Stress/strain
When I started looking at cardiovascular disease I wondered why French people suffered far less than the Scots. I concluded, somewhat prematurely, that it was because the French ate food in a completely different way. They ate slowly, with the family, and food was an important part of life. Whereas, in Scotland, food was to be endured, not enjoyed. As scientific proof I would present Bovril and mince pie, at half time, at a Scottish football match.
When the French ate it was slowly, in a relaxed fashion. This allowed all the stress hormones, and all the nervous system involved in ‘flight or fight’ to settle down. So the French could digest and absorb food properly. Sugar levels would not spike; insulin would not spike. We would not have a battleground of cortisol and glucagon vs. insulin, and suchlike. Many animals after they have eaten simply find somewhere to go to sleep, to digest. Many humans just keep rushing about. Fast food indeed.
This brought me to led me to look at the overall concept of ‘stress’ in far more detail. Years and years later I have emerged – at times more confused than when I started. In the process I have fully embraced Einstein’s view that ‘Not everything that counts can be counted, and not everything that can be counted counts.’ I prefer it in the version. ‘Most things that can be measured don’t matter, and most things that matter cannot be measured.’ At one point this was my screensaver.
Stress fits well into this view of measurment. Stress certainly exists. Or perhaps to be more accurate ‘strain’ exists. In fact, both things exist, but measuring them… well, that it a trickier task. Which is one reason why medicine, obsessed as it is with ‘that which can be easily measured’, has tended to dismiss stress as a cause of anything. Focussing instead on blood pressure and cholesterol levels and blood sugar levels, and suchlike.
One thing I think I need to add at this point is to say that people do not actually suffer from stress, they suffer from strain. A subtle, but important difference. In that, two people can suffer exactly the same stress/stressor, yet react completely differently. One may feel strain, the other may not.
If, for example, two people are asked to stand up in front on an audience and give a talk. One person may dread this, the other may love the opportunity. They are both exposed to precisely same stressor, but the strains on the individual are diametrically opposed.
Extending this thinking somewhat, it became clear that stress, if indeed we should use this word at all, needs to be differentiated into, at least, four parts.
- Positive stressor
- Negative stressor
- Positive strain
- Negative strain
Of course, it gets even more complicated than this. We have short term and long term stressors. We have individual resilience, and suchlike. A person feeling strong fit and well may deal with a stressor well one day, yet when feeling physically ill, may be unable to cope with exactly the same stressor.
What mattered, I came to recognise, was not to get hung up on individual stressors, but to look at how the body adapts to different forms of external stress. It is impossible to look at someone’s lifestyle and say ‘they must under huge stress.’ Well, maybe they are, but maybe they treat it all in a positive way and it has beneficial effects on them.
I remember a cardiologist reviewing a lady who lived in the countryside, surrounded by a flower filled garden, with no money worries etc. He remarked ‘Well, stress obviously cannot have contributed to her heart attack.’ I merely nodded and thought to myself. ‘How can you possibly know? Perhaps her husband is horrible to her every day, and bullies her. Perhaps she yearns for another life.’
Of course, if you cannot measure strain, then the discussion does become rather pointless. ‘Anyone who has heart disease must suffer from strain, because strain is the cause of cardiovascular disease.’ This would be one of Popper’s circular arguments. A statement that relies on itself to prove itself. Similar to the argument used when a young person, with no traditional risk factors for heart disease has a heart attack. ‘Oh, it must be genetic.’
‘How do you know it is genetic?’
‘Well, they have no risk factors, and had a heart attack, so it must be genetic.’
Yes, indeed, it must be genetic… not. Try again, you idiot.
So, my attention inevitably became drawn to two researchers. Sapolsky and Bjorntorp. Sapolsky has studied baboons for many, many, years. He found that Baboons were pretty similar to humans in social structures, also in being perfectly horrible to each other, battling to gain higher status, bullying weaker members, and suchlike.
However, life in a Baboon troop normally muddles along quite well, but when the social hierarchy is disrupted by a new alpha male trying to take control of the group, there is a massive rise in cortisol levels, and a subsequent fall in white blood cells in all the baboons. Both of these are very significant signs of strain. You can look up Sapolsky on Google, he is a very entertaining lecturer and writer. His best known book is ‘Why Zebras don’t get ulcers.’
But, of course, Baboons are baboons. Humans are humans. Which is where Bjorntorp comes in. He wanted to know If strain, in humans, could be measured objectively [He called strain stress – as does everyone except me]. He found that it could indeed be measured by looking for a dysfunction of the Hypothalamic Pituitary Adrenal axis (the HPA-axis).
The HPA-axis is an extraordinarily complex physiological system that co-ordinates our responses to external stimuli – both negative and positive. If a lion were to walk into your room, right now, the HPA-axis would do its thing, and trigger the flight or fight response. [I would recommend flight]
The main hormones involved in flight and fight are: cortisol, glucagon, adrenaline (epinephrine) and growth hormone. The sympathetic nervous system response acts alongside the hormones. In a situation that triggers fear, the sympathetic nervous system lights up. This raise heart rate, pushes blood to muscles, and suchlike. Of course, at the same time, the stress hormones make the blood hyper-coagulable (far more likely to clot). You don’t want to bleed in a fight.
Anyway, Bjorntorp decided to measure twenty-four-hour cortisol secretion, in different populations. By this I mean he looked at what happened to cortisol levels every hour (or half hour) during the day. A normal cortisol secretion rises in the morning, goes down, rises at lunch, goes down and up quite a lot for the rest of the day. It is, basically, flexible.
An unhealthy cortisol secretion is more of a flat line. It does not peak in the morning, then it does not fall so much. He described this pattern as a ‘burnt-out’ HPA-axis. The hypothesis being that if someone is exposed to repeated activation of the HPA-axis it eventually becomes unable to cope. The system becomes damaged/inflexible.
This is similar to many other conditions whereby a ‘flattening out’ of normal responsiveness is a sign of significant physiological damage. [See under fetal heart monitoring, or the final development of type 2 diabetes].
As a quick aside, I should add that [inevitably and depressingly], a number or researchers have decided to measure cortisol levels in the morning to look for signs of stress/strain. They found a low level, in those with cardiovascular disease, and concluded that stress has nothing to do with cardiovascular disease, because the people they looked at had low morning cortisol levels. Ho hum.
Back to Bjorntorp. Here is the abstract from his paper ‘The metabolic syndrome–a neuroendocrine disorder?’
‘Central obesity is a powerful predictor for disease. By utilizing salivary cortisol measurements throughout the day, it has now been possible to show on a population basis that perceived stress-related cortisol secretion frequently is elevated in this condition. This is followed by insulin resistance, central accumulation of body fat, dyslipidaemia and hypertension (the metabolic syndrome).
Socio-economic and psychosocial handicaps are probably central inducers of hyperactivity of the hypothalamic-pituitary adrenal (HPA) axis. Alcohol, smoking and traits of psychiatric disease are also involved. In a minor part of the population a dysregulated, depressed function of the HPA axis is present, associated with low secretion of sex steroid and growth hormones, and increased activity of the sympathetic nervous system.
This condition is followed by consistent abnormalities indicating the metabolic syndrome. Such ‘burned-out’ function of the HPA axis has previously been seen in subjects exposed to environmental stress of long duration. The feedback control of the HPA axis by central glucocorticoid receptors (GR) seems inefficient, associated with a polymorphism in the 5′ end of the GR gene locus. Homozygotes constitute about 14% of Swedish men (women to be examined). Such men have a poorly controlled cortisol secretion, abdominal obesity, insulin resistance and hypertension.
Furthermore, polymorphisms have been identified in the regulatory domain of the GR gene that are associated with elevated cortisol secretion; polymorphisms in dopamine and leptin receptor genes are associated with sympathetic nervous system activity, with elevated and low blood pressure, respectively. These results suggest a complex neuroendocrine background to the metabolic syndrome, where the kinetics of the regulation of the HPA axis play a central role.’ 1
In short. If you are exposed to constant negative stressors, you are likely to burn out your HPA-axis, you will end up with abnormal cortisol secretion, and suchlike. You will then develop central obesity, high blood pressure, high VLDL levels, low HDL levels, high levels of fibrinogen, and many other clotting factors.
For those of you who have been paying attention to this series up to now. All of these things will increase endothelial damage, stimulate blood clotting and impair the repair systems.
For many years I knew that ‘stress’ was a very important factor in increasing CVD risk. All the evidence supported this, no evidence (other than people who failed to understand how strain affects cortisol secretion in the morning) contradicted it.
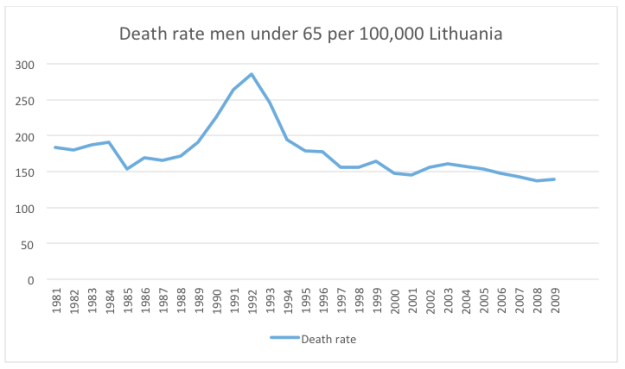
Which is where I return to my earlier graph on the rate of CHD in Lithuania in men under 65. As you can see, it was falling from 1981 to 1989, at which point it spiked, returning to its point of decline about eight years later.
Exactly the same pattern can be seen in Latvia

Here, I think we see Sapolsky’s work on Baboons, mirrored in humans, and mirrored in two countries that lie side by side, next to Russia. In 1989 the Berlin wall fell, the Soviet Union collapsed, the established social hierarchies disintegrated. Strain rose dramatically, and so did the rate of CHD.
This affected various Soviet Union states in slightly different ways. Poland, which had gone through the strikes and the battles of Solidarity years earlier, was very little affected in 1989, but the same basic pattern can be seen. In Belarus CHD skyrocketed, and has stayed very high [Belarus is the only dictatorship left in Europe]. In 1981 the rate of CHD in Belarus was 137/100,000 per year. In 2009, the last year with published data, it was 213. The Ukraine, and Russia also remain very high, both at 186.
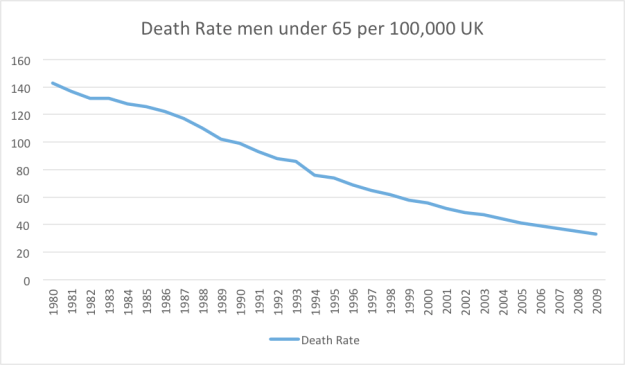
During the same period, in Western Europe, absolutely nothing happened to CHD rates other than a slow and steady decline in all countries, year on year. The UK has gone from 143 to 33. Austria 83 to 29. Italy 62 to 19. France 39 to 15 etc.
I do not wish to hark back to a subject that I have previously covered. However, I can think of no other possible explanation for the rise in CHD in all ex-soviet countries after 1989 than the fact that there was a tremendous social upheaval, creating enormous strain. This signal is extremely strong and the data are remarkably consistent.
Data that links the work of Sapolsky and Bjorntorp who, in my opinion, ought to be recognised as the man who established, beyond doubt, how negative stressors can create measurable dysfunction of the HPA-axis which leads, in turn, to the metabolic problems that cause CHD. Or, to put it more simply. How stress causes heart disease. [No, it is not the only cause, but it is probably the most important single cause].