly common in what used to be called the Far East. China has rapidly rising rates; have a listen to this video https://www.youtube.com/watch?v=S5NLGKacFgs
Although I have never even set foot in Asia, I always understood that Japanese culture would dictate a “gourmet” approach to enjoying food rather than “gourmand” (connoisseur rather than greedy).
Don’t they eat fairly small portions, focussing on quality rather than quantity?
Interesting point. I’ve always found this paper intriguing, but it does not mention Japan at all. And the 1918 flu hit Japan pretty hard.
Dr David Grimes has long maintained that the 20th Century epidemic of CVD was due to some organism. I know Dr Kendrick does not agree with this, but you might want to look at http://www.drdavidgrimes.com/2013/07/an-epidemic-of-coronary-heart-disease.html
Incidentally, heart problems are not unique to Covid-19. They seem to be characteristic of influenza like illnesses.
“Studies have shown that flu illness is associated with an increase of heart attacks and stroke. A 2018 study found that the risk of heart attack was 6 times higher within a week of confirmed flu infection. These findings were most pronounced for older adults and those experiencing their first heart attack.” — https://www.cdc.gov/flu/highrisk/heartdisease.htm
It has been known for a very long time that infections anywhere in the body can lead to heart disease. One especially high risk is gum disease. People with bad teeth and gums are likely to suffer from serious illness including heart problems.
One fairly simplistic explanation:
https://www.mayoclinic.org/diseases-conditions/endocarditis/symptoms-causes/syc-20352576
“These findings were most pronounced for older adults and those experiencing their first heart attack”.
That looks right up to the CDC’s usual standard of intelligence and logic. For “those experiencing their first heart attack”, I imagine the risk of a heart attack is… let me see… about 100%.
No?
Hi Eric: epidemic of saturated fat phobia followed by increasing consumption of vegetable oils is a simple explanation for heart disease pandemic. Other contributing misconceptions ; meat is bad, grains are healthy, cholesterol is bad, plant sterols are good, etc..
Current status of COVID knowledge:
https://www.statnews.com/2020/08/17/what-we-now-know-about-covid19-and-what-questions-remain-to-be-answered/?utm_source=STAT+Newsletters&utm_campaign=68d8cf406c-MR_COPY_01&utm_medium=email&utm_term=0_8cab1d7961-68d8cf406c-152161286
They don’t mess around in Queensland, Australia.
“You are not allowed to take hydroxychloroquine as a preventative measure for COVID-19.
If you don’t comply you may receive an on the spot fine of $1334, a court-imposed penalty of up to $13,345 or 6 months imprisonment.”
https://www.qld.gov.au/health/conditions/health-alerts/coronavirus-covid-19/current-status/public-health-directions/prescribing,-dispensing-or-supply-of-hydroxychloroquine-direction
Does the same apply to the use of Quercetin? Or chloroquine? Or quinine perhaps?
Sounds like be Pharma are controlling the Queensland legislature even more than the USA’s.
Lunacy
Jeez! What is the point? It’s as though they don’t want people to be healthy. And I though the NHS was bad …
And it’s as if they learned nothing by watching the mistakes and the therapeutics in the northern hemisphere. Are they putting people on ventilators?
“Are they putting people on ventilators?”
If they have a motive for maximising the number of “cases” and “deaths”, I’m sure they do. The advent of medical insurance, “best practice”, compulsory protocols and ethics committees has meant the obsolescence of that old-fashioned luxury, a conscience.
So… are you allowed to take hydroxychloroquine against malaria? Lupus? Rheumatoid arthritis?
Or just because you like the taste?
Surely, suffering from heart problems following a flu-like illness is an old and fairly common problem?
shirley3349, exactly. Diseases take their toll, it happens through the animal and plant kingdoms. Tuberculosis anybody? Those who favour lockdowns and draconian measures to avoid this current claimed virus have only death in their thoughts as an outcome, no matter that many will see life as not worth living because they are not allowed to enjoy anything despite the risk of the activity being far higher than the virus.
At the beginning of this deceit, how many people were saying, it’s selfish to not shut yourself away for a couple of weeks to protect the vulnerable. Well it’s extremely selfish for people to carry on demanding we are still shut in so those that are healthy and have a life to lead, are kept away from anybody with crp statements such as “Keeping apart will keep us together”. What total and absolute nonsense.
Oh shit… here’s another place you need to wear a mask.
Flushing a urinal, much like flushing a toilet, involves an interaction between gas and liquid interfaces. The result of the flushing causes a large spread of aerosol particles to be released from the urinal, which the researchers simulated and tracked.
“From our work, it can be inferred that urinal flushing indeed promotes the spread of bacteria and viruses,” says Liu. “Wearing a mask should be mandatory within public restrooms during the pandemic, and anti-diffusion improvements are urgently needed to prevent the spread of COVID-19.”
https://phys.org/news/2020-08-restroom-mask.html
Martin, we’ve been in the vicinity of flushing toilets and urinals for decades and most (near 100% I would venture) have not died as a result of picking up arseole particles. It’s just more mask nonsense. If people don’t stop it now, and push back against this control narrative, I predict they will be effectively slaves by early 2021. You have been warned, take no notice if you choose. I have been asking people this week if they have heard of Agenda 20, despite the fact I expected them to be worldly wise and would know what’s going on, NONE had heard of it!!!!
Since reading The Big Necessity a number of years ago, I have made it imperative to put the lid down before flushing – the thought of aerosols landing on toothbrushes and face cloths is not appealing. Of course, this is not an option in public loos with urinals and no lids!
Are any public toilets actually open? I always close the lid before flushing – but I’m not male
‘“From our work, it can be inferred that urinal flushing indeed promotes the spread of bacteria and viruses,” says Liu’.
Wow, big discovery. That’s been known for centuries.
About the only mechanism that’s even more efficient for spreading bacteria and viruses is an electric hot air hand dryer.
This is a mass psychosis/hysteria.
Australian prime minister says coronavirus vaccination is likely to be mandatory in Australia – see Scott Morrison expects a successful coronavirus vaccine would be mandatory in Australia: https://www.abc.net.au/news/2020-08-19/morrison-coronavirus-covid-19-vaccine-mandatory/12572992
Things are pretty grim in Australia… Here’s a comment I left on a newspaper article today:
In the space of a few months we have a new coronavirus, a newly named disease, and vaccine products in ‘warp-speed’ experimental development.
Scott Morrison announces this morning coronavirus vaccination will be mandatory for Australians.
As I noted in a previous comment on this thread, my reading of the Biosecurity Act 2015 indicates people who refuse vaccination could be at risk of five years imprisonment and/or a $63,000 fine.
So our ‘liberal democracy’ is in very interesting times, with the threat of mandatory vaccination, currently not allowed to leave the country, or even the state in some cases. And we have the example of the police state of Victoria, with people in lockdown, impeded from leaving their homes, with mandated masks, and curfews. The police and ADF are enforcing these edicts, and we’ve seen horrifying vision of a woman thrown to the ground with a policeman astride her, his hands around her neck, because she wasn’t wearing a mask.
I can’t believe what’s happening in this country, it’s terrible, our rights are being trashed.
Meanwhile, in the past six months, 438 deaths have been attributed to COVID-19 in Australia, 351 of these deaths are in Victoria. Most of the deaths reported are in people over 80 years old.
I hope people are starting to wake up and think about this…
Elizabeth Hart
Morrison has had to back down re mandatory coronavirus vaccination…
Prime Minister Scott Morrison has moved to assure Australians any coronavirus vaccine will not be compulsory, despite earlier saying he expected that would be the case.
Scott Morrison walks back mandatory coronavirus vaccination comments
https://www.abc.net.au/news/2020-08-19/pm-walks-back-mandatory-coronavirus-vaccination-comments/12575600
I suppose the good news is that there is clearly a groundswell of people in Australia saying enough is enough! Politicians ‘walking back’ pretty painful!
Walked back again… Health Minister Greg Hunt refuses to rule out consequences for anti-vaxxers refusing COVID vaccine: https://7news.com.au/sunrise/greg-hunt-refuses-to-rule-out-consequences-for-anti-vaxxers-refusing-covid-vaccine-c-1252235
Returning Australians to their roots… making it a land of convicts again. ;o)
Elizabeth, searching for independent AUS media sources & found this critical of Scott Mo.
https://www.crikey.com.au/2020/08/20/scott-morrison-covid-19-vaccine/
Maybe this news source is suitably independent of the 70% monopoly of AU media enjoyed by Rupert ?
He writes:
“Practically everyone who was tested had COVID, regardless of what the presenting symptom was. People came in with a nose bleed and they had COVID. They came in with stomach pain and they had COVID.”
Thuis is because there is no virus, as i explained before, there is no proof that sars-cov-2 exists, that is why the rt-pcr test only finds non-specific pieces of RNA. It is therefore completely explainable that ‘regardless of the presenting symptom’, people are classified as covid-19, which is only a smokescreen clinical definition to hide the truth: there is no virus.
my previous question to people that disagree: prove that sars-cov-2 exists by showing 1 scientific paper.
That’s an interesting observation, Bart.
I’m no virologist but what diagnostic tests would you accept as confirming any other type of non-specific viral infection?
I imagine the usual tests for a positive confirmation such as Immunofluorescence or immunoperoxidase assays are not confirmatory for a variety of reasons to confirm sars-cov-2 exists.
Interested to read what others think.
My impression (which might be wrong – I am not a medical doctor) is that until very recently viral diseases were diagnosed on the basis of symptoms – not detecting the virus itself.
Detecting the virus by running a PCR test was just impractical until recently, and like all new tests, the initial question has to be whether testing positive actually predicts something. For example I have to wonder if those painful nose swabs were picking up viruses that had simply been breathed in, and were going to get desrtoyed by the body before they could do anything.
I think it is also important to remember that the test destroys the virus particles by breaking them open. It then tries to detect RNA with particular base sequences (via the RT-PCR process), supposedly found in CV-19 viruses. But since the virus was never purified, the sequences chosen for detection might have been simple human RNA.
Can someone correct me if any of this is wrong!
“Detecting the virus by running a PCR test” .. that sort of implies an intact, whole virus David;
the PCR test finds tiny, tiny fragments and multiplies them up; like the Sorcerer’s Apprentice; they could be anything
“But since the virus was never purified, the sequences chosen for detection might have been simple human RNA.” … that may well be: no-one is willing to be honest;
PCR testing goes back to the virus that was invented in the 1980s; Kary Mullis invented the technique and he was very critical of how it was used by those virus inventors;
“I have to wonder if those painful nose swabs were picking up viruses that had simply been breathed in, and were going to get destroyed by the body before they could do anything.”
…. absolutely: our immune system: we need to keep repeating this stuff, till we are blue in the face (as my mother used to say).
David, you can only develop a validated test if you have first purified a virus an characterized the RNA sequence via gelelectroforese. only the do you know the real sequence andere van develop the primers to copy parts of the sequence. then, when you validate the test you must check again by purification if the specific virus you are testing for is present. you also need to include control groups in each step to verify that what you are doing is actually a result of the experiment itself.
this offcourse has never been don with sars-cov-2.
Which brings into question whether viruses are the cause of a problem. A comparison might be “did the maggots on a corpse cause its death?” or “does the fire brigade cause fires?, since they seem to be there whenever there is a fire” Stephan Lanka’s research may provide answers.
https://www.globalresearch.ca/dr-stefan-lanka-2020-article-busts-virus-misconception/5719146
Have you noticed that whenever some strange phenomenon appears, there is a conspiracy there ready to explain it. Sinister, non?
Autre Temps, there couldn’t possibly be a conspiracy by, say, er, the Rothchilds since the 18th century to take over the world, and in the early 20th century get control of the US banking system by the setting up of the Federal Reserve, could there? That conspiracy is going on now.
dear David, I think you are right, but we should understand that pcr is a tool to manufacture a specific piece of DNA, you van only do this if you are designing tour primers based on the DNA that you want to copy.
Just imagine what would happen if you put an old primer in an unpure sample such as a nose swab. The primer will latch on to the first piece of RNA that matches, the enzyme finishes the DNA strand, and voila, you have a piece
of genetic material.
Then you publish this as a research paper in a famous medical journal such as nature or the lanced, NEJM etc. as having discovered a new infectious virus and you have created the start of a new epidemic and total world chaos.
But you know it is nonsense, and they know it is nonsense. But the rest doesn’t because they don’t actually read the paper so they would remain scared to death.
Pete Towshend used to sing of “see me, feel me, touch me, heal me …….” and Koch’s postulates were on that sort of track: the standards that were needed to verify a bacteria did what you said it did ……
……. since the virus was allowed to be invented in the 1980s with lesser criteria, virology has been let off the hook; bacteriology is the study of bacteria; they can be seen; grown; infect and isolated; virology is to bacteriology; as astrology is to astronomy some say ………. virology has some of the sense of cholesterol fever in the 1950s and onwards; fiercely held convictions; strong-arm tactics; compulsion (sorry, consensus); all the movement lacked were some background facts and substantiation …….
Another explanation is that the virus grew exponentially. One case in January could leans to everyone in Sweden being positive by March. That’s how exponential growth works.
This is something that worries me – something really goofy and/or sinister is happening.
In a way, I wish someone here was able to knock this idea down – but nobody seems to try much.
Have you come across Andrew Kaufman? He has a theory that seems plausible:
David
Thank you David. Horrifying but unfortunately in these days, believable. I shall never have another vaccine. Not for anything. We should learn from history that there will always be horrid people and the gullible populace they prey on.
Sinister.
Largely because the ‘Fact Checkers’ have lied so transparently to deny the GMOing potential of various of the DNA and RNA vaccines, that it must be true.
Whether the proposed vaccines already contain the contraceptive/sterilisation sequences and the CRISPA sequence to insert them remains to be proved.
And this one…
THE HORRORS OF THE COVID-19 VACCINES – DR CARRIE MADEJ
https://www.bitchute.com/video/habmX3cx9GwW/
Ha ha, that would be truly funny. And the vaccine will be even funnier!
“People came in with a nose bleed and they had COVID. They came in with stomach pain and they had COVID.”
Thus proving, of course, what a terrible virus it is – that has so many unpleasant side effects and consequences.
If someone goes to hospital with a heart attack, they will be tested for Covid-19; and if the test is positive – hey presto! Covid-19 causes heart attacks!
(My previous attempt at replying to this comment disappeared, so trying again)
Another explanation is that the virus demonstrated exponential growth, so say one case in Sweden in January would lead to millions of infections by March assuming an exponent of 2. That’s the nature of exponential growth.
With diseases exponential growth does not occur. otherwise everyone woukd have it in a very short time. There is always negative feedback because of people becoming immune.
Exponential growth did occur, COVID doubled every 2 to 3 days. In Scotland for example there was clear exponential growth which was hidden by the use of logarithmic scales in presentations. The numbers doubled every two days.
That’s why the disease seemed to come from nowhere, its growth was exponential. Look at the growth curves, the early slope is exponential, not linear. If you have 10,000 cases st the start of the week, you’re looking at 120,000 in a week, a million in 2 weeks.
Eventually, some sort of heard immunity will kick in or the vulnerable will die leading to a plateau or decline in growth but I’m only trying to explain the early growth and not having to resort to some conspiracy theory for an explanation.
“Exponential growth did occur, COVID doubled every 2 to 3 days. In Scotland for example there was clear exponential growth which was hidden by the use of logarithmic scales in presentations. The numbers doubled every two days”.
Where can we find the numbers demonstrating that, please? Obviously you can find a link or other reference easily enough, as you must have had the numbers by you when writing your comment.
Sure. Public Health Scotland publish this data both in a visual form and as raw JSON files. Start here: https://www.publichealthscotland.scot. You can interrogate the data as wish.
If the numbers doubled every two days, surely by now everyone in Scotland would have had it – and since not everyone in Scotland is dead and most would be unaware they had it, it must not be very serious.
20 days of doubling would give around a million cases, 30 days would give around a thousand million (billion to US readers). Looking at the Public Health Scotland raises questions How was the data recorded? What were the methods used to ascertain it was corona virus? There will be other questions, but the basic problem with data from a government agency it has been historically unreliable. Sorry about that watchingthestream, but why did the main peak in deaths come just after the UK lockdown? You may not have an answer, that is not a problem, it illustrates the problems with data and its use, or misuse. Did someone mention “Doctoring Data” ?
“20 days of doubling would give around a million cases, 30 days would give around a thousand million (billion to US readers).”
Correct.
Cases were doubling every 2 to 3 days. In Scotland we had I think 2 admissions in early March with COVID patients, by early April we had around 70. So that’s about 6 iterations and 2 raised to the power of 6 is 64. The graphed data describes an exponential function. If nothing had been done, then this exponential growth would have continued. Exponential growth is something you don’t want.
“Looking at the Public Health Scotland raises questions How was the data recorded?”
Hospital Admissions data.
“What were the methods used to ascertain it was corona virus?”
Clinical observation and diagnostic tests as is done with any patient. We try to see if there might be some other cause so the appropriate treatment can be used. It’s called medicine.
“There will be other questions, but the basic problem with data from a government agency it has been historically unreliable.”
Prove this.
“Sorry about that watchingthestream, but why did the main peak in deaths come just after the UK lockdown?”
Because deaths lag hospital admissions, we try not to kill our patients.
“You may not have an answer, that is not a problem, it illustrates the problems with data and its use, or misuse. Did someone mention “Doctoring Data” ?”
It illustrates the damage of unsubstantiated allegations to undermine data that doesn’t fit with your views.
Virus spread depends on a number of things and opportunity is a big one. By social distancing and restrictions on movement, the opportunity measured as the number of person to person infections dropped so the numbers began to decline. The infection rate would have increased exponentially without this until the herd immunity effect appeared or the vulnerable had died. No virus has ever infected 100% of a population as far as I know.
The virus’s natural reproduction rate is unchanged and you can’t change it.
As to whether you thing this is serious depends on whether you or someone close to you has had the disease. If you’re happy to kill off a high percentage of those over 75 then it’s not serious.
So if socila distancing and lockdown made all the difference, how come there is no real difference between outcomes in places that did and did not lockdown – except for their economies? The fact is that we don’t really know how infections spread (read Hope-simpson) and have no way to explain why some people get ill and others don’t – in the same family or workplace. More people die from road accidents, flu, TB and so on, so I’d say that CV19 is not serious for most people. If you need a test to know you have it and have no symptoms, it’s not a serious disease. There are apparently effective treatments that the NHS won’t use (presumably because they “under orders” to kill off the expensive elderly. I see no evidence that lockdown and distancing have helped anything except the very rich get richer while the rest of use can’t get proper health care or services (I’ve been waiting nearly 6 months for a working gas meter).
“If you need a test to know you have it and have no symptoms, it’s not a serious disease.”
Do you really believe this? Lots of serious problems are picked up early when there are no symptoms. Early detection is a good thing.
If the test was fit for purpose and reliable.
Yes, I really believe this. I suspect that the majority of people who currently test positive will either have no symptoms or nothing worse than a cold. Early detection often results in over- or unnecessary treatment and helps no one. Treat people with symptoms appropriately and safely and leave those with no symptoms alone. I’ve seen no real proof of asymptomatic transfer – in fact, I think we don’t have a clue about how diseases are spread but just look for anything that backs up the current view. To prove a hypothesis, you have to try to DISprove it first
A case of testing for a non-existent epidemic https://youtu.be/Pi5Go_LExWo
watchingthestream, you have nothing to back up a statement like that, otherwise how do you explain the figures from Sweden and from Dakota, both had low death figures, with no mandatory restrictions.
Have you ever been to the Dakotas? North or South? They are mostly empty and have one of the most brutal climates in the US. They are also extremely dry. During the summer, life is lived outdoors, Perhaps these are factors. Public transport almost doesn’t exist too.
For every Dakota is is a Hawaii where you can see three stages.
Strong exponential growth with possible superspreader events.
Lock down with travel restrictions and plateauing of numbers
Easing of lockdown, exponential growth in cases again across all the islands.
Hawaii is humid.
Read Edgar Hope-Simpson’s “The Transmission of Epidemic Influenza” These diseases always appeared to have come from nowhere, and have been doing it for hundreds of years. Since the growth phase appears to be about 20 days, then starts disappearing, the mention of exponential refers to a short transition, and I suspect is used to try and increase the drama.
An exponential function plots as a straight line on log-normal graph paper. So it looks like the general pattern is exponential growth for 20 days, peak and transition for 20 days, and exponential decline for 100-200 days. Of course, lots of real-world lumps and bumps on the way.
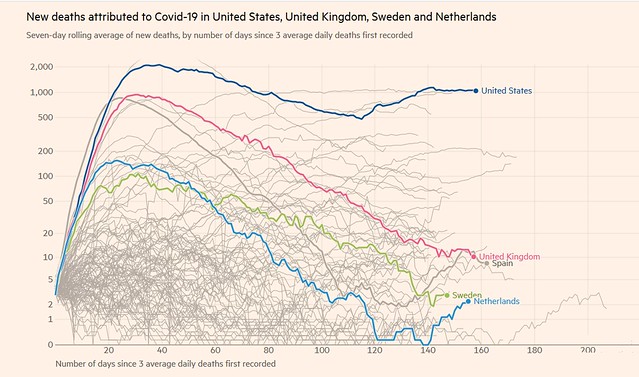
Martin,
The classic function describing how epidemics evolve over time is the Gompertz function. It has several parameters that can be used to fit the function to actual data. Michael Levitt (Nobel prize winner in Chemistry) has published a paper where he describes the mathematics to linearize the Gompertz function while estimating the function’s parameters. He has used his technique to estimate when the epidemic will have waned in the US.
https://www.medrxiv.org/content/10.1101/2020.06.26.20140814v2
Tom Morgan
Tom,
I know about Michael Levitt and the Gompertz function. What I am objecting to when use of the word “exponential” in its popular sense is considered reason enough to dismiss the argument.
If you listen to many medical staff, it waned long ago, and is only kept alive by using unreliable tests to claim increasing numbers of cases. Cases whiich in many instances didn’t even have symptoms.
As you are well aware, the press uses “exponential” as a synonym for “very fast”, not in the strict mathematical sense of the term. Similarly, when they say something was “decimated” they don’t mean 10% was destroyed, they mean the something was very substantially damaged.
If the virus was truly exponential the entire population of Earth would be infected by Day 33, assuming a doubling every day. Clearly this is not the case, but to a near approximation, in the early stages, for a short time, growth is exponential. To say otherwise is just nitpicking.
Martin, it is lack of nitpicking by people that has allowed the world to get into the current fiasco, where we have increasing cases and falling death rates, partly because the testing is near useless, and partly because the controlled MSM loves to lie about, it is beginning to seem, almost everything.
Rabbit population growth is exponential but the world isn’t covered in rabbits. Why not? Because as well as the growth driver there are breaks on growth. For example a strong break is susceptibility. Initially everyone is susceptible as it’s a new virus but this decreases as immunity builds leading to the infamous herd immunity level.
Coming back to rabbits, Australia was essentially covered in rabbits at one time because of exponential growth and the lack of natural breaks on growth.
I think your comment on journalists’ understanding of exponential is bang on. And I think the quality of journalism is abysmal.
a case does not mean somebody is infected, the case dedinition is separated from the virus so that they can create the illusion of an epidemic without actually proving people are infected.
It is their trick, their scam. separate the clinical definition of a case (covid19) from the virus (SARS-CoV-2) and fake an epidemic.
Testing – as a couple of posts don’t seem to have ‘gone through’…
I tried to share the link to the world premiere of a documentary showing another side of the Covid story, but I think it may be being censored. Here is is again – but replace the “space DOT space” just with a dot, removing the spaces, as the site censors won’t let me post it:
https://freedomplatform DOT tv/plandemic-indoctornation-world-premiere/
Bart,
You make an interesting observation. It seems to me the basic argument is that we don’t understand viruses, and we can’t isolate them, therefore they do not exist.
I’ve had enough colds and flus to know something exists, and if my wife is sick, I will probably get it from her. Clearly people are getting sick from this, and as Malcolm has pointed out from his personal experience, the clinical symptoms are very different than a typical flu.
Sadly, those in power have banned all effective treatments that would make this a non issue, as we wait to lubricate their greedy palms with trillions of our dollars for their promised franken-vaccine.
Dr John H,
I think if you want to get some idea of the potential issues around viruses, a good place to start is with Henry Bauer:
https://thecaseagainsthiv.net/
You don’t have to accept his theory about the HIV virus to see where a lot of the potential for confusion can come from. There seem to me to be a lot of parallels with CV-19. In the case of AIDS, there was never a formal scientific paper claiming to have proved that HIV causes AIDS – it just became common knowledge. Likewise (at least HB claims) the HIV virus was never purified. Also there were always other possible explanations for AIDS type symptoms – such as fungal infections, but suddenly they lasered in on this one virus.
There is no equivalent of the Petri dish when you are growing viruses. You need a cell culture that you inoculate with the virus in question. However that immediately contaminates the virus, so for example RNA or DNA (depending on the type of virus) may come from the virus or the cells on which it grows.
HB points out that many of the AIDS drugs happen to work against fungal infections, but they are too toxic to be used in this way normally – so do people appear to recover because of this anti-fungal effect?
Obviously that is just what I understand from reading his side of the story – I’m not claiming anything from personal knowledge.
dear John,
I am not denying however that people get sick and die, this is just a fact.
But, how can you know that you are getting sick of a virus, if there is no proof that it actually exists?
Maybe it would be better to turn it around and look for another cause that a virus. There is not any cure for it anyway, assuming that you would believe it exists. Which I don’t, perhaps low vit D levels are a cause? maybe soms toxicity? maybe the yearly flueshot (of which it has also not been proven to exist).
Bart,
I know that a few viruses can be crystallised – notably tobacco mosaic virus – but I wonder if RNA viruses are more difficult to crystallise because the RNA molecule is more floppy.
Do you know of any other way than crystallisation to satisfactorily purify viruses ?
Airports and flying constitute a dangerously narrow congested “tunnel” that is necessary to get from one reasonably safe place to another safe but distant one. Worth it? Or maybe you don’t believe it, in which case, you’re safe?
https://www.medpagetoday.com/infectiousdisease/covid19/88131?xid=nl_covidupdate_2020-08-19&eun=g42415d0r&utm_source=Sailthru&utm_medium=email&utm_campaign=DailyUpdate_081820&utm_term=NL_Daily_Breaking_News_Active
It’s nonsense, I’m safe, so is almost everyone else, pure unadulterated fear mongering.
AhN always brings this to mind, for some reason:
“I beseech you, in the bowels of Christ, think it possible you may be mistaken.”
“The quotation is, of course, from the well-known remark of Oliver Cromwell, urging the mule-headed General Assembly of the Church of Scotland to repudiate their allegiance to the crown, i.e., to Charles II. Cromwell, mule-headed himself, made his famous plea: “I beseech you, in the bowels of Christ, think it possible you may be mistaken”.
History is full of those who were wrongly sure of themselves, to the point where we suspect that anyone who is completely sure is never quite right. Many religious groups have been “sure” that “others” were wrong, and have used force to convert them. Within Christianity, Roman Catholics have burned heretical Protestants at the stake, and vice versa, and so on.
Not only in religion do we find this, but in political life as well. Communists have forced their ways on society, as did the Nazis. None of all this made many true converts, or proved who was right. Sports and styles offer more examples, without the violence, mostly.
If we search for reasons for all this, we find ourselves considering, again, the biological need to belong, preferably to those whose appearance, language or geographical origins are similar to ours. We are uneasy being alone. It all seems as simple as that. So much for freedom.”
– Donald Crowdis –
“Communists have forced their ways on society, as did the Nazis.”
Not exactly, because the people wanted the changes. And now we have people desperate for vaccines. Most won’t feel coerced at all. So much for freedom indeed.
Most of us follow this blog for information, not because we need to belong. The cholesterol wrongs are so serious that a united front against them is desirable. This obvious con warns us, as does history, of the possibility of further outrages.
We have 3 options:
We can join the crowd
We can seek information and share our thoughts
We can bury our heads in the sand
Any certainty shown by contributors to this blog pales into insignificance when compared to the strength of it in the media, government and general public.
Tish,
I don’t think people wanted the changes wrought by communist or fascist revolutions. It takes a small number of dedicated and paid revolutionaries to accomplish it. That is why I am so worried about the Marxism and violence that suddenly seems to be everywhere in the US, including in most of the Democrats running for president or speaking at the convention.
P.S. Any uncertainty shown by governments, e.g. “We don’t know enough yet, it’s a new thing….We have changed our minds, we are learning more about this dreadful thing…” serves to increase fear. Whether this is a deliberate approach to suggest a lack of control or simply represents bungling and ignorance I wouldn’t like to say, but it certainly creates the response they seem to favour. Remember the early phrases repeated ad nauseam? Nobody should doubt the motive there, surely.
All these nice comments on my Donald Crowdis quote above completely miss the salient point. I could not possibly care less about politics or what governments decide to do, as discussed here.
I comport myself according to what I think is the best, most reliable Scientific/Medical information I can find, having done the time and labor intensive search as best I can. Harp on as much as you like about your governments and their toadies, amongst yourselves.
This is the point:
“History is full of those who were wrongly sure of themselves, to the point where we suspect that anyone who is completely sure is never quite right.” “If we search for reasons for all this, we find ourselves considering, again, the biological need to belong, preferably to those whose appearance, language or geographical origins are similar to ours. We are uneasy being alone. It all seems as simple as that. So much for freedom.”
No one has criticized this. An interesting Freudian oversight? Look to yourselves.
JDP, ditto.
J.D.P wrote:
“I could not possibly care less about politics or what governments decide to do, as discussed here.”
Fine – but if you are talking about medicine, you need to ask yourself if the data and theories you read about are equally untainted by politics or money – or indeed any other motive that is not directed at making people well again.
On the one hand we have the old people in care homes, cruelly starved of contact with family and friends, and on the other, there is a very real concern for children. Young parents are far too busy to properly analyse information on vaccines and just assume they are o.k. Grandparents who are fearful for the children are limited in their influence against all the dreadful propaganda and censorship. It is truly sickening.
From The Fat Emperor (Ivor Cummins) a video https://youtu.be/SwlkumcRf6w. An example of how the MSM tries to twist the data to fit their paymasters’ agenda, while someone who sees the situation daily is harangued. It is in Spanish, and you will have to read fast to keep up with the English subtitles. Note the mention of lockdown in September………………..
Can we rely on any figures around the world for this virus?
Hospital coronavirus admissions were over-reported at peak of pandemic | Daily Mail Online
https://www.dailymail.co.uk/news/article-8650163/Hospital-coronavirus-admissions-reported-peak-pandemic.html
So… The way that the ONS records “COVID-19 mortality” is less than useless: https://www.ons.gov.uk/aboutus/transparencyandgovernance/freedomofinformationfoi/breakdownofcovid19deathdatabyu071andu072codesincludinginformationregardinghowthepatientwasdiagnosed
An interesting study from Scotland ….”Associations of severe COVID-19 with polypharmacy in the REACT-SCOT case-control study”
“Conclusions — Severe COVID-19 is associated with polypharmacy and with drugs that cause sedation, respiratory depression or dyskinesia, have anticholinergic effects or affect the gastrointestinal system. These associations are not easily explained by co-morbidity. Although the evidence for causality is not conclusive, these results support existing guidance on reducing overprescribing of these drug classes and limiting inappropriate polypharmacy as a potential means of reducing COVID-19 risk.”
Its a very strange health system that wont prescribe or even recommend vitamin D despite the evidence that it is so important for the immune system, yet will happily prescribe a cocktail of drugs that are known to have side effects.
https://www.madinamerica.com/2020/08/antipsychotics-associated-severe-covid-19-fatal-outcomes/?fbclid=IwAR0UkRu9dM0607HvxKEIufQ7y3oMwQDmVWXzqPjMIUo24sfGD2-SLaeR1sg
I’d like to ask people what you think the following thought experiment might produce.
Imagine a psychological experiment in which a new disease was invented and the medical profession was persuaded to go along with the fiction and put out increasingly alarming messages including the idea that it would be necessary to make enormous sacrifices and give up so much of what it is to be human simply to stay alive – and even then you would have to cross your fingers.
As part of the experiment, every place you turned – radio, television, the internet would also push the same message.
Given what you know of nocebo effects and people’s varying suggestibility, what fraction of the population would you sicken, and how many would die – without any objective virus?
Shouldn’t this baseline be subtracted off all the COVID figures?
On reflection, I guess this experiment could be really tested in a weaker form in the form of virtual reality. I’d guess it would make some ‘players’ decidedly unwell.
David Bailey: I’ve been thinking of nocebo effects too, but also from an anthropological perspective. Anthropologists and colonial memoirists (e.g. Elspeth Huxley) well document the effect on people who discover that someone has laid a curse on them. It is a supreme method of socio-psychological control. It often begins with a preliminary warning that it will be laid. No amount of rationalising will effect a remedy: the victim surrenders themselves to death unless some more powerful agency can counter with means whereby the cursed can make restitution to the curse-layer.
Courtesy of the unrelenting MSM hysterics/images from Wuhan, and WHO pronouncements of ‘PANDEMIC!’ it seems to me that the equivalent of a curse was laid. I thought this again recently when the whistle-blowing nurse at the New York hospital described how in the early days of the pandemic she saw patients arriving with breathing problems who were immediately put on ventilators when in her opinion they were suffering from anxiety attacks. Given endemic levels of anxiety in industrial populations, one cannot help but wonder: how many of the fatalities surrendered to the ‘laying of a curse’.
I so agree Tish. Those of us who think we got the virus before it was named probably did a lot better.
Yes. I think I had it too, and quite failed to infect nearest and dearest.
Tish – I totally agree. For my husband and me it was ‘just’ a nasty chest infection. Had it, recovered, forgot about it. (It’s taken this long though to regain a sense of smell. Our garden has been very dull.)
Have you watched the Event 201 videos?
Check out Segment 4 for example, re ‘communications’ https://www.centerforhealthsecurity.org/event201/videos.html
Stepping out beyond you area of training/expertise – An electrophysiology cardiologist:
https://www.drjohnm.org/2020/08/doctoring-and-activism/
Regarding the complete ‘Horlicks’ that the UK Gov is making of travel related quarantine, my son returned to Germany on Saturday evening and was tested at the airport then received the result by email this morning (Monday). How simple is that?
What is wrong with our Government?
Meme Machines. Spreading scurrilous crap. And yes, some of you know who you are: https://www.bellingcat.com/news/2020/08/21/who-director-general-attacked-on-twitter-with-ccp-related-memes/
Attn:Dr. Kendrick,
Right up your alley:
The glycocalyx and COVID-19:
https://t.co/QlJ3DVe9tB?amp=1
Thanks, read it. Pretty much confirms my thinking. COVID seriously damages the glycocalyx, possibly due to underlying endothelial cell dysfunction. I think my new theory is, remove the O and I, and you turn COVID into CVD. Although I am not entirely sure this is a fully worked up theory.
https://youtu.be/FU3OibcindQ Ivor Cummins explains the current casedemic which is being interpreted by the tyrants as an excuse to quarantine holidaymakers who fail to get back home by 4 a.m. Saturday morning.
Mark Woolhouse said lockdown was a monumental mistake, but for those affected by these moron inflicted quarantines, it’s still a lockdown. The opposition will no doubt play the semantics game to explain how these mini-panics are a vital health measure. https://lichtnahrung2015.wordpress.com/2020/08/24/the-coronavirus-lockdown-was-a-panic-measure-and-a-monumental-mistake-on-a-global-scale/
Simple & Fantastic COVID Treatment flow chart:
Click to access Marik-Covid-Protocol-Summary.pdf
The new P1andemic: Inductrination movie is out, and it’s great! It follows the money – Gates, Fauci etc. I intentionally misspelled the title as previous attempts at posting here were caught by censors. Go to https://londonreal.tv/
How are Melbourne people on this blog thread going? With Dictator Dan Andrews, sorry Premier, seeking to extend emergency powers for up to another 12 months lockdown?
I’m horrified by what is going on in Australia. How many other countries in the world have forbidden their citizens the freedom to leave without special dispensation. We can’t even move around the country freely.
We’re under the tyranny of the unelected Federal and State medical officers, I’m really gobsmacked by the current situation.
I hear they’re pushing masks for children now, what do you think about this?
Advice on the use of masks for children in the community in the context of COVID-19
https://apps.who.int/iris/rest/bitstreams/1296520/retrieve
Yes, and more young children seem to be wearing masks Elizabeth, almost like fashion accessories. The very suggestion is appalling. Parents have to be really brainwashed to allow it.
This could be the explanation!
Doctors challenging the covid narrative, a recent conference in Hungary:
https://www.xn--rzte-fr-aufklrung-pqbn68b.de/informationen/aktuelles/
Also German doctors: The Covid 19 extra parliamentary investigation committee:
There are English versions on their site: https://acu2020.org/english-versions/
Perhaps this might explain the different transmission rates being observed using Austria & the US as examples. A threshold and network topology effect. The math(s) seem to work.
https://medicalxpress.com/news/2020-08-covid-infection-unexpectedly.html
I’ll have a read of that, thanks, a link would be appreciated. There is an aphorism by an expert in this field called George Box that says “All models are wrong, but some are useful”.
The assumptions made back in March were based on data mainly from China and some from Italy as that was what was available at the time.
Having looked at the code myself, I would have made exactly the opposite conclusion to the report you cite, the model is way too complicated and is a bit baroque. However, as George Box would have said was it useful? That’s the key thing. Its predictions matched the formulae that I think you pointed out in an earlier post but I’d regard that was a good thing. Models are supposed to match to increase confidence that they are right.
I find the lack of a test framework in the code alarming but again, is the model useful? That’s the key question.
This carefully choreographed vilification of Prof Ferguson does bother me and I really wonder who decided to pick Neil as the fall guy. That report from some anonymous person from Google criticising the code seems to be part of this plot. Perhaps there’s a conspiracy here.
Carefully choreographed. Interested concept, and who do you think choreographed me? Ferguson’s model was a guess, based on key parameters that were wrong. The IFR he used was 0.9%, the current IFR in Iceland (most tested population in the world )is 0.16% – out by a factor of 5. He has form in wildly overestimating deaths. He picked himself as the fall guy. He was the ‘face’ of the Imperial College Model. His model, and others based on it, have lead to an enormously destructive lock down that was, in my opinion, completely unnecessary and has caused many tens of thousands of deaths. I am sure the model was very useful – for certain people.
The model was used as a tool to justify a lockdown, then found to be a mistake https://www.redstate.com/michael_thau/2020/08/24/lockdown-monumental-mistake-%e2%80%93-must-not-happen-again-says-top-uk-epidemiologistcovid-advisor/
The mistakes continue with all the social isolation dictates (which I ignore as much as possible).
Watching the stream
About Prof Ferguson, I said at the time that It seemed very convenient that there was an anonymous rubbishing of the code, and the outing of his extra marital adventures, when he had become surplus to requirements and a very convenient fall guy. I noticed that on this blog many commenters have taken up this theme, so that was successful.
As to thé model, it was pointed out that there are technical reasons for some of the alleged faults.
As for models, as a former finance director, I always found forecasting extremely hard, but, as you say, a model teaches you an awful lot. If politicians did not understand the limitations, well what can anyone do? I am surprised that the acting prime minister D Cummings didn’t understand that since he is said to obsessed with data handling. Or perhaps he did.
At a guess, you read this in the English media. There are some telltales in this Ferguson story. The necessary ingredients are
1. Refer to him as Ferguson or some nick name
2. Pick him out amongst all the other advisors
3. Express moral outrage that he met a “married lover” and never question how anybody ever found out.
4. Incorrectly sling mud at the code by citing some anonymous author from Google.
5. Say something like “He’s got a patchy history in predictions”. With no evidence of course.
In Scotland, there are at least 4 models being used including Imperial’s but the others are never picked out. The others are from Warwick, LSHTM, Manchester. Are these other models perfect? Why still use Imperial’s if it’s so bad?
Margaret Thatcher once said that “Advisor advise, ministers decide”. Prof Ferguson oh sorry, I went off script there, the Fergoid was one of many advsors so again why pick him? This was a government decision and I strongly suspect the government is cynically shifting the blame. And it’s odd that almost every European government made the same choice without Ferguson.
The Iceland numbers were not available in March.
The Imperial Group did a really brave thing by open sourcing their code for anybody to download and look at and I think they should be congratulated for doing this not vilified. I wish other teams were less coy with their data and followed Ben Goldacre’s open approach.
Watching t s – In whose interest would such a campaign be in & who might fund it ? Large swathes of largesse is swilling about right now from billionaires and one in particular. Could he, the one identified in an independent journal be responsible ?
https://www.cjr.org/criticism/gates-foundation-journalism-funding.php
The plot thickens !
Whatever do you mean by “patchy history with no evidence”? There’s plenty of evidence, foot and mouth (another manufactured plague), association with Roy Anderson, BSE, swine flu. the last two predicted to kill huge numbers. And the UK government bought loads of Tamiflu on the strength of the predictions.
“1. Refer to him as Ferguson or some nick name
2. Pick him out amongst all the other advisors
3. Express moral outrage that he met a “married lover” and never question how anybody ever found out.
4. Incorrectly sling mud at the code by citing some anonymous author from Google.
5. Say something like “He’s got a patchy history in predictions”. With no evidence of course. ”
1. Eh? his name IS Ferguson. What else would you call him When I was a Oxford, we referred to the teaching staff by their last names. I doubt Imperial is any different.
2. No, we hate Cummings as well. We don’t pick and choose.
3. I don’t give a toss who he met. Although the fact that he broke a lockdown that followied his own recomendations suggests that he didn’t believe his own predictions.
4. So you don’t a) think people would be allowed to be anonymous and b) that code for this sort of model should produce the same result for the same inputs? Fine. I wish I could run tax software multiple times until it gave me ” tax refund due”
5. He hasn’t got patchy history with predictions – he’s always reliably wrong! Evidence was cited but you ignored it. I don’t think all tahat mnay cows were killed in 1967 – wej ust spent a lot of time trudging through trays of disinfectant (but perhaps you are not old enough to remember). Certainly no heaps of burning cows in fields near schools
You obviously inhabit a different universe from me.
“That code for this sort of model should produce the same result for the same inputs? Fine. I wish I could run tax software multiple times until it gave me ” tax refund due””
These models try to model human behaviour which is basically random and to try to represent this, the code uses some source of randomness. So every time you run the model, you get a different result but that’s because some choice was made that was different to the previous run. Human behaviour is random. Someone took the bus rather than drive for example.
However, the models are run again and again to get a range of outcomes and, fingers crossed, some result will turn our to be by far and away the most likely. Sometimes this doesn’t happen.
With your tax code, there is no randomness, it’s a straightforward calculation.
With the same inputs, code will always produce the same results. But to artificially model something random, you have to program in a pseudorandom source.
An excellent analysis/evaluation of the present situation. If only the majority of the world population could read and understand what is said here, an essential change in direction can be made in order to avoid disaster here on Earth. We should have followed Sweden’s common sense strategy.
Thank you.
Ivermectin is used against parasite diseases all over the world. Someone has probably been cured of one of these parasite diseases and been cured of the Corona virus at the same time because of WHO or FDA the one cure is an fortunant accident and the other is business as usual for the drug ivermectin.I hope such a case comes to light before more people die from Corona
this didn’t age well…..