How is medical data presented to the public?
17 Replies

We are told, ad-nauseam, that obesity is the main cause of type II diabetes. This, allegedly, follows a very simple causal chain.
Obesity > insulin resistance > raised blood sugar levels
For those not familiar with the term Insulin resistance, this is the condition whereby various organs in the body become gradually more insensitive to insulin, which forces insulin levels higher to keep the blood sugar levels down.
Eventually the resistance to insulin becomes so great that the blood sugar levels rise anyway – despite the high insulin levels. Alternatively, or in parallel, the pancreas gives up fighting against the resistance and insulin production becomes ‘burnt-out’. Whichever process is dominant, they both result in sugar levels become very high, and you will be diagnosed with type II diabetes.
At this point I have to state that I have always found it weird that a raised blood sugar level can be defined as a disease, when it is clearly nothing of the sort. In my world a ‘disease’ is the underlying malfunction which causes various signs and symptoms to occur (of which a raised blood sugar level would be one).
Everyone agrees that insulin resistance is the basic underlying cause of a raised blood sugar level a.k.a. type II diabetes. Despite this we define the blood sugar level itself as the disease.
‘A high blood sugar level is type II diabetes….end of.’
‘So, if we lower the sugar level, we have cured the disease?’
‘Yes. Now do shut up.’
Clearly bonkers, but let us not expect too much in the way of logic in medicine. Anyway, that is a slight distraction from the main theme here, which is the: obesity > insulin resistance > raised blood sugar levels discussion.
Now, for reasons that I am not going to fully bore you with here (but maybe at a later date), I have always had problems with this causal chain. Primarily, that it has never made much sense to me. Insulin resistance occurs almost exclusively in two tissues; the liver and skeletal muscle, and NOT in adipose tissue. So why would having too much adipose tissue make you insulin resistant? Answers on a post-card please*.
In order to pursue this thought further I started to look at evidence from Sumo Wrestlers. These are the most obese people on the planet. At least they are if you use BMI to define obesity. Yet, none of them have type II diabetes (at least not, whilst in training). For example:
‘Abnormally large waist circumferences, which were determined by the criteria established by the Japanese Society of Internal Medicine, were present in all Sumo wrestlers (100%), and fifteen Sumo wrestlers (83%) had high abdominal visceral fat areas (>100cm2). Only 2 subjects were categorized with high serum triglyceride levels, and 5 subjects were classified with low HDL-C levels by established criteria. None of the Sumo wrestlers had fasting hyperglycemia (high blood sugar levels) (0%)’1
Interesting, is it not, that the most obese people on the planet do not have type II diabetes (although some of them have a degree of insulin resistance – for reasons that I may explain at a later date). Yes, I know exactly what you are now thinking. They do not have diabetes because they exercise a lot. It’s true, they do. But does that not make it more likely that a lack of exercise is the true of cause of insulin resistance, rather than obesity….yes, of course it could certainly mean that.
In truth, finding very obese people without diabetes does not rule out obesity as the cause of diabetes. But it does rule out obesity as being both ‘necessary’ and ‘sufficient’. At this point I need to explain the concept of necessary and/or sufficient.
It was Koch who first tried to determine a process of logic to describe whether or not something may be a true cause of a disease, or just a chance association. He introduced us to Koch’s postulates, and also the concept of necessary and/or sufficient.
For example, it is known that the bacteria vibrio cholarea causes cholera. In order to get all the signs and symptoms of cholera it is ‘necessary’ to be infected with this organism. However, infection with vibrio cholarea does not cause cholera in everyone. If you are a fit and healthy adult you can shrug off the infection with only mild symptoms. Koch proved this by drinking a glass of water known to be infected with vibrio cholarea and developing only mild symptoms of the disease
Thus it can be stated therefore that infection with vibrio cholarea is ‘necessary’ to cause cholera. However it is not, on its own, ‘sufficient.’ Other factors are needed. On the other hand, if you could find people with cholera who had not been infected with vibrio cholarea, then you would have to declare that vibrio cholarea was neither necessary, nor sufficient, to cause cholera. So it could NOT be the cause of cholera.
This is obvious, and inarguable.
So, moving back to type II diabetes. Can you find people with type II diabetes who are of normal weight? Or, to stretch this concept to the limit, can you find people with type II diabetes who have no adipose tissue at all? Surely not, you say. Surely impossible.
At this point I shall introduce you to ‘Berardinelli-Seip Congenital Lipodystrophy’. This condition affects about one in ten million people. So it is hardly common, but that is not the point. The point is that the primary abnormality in Berardinelli-Seip Congenital Lipodystrophy is a lack of functional adipocytes – which means that those who suffer from this condition do not have fat cells, and cannot store fat. Ergo, that they are extremely lean. The leanest of the lean, the least obese of the least obese.
From time to time I describe this condition to doctors. At which point I somewhat cheekily ask them to guess what percentage of people with Berardinelli-Seip Congenital Lipodystrophy have type II diabetes. I say cheekily, because they inevitably get the answer wrong. They always, without exception, answer pretty much as follows:
‘Obviously, none of them.’
The correct answer is, of course, ‘Every… single…one…of…them.’ [Gasp, sounds of people collapsing to the floor in shock etc.]
Now, if you can understand why this is true, you are at least one step on the road to understanding type II diabetes. Or to be more accurate, what is the true underlying cause of insulin resistance and high blood sugar levels. You will also understand that obesity has only a small and indirect part to play in this process; that BMI has no relevance to the issue, and that the simple causal chain: Obesity > insulin resistance > raised blood sugar level……is wrong.
Of course obesity is closely associated with diabetes – to state otherwise would be nuts. However it is not the cause of type II diabetes. It is caused by it. By which I mean that obesity is (in major part) caused by that the underlying process that also leads to insulin resistance and high sugar levels. There is a causal chain here, but it is not Obesity>insulin resistance>raised blood sugar levels.
More on this later, once your brain has become unscrambled.
*Yes, for those who know about this area, you can talk about visceral fat, but this is another more interesting and completely different discussion. I am also only discussion type II diabetes, not type I (which is a completely different condition altogether).
There is a doctor in the USA called Duane Graveline who I know well. He trained as an astronaut, when such things were seen as exciting. He was very much mainstream in his prescribing and thinking about medicine, until he was started on statins. He took them happily, until he suffered an episode of transient global amnesia. A complete loss of memory, re-booting his brain to the age of about eight.
On the first occasion he had no idea what had happened. He thought he could have had a stroke, but after investigations nothing was found. He asked if the statin could have caused this, and was told no – not a chance. So he started on statins again, and suffered another episode, the same as the last.
He then started investigating and found that thousands of others had suffered from episodes of transient global amnesia whilst on statins. A very, very, rare thing to happen to anyone, but increasingly common nowadays. I wonder why? Dr. Graveline then started to develop a neuromuscular disease, similar to amyotrophic lateral sclerosis (ALS) which he attributes to the statin. Statins can certainly cause neuropathy – but I shall say no more on this issue at present.
Dr. Graveline is not so keen on statins now, nor does he believe that cholesterol causes heart disease – having looked at the evidence again with a fresh eye. For those who do not know, he has a website www.spacedoc.com. Here are listed all of the many adverse effects of statins, and the suffering of many thousands of people.
He believes that the authorities are, basically, turning a blind eye to the many and varied problems with statins. So he has laboriously gone through the Food and Drug Administration (FDA) database of Adverse Drug Events (Medwatch), to find out just exactly how many deaths statins have caused.
This is extremely difficult to analyse as the coding system in Medwatch is complex, poorly linked and many things – frankly – do not seem to make sense. Whilst going through this stuff is an absolute nightmare, it can be done – although you have to make some assumptions along the way.
What Dr. Graveline did was to look for case of rhabdomyolysis (catastrophic breakdown of muscle tissue) linked to statins. Rhabdomyolysis is a pretty specific, and well-accepted, adverse effect of al statins. However, it is considered as so vanishingly rare as to be not worth bothering about by most doctors.
Rhabdomyolysis carries a very high mortality rate, because the waste products of dissolving muscles travel to the kidneys, where they block up the nephrons, causing acute kidney failure. In around ten per-cent of cases rhabdomyolysis is fatal. So you can assume, with reasonable accuracy, that for every ten reported cases of rhabomyolysis, you will get one death. You will also get a number of people with destroyed kidneys who end up on dialysis – hey ho.
At this point I should also point out that adverse drug events are widely known to be a massively under-reported. It is difficult to be certain on the exact figures. However, having read many papers on this subject the general feeling is that about 1 – 5% of all events are actually reported by anyone – ever. Which means that any figures in Medwatch can be pretty reliably multiplied by twenty to one hundred? Which is a topic for another day.
Anyway, with this pre-amble out of the way, I have copied Dr. Graveline’s blog on statins (with his full permission). What he has found is that, over a six year period there were 8,111 cases of rhabodmyolysis reported to Medwatch associated with statins. This represents, at least, 811 deaths in this period. [If you were to multiply this figure by twenty, this is 16,200. Multiply by one hundred and you have 81,110.]
A few years ago one of the statins called Baycol was rapidly removed by the FDA after sixty people died from rhabdomyolysis whilst taking statins. Well, all statins can cause rhabdomyolysis. Hundreds have died, probably more, since Baycol was yanked from the market. Yet there is absolute radio silence on this issue.
Below is Dr. Graveline’s blog…
Relative risk of Statin Associated Rhabdomyolysis
A recent study comparing the relative risks of muscle problems with the use of the various statin drugs has recently been reported. Generally the risk of muscle adverse effects varies with the strength of the statin used except for the statin fluvastatin (Lescol). Lescol, usually considered to be the weakest of the commonly used statins now shares with rosuvastatin (Crestor), the strongest of the statins, in being consistently linked to higher adverse muscle events relative to the other commonly used statins. Atorvastatin (Lipitor) and simvastatin (Zocor) showed intermediate risks and pravastatin (Pravachol) and lovastatin (Mevacor) had the lowest risk rates. Designating rosuvastatin’s and fluvastatin’s relative risk as 100%, comparative rates for atorvastatin, simvastatin, pravastatin, and lovastatin were, respectively, 55%, 26%, 17%, and 7.5%.
There were a total of 186,796 case reports listed within the Adverse Event database (Medwatch) during the study period 1 Jul 2005 to 31 Mar 2011. Choosing rhabdomyolysis as one of the more discrete and credible of the muscle diagnoses, a total of 8,111 cases of rhabdomyolysis were reported during this study period, averaging 1,350 cases yearly. Sidney Wolfe MD has previously estimated the statin associated rhabdomyolysis death rate to be 10 percent (giving a total of 811 deaths during this 6 year 4 month time period). Of the total number of rhabdomyolysis cases, fluvastatin was involved in 164, rosuvastatin in 1146, simvastatin in 3395, atorvastatin in 1641, pravastatin in 267 and lovastatin in 161.
Returning to the death rate estimate of 811, this strikes me as extraordinarily high and I cannot believe I am just now discovering this. Back in the Baycol crisis of 2004, sixty deaths caused FDA to rise up and Bayer to take its problematic product off the shelves. Six years later, 811 deaths do not even deserve a mention. What has happened? Where is the media uproar that we had back in 2004? I knew the Medwatch figures for Lipitor because I had obtained a copy of the Medwatch data and counted the rhabdomyolysis cases myself. I counted 2731 cases of rhabdomyolysis from the period 1997 to 2011 from Lipitor alone which fits quite well with this recently published work. So I had a heads up. I predicted the total rhabdomyolysis cases would be 6,000 for all the statins never suspecting I would underestimate by several thousand.
Medwatch exists for FDA to monitor these outrageous post marketing events and report back to the medical community. Where is the FDA report? This is incredible!
A couple of night’s ago, I was watching a programme called ‘Long Live Britain’ on the BBC, co-presented by Phil Hammond. He is a UK doctor whom I greatly admire, and who mostly talks common sense. So I hesitate to criticise him. But on this programme I heard him say these very words to a volunteer on the programme (sic) ‘A lifetime of eating fatty food has made your liver fatty……’ In truth, he may have used slightly different words, but I cannot bear to watch again.
He then went on to present a lengthy clip of a very unwell lady with (I presume, though not stated), non-alcoholic steatohepatitis NASH. This is the name for a damaged, fatty, liver. A condition that can worsen and worsen and may, eventually, lead to liver failure.
Sorry Phil, but when I heard you say that eating fat caused a fatty liver, I had to switch the television off and take a few deep breaths, lest my blood pressure became too high.
What is it about diet that no-one has even the faintest damned idea what they are talking about, especially when I comes to fat consumption. I think we have demonised fat for so long that you can say anything about fat and, so long as it is sufficiently damning; no-one dares question anything you say. Science goes straight out the window.
A.N. Idiot: ‘Did you know that eating fat can make your liver explode.’
A.N. Other Idiot: ‘OMG, I never knew that.’
A.N. Idiot: ‘It’s true. It must be, I saw it on the telly.’
Well, here are a few facts that really are facts. When you eat fat it is absorbed in the small bowel, turned into triglycerides, and packaged into a lipoprotein called a chylomicron. Chylomicrons are then fed directly into the bloodstream via the thoracic duct – bypassing the liver completely. As they pass fat cells, the cells strip almost all of the fat out of them, so the chylomicrons shrink down and down in size, becoming chylomicron remnants. Once almost all fat is gone, these remnants are absorbed into the liver.
As should be clear from this, at no point in this process does the vast, vast, majority of fat we eat get anywhere near the liver. It is carried from the bowel directly into adipose tissue. So, Phil, how does eating fat make your liver fatty…exactly? When the liver has no part of play in the absorption, transport and storage of any fat we eat? Oh, sorry, you’re right, it can’t.
Carbohydrates, on the other hand, now here you are talking. All the carbohydrates we eat are converted into glucose and/or fructose in the gut [apart from fibre, and starch, which we cannot digest]. Glucose and fructose then pass directly into the liver where, if your body’s sugar stores are full, they are converted into…you guessed it…fat. [Your body can only store about fifteen hundred calories of energy as glucose/sugar before the stores are full – which is not a lot].
Imagine, if you will, a body with full sugar stores* – this would be most people, most of the time. You eat carbohydrate a.k.a. proto-sugar. With sugar stores full, there is nowhere for this excess sugar to go, so the liver converts it all into fat a.k.a. triglycerides. The liver tries to stick this excess triglyceride into a lipoprotein called a VLDL (Very Low Density Lipoprotein). However, this process is complex, so the liver starts to fill up with fat.
At the same time insulin does battle with the liver, in order to drive lipogenesis (the making of fat from sugar) in the liver. Which means that you are more likely to end up with diabetes. This is not rocket science. This is basic human metabolism/physiology. And you know what, the way to reverse this process is…TO EAT FAT.
The simple fact is that there is no way on God’s earth that eating fat can give you a fatty liver. However, the process by which eating excess carbohydrate could give you a fatty liver, and then diabetes, is simple and straightforward. Yet we have a BBC programme, with a real doctor on it, stating the exact opposite.
I suppose I don’t really blame Phil Hammond too much. We have all been fed with such unutterable balls about the dangers of eating fat for so long now that the science behind nutrition long since became an inconvenience. ‘Do not bother me with facts, for my mind is made up.’
Or ‘don’t bother me with the fats; I am going to kill myself eating carbohydrates.’ Long Live Britain indeed.
*sugar/glucose is stored in the body as glycogen, a polymer of glucose (lots and lots of glucose molecules stuck together). The body does this to reduce the amount of water required to encircle individual glucose molecules.
(Quis custodiet ipsos custodes?)
Mainstream medicine increasingly relies on Guidelines. Well, they are called guidelines, but increasingly they carry the force of law. In many countries if you try to practice outside the wise and infallible guidelines you may lose your license to practice medicine. In the US, you may well be dragged into court, and if you have not been following the guidelines, you will be sued. You can even be gaoled (or jailed, as we say in the UK).
In short, guidelines are very serious and important things indeed, and they now rule medicine with a rod of steel. In the UK up to 50% of general practice time is spend ensuring that all patients are constantly monitored to ensure that various guidelines are rigorously followed. Is the BP low enough, the cholesterol low enough, have you checked blood sugar levels etc.
But where do guidelines come from – exactly? Who gives people the right to sit on guideline committees? What are the entrance requirements? Who shall guard the guideliners?
The answer is, perhaps shockingly, that there are almost no rules to this. If a group, such as the National Institutes for Health in the US, decides to set up a committee to decide on, for example, what is the healthy level for cholesterol lowering, what happens? They ask a number of Key Opinion Leaders to join the committee. In this case the NCEP (National Cholesterol Education Programme – which is a committee, not a programme).
In 2004 this committee decided that cholesterol levels should be lowered far more aggressively than in the past. Based on, as far as I could see, very flimsy evidence. Could it be that that committee was, in some way, biased in favour of cholesterol lowering companies? A number of people, including me, demanded to see if any of the eight invited members of this hugely important committee had financial conflicts.
With much reluctance, the conflicts were revealed (I have highlighted, in bold, the companies who marketed cholesterol lowering agents at the time.) See below
ATP III Update 2004: Financial Disclosure of NCEP members
Dr. Cleeman: (Chairman) has no financial relationships to disclose.
Dr. Grundy: has received honoraria from Merck, Pfizer, Sankyo, Bayer, Merck/Schering-Plough, Kos, Abbott, Bristol-Myers Squibb, and AstraZeneca; he has received research grants from Merck, Abbott, and Glaxo Smith Kline.
Dr. Bairey Merz: has received lecture honoraria from Pfizer, Merck, and Kos; she has served as a consultant for Pfizer, Bayer, and EHC (Merck); she has received unrestricted institutional grants for Continuing Medical Education from Pfizer, Procter & Gamble, Novartis, Wyeth, AstraZeneca, and Bristol-Myers Squibb Medical Imaging; she has received a research grant from Merck; she has stock in Boston Scientific, IVAX, Eli Lilly, Medtronic, Johnson & Johnson, SCIPIE Insurance, ATS Medical, and Biosite.
Dr. Brewer: has received honoraria from AstraZeneca, Pfizer, Lipid Sciences, Merck, Merck/Schering-Plough, Fournier, Tularik, Esperion, and Novartis; he has served as a consultant for AstraZeneca, Pfizer, Lipid Sciences, Merck, Merck/Schering-Plough, Fournier, Tularik, Sankyo, and Novartis.
Dr. Clark: has received honoraria for educational presentations from Abbott, AstraZeneca, Bristol-Myers Squibb, Merck, and Pfizer; he has received grant/research support from Abbott, AstraZeneca, Bristol-Myers Squibb, Merck, and Pfizer.
Dr. Hunninghake: has received honoraria for consulting and speakers bureau from AstraZeneca, Merck, Merck/Schering-Plough, and Pfizer, and for consulting from Kos; he has received research grants from AstraZeneca, Bristol-Myers Squibb, Kos, Merck, Merck/Schering-Plough, Novartis, and Pfizer.
Dr. Pasternak: has served as a speaker for Pfizer, Merck, Merck/Schering-Plough, Takeda, Kos, BMS-Sanofi, and Novartis; he has served as a consultant for Merck, Merck/Schering-Plough, Sanofi, Pfizer Health Solutions, Johnson & Johnson-Merck, and AstraZeneca.
Dr. Smith: has received institutional research support from Merck; he has stock in Medtronic and Johnson & Johnson.
Dr. Stone: has received honoraria for educational lectures from Abbott, AstraZeneca, Bristol-Myers Squibb, Kos, Merck, Merck/Schering-Plough, Novartis, Pfizer, Reliant, and Sankyo; he has served as a consultant for Abbott, Merck, Merck/Schering-Plough, Pfizer, and Reliant.
http://www.nhlbi.nih.gov/guidelines/cholesterol/atp3upd04_disclose.htm
Of course, as people have stated to me, the mere fact that there were seventy two financial conflicts of interest does not mean that the guidelines themselves were biased. But you know what, I don’t believe it. Imagine if eight Supreme Court judges, ruling on any issue, had seventy two direct financial conflicts of interest to do with that issue…..Well, the outcry would never end.
Yet doctors, it seems, are beyond any suspicion – of any sort. There is not the slightest possibility that any doctor would ever do anything wrong….We are, after all, superior beings. ‘But, what’s that you say skippy…. hold on.’
‘Despite a 2-year-old scandal discrediting key evidence, current guidelines relying on this evidence have not been revised. As a result of physicians following these guidelines, some researchers say, it is possible that thousands of patients may have died each year in the UK alone. It is unlikely that a true understanding of the damage will ever be known…..
The guidelines, which were published in 2009, were based on analyses of the available trials. The strongest evidence came from the DECREASE family of trials, which appeared to strongly support perioperative beta-blockade, and one other large trial, POISE, which raised concerns that beta-blockers might lead to an increase in deaths
In 2011, however, faith in the reliability of the DECREASE trials was shattered as a result of a scientific misconduct scandal centering on the principal investigator of the studies, the now disgraced Dutch researcher Don Poldermans. The issue was further complicated because, in addition to his key role in the trials, Poldermans was the chairman of the committee that drafted the guidelines.’ http://cardiobrief.org/2013/07/31/european-heart-guidelines-based-on-disgraced-research-may-have-caused-thousands-of-deaths/
Oh well, maybe not.
The fact is that, wherever you look, guidelines are being developed by doctors who have widespread conflicts of interest. And if you go a step further back to review the studies that the guidelines are based on, they are run by, and written up by, doctors who have enormous conflicts of interest. Although sometimes, these conflicts are just…well, forgotten about.
For example, a few opinion leader were ‘named and shamed’ by the Journal of the American Medical Association, when someone pointed out that a number of the authors of the original paper they wrote might just have slipped up in declaring their conflicts:
Unreported Financial Disclosures in: ‘Association of LDL Cholesterol, Non–HDL Cholesterol, and Apolipoprotein B Levels With Risk of Cardiovascular Events Among Patients Treated With Statins: A Meta-analysis.’
….the following disclosures should have been reported: “Dr Mora reports receipt of travel accommodations/meeting expenses from Pfizer; Dr Durrington reports provision of consulting services to Hoffman-La Roche, delivering lectures or serving on the speakers bureau for Pfizer, and receipt of royalties from Hodder Arnold Health Press; Dr Hitman reports receipt of lecture fees and travel expenses from Pfizer, provision of consulting services on advisory panels to GlaxoSmithKline, Merck Sharp & Dohme, Eli Lilly, and Novo Nordisk, receipt of a grant from Eli Lilly, and delivering lectures or serving on the speakers bureau for GlaxoSmithKline, Takeda, and Merck Sharp & Dohme; Dr Welch reports receipt of a grant, consulting fees, travel support, payment for writing or manuscript review, and provision of writing assistance, medicines, equipment, or administrative support from Pfizer, and provision of consultancy services to Edwards, MAP, and NuPathe; Dr Demicco reports having stock/stock options with Pfizer; Dr Clearfield reports provision of consulting services on advisory committees to Merck Sharp & Dohme and AstraZeneca; Dr Tonkin reports provision of consulting services to Pfizer, delivering lectures or serving on the speakers bureau for Novartis and Roche, and having stock/stock options with CSL and Sonic Health Care; and Dr Ridker reports board membership with Merck Sharp & Dohme and receipt of a grant or pending grant to his institution from Amgen. http://jama.ama-assn.org/content/307/16/1694.3.full?etoc
Not a bad little list. As you can see, Dr Ridker had board membership with Merck Sharp and Dohme…… a company that has made billions from selling statins. Now, here is he is authoring a paper on the benefit of statins (which will be used to develop guidelines on cholesterol lowering), and he simply forgot about this conflict of interest. As for the others, well, they’re also busy people; things must have just slipped their minds, such as thirty three separate financial conflicts.
For this terrible crime against the integrity of medical science, none of them can ever again do medical research, or author a medical paper, or sit on guideline committees. Cue, mad cackling laughter. As you may expect, absolutely nothing happened at all, apart from the publication of that statement you in the Journal in the American Medical Journal (JAMA).
I am sorry, but the system of developing guidelines is, frankly, bust. It has been for many years, but it is a very big and dangerous looking nettle to grasp, and no-one, currently has the will to do it.
Someone, somewhere, needs to ensure that guidelines, and the evidence they are based on, and the interpretation of that evidence, is of the highest quality – and free from potential bias, and financial conflicts of interest. We are about as far from this happy state of affairs as I am from being invited onto any guideline committee, ever, anywhere.
And that, my friend, is a very, very long way away indeed. You would need to Hubble telescope to see across distances as vast as that.
Last week I was going through some old files, and presentations, in a vague effort to clean up my computer. Whilst looking a one of many thousands of studies I had filed away I came across this paper: ‘Clarifying the direct relation between total cholesterol levels and death from coronary heart disease in older persons1.’
I read it, and immediately recalled why I kept it. For it came to the following, final, conclusion:
‘Elevated total cholesterol level is a risk factor for death from coronary heart disease in older adults.’
I remember when I first read this paper a few years ago. My initial thought was to doubt that it could be true. Most of the evidence I had seen strongly suggested that, in the elderly, a high cholesterol level was actually protective against Coronary Heart Disease (CHD).
However, when a bunch of investigators state unequivocally that elevated cholesterol is a risk factor for heart disease, I try to give them the benefit of the doubt. So I read the damned thing. Always a potentially dangerous waste of precious brainpower.
Now, I am not going to dissect all the data in detail here, but one sentence that jumped out of the paper was the following:
‘Persons (Over 65) with the lowest total cholesterol levels ≤4.15 mmol/L had the highest rate of death from coronary heart disease, whereas those with elevated total cholesterol levels ≥ or = 6.20 mmol/L seemed to have a lower risk for death from coronary heart disease. ‘
Now, I can hardly blame you if you struggled to fit those two quotes together. On one hand, the conclusion of the paper was that .. ‘Elevated total cholesterol level is a risk factor for death from coronary heart disease in older adults.’ On the other hand, the authors reported that those with the lowest total cholesterol levels had the highest rate of CHD; whilst those with the highest cholesterol levels had the lowest rate of CHD.
Taken at face value, this paper seems to be contradicting itself…. utterly. However, the key word here, as you may have already noted, is seemed. As in… those with elevated total cholesterol levels ≥ or = 6.20 mmol/L seemed to have a lower risk for death from coronary heart disease. ‘
Now you may think that this is a strange word to use in a scientific paper. Surely those with elevated total cholesterol levels either did, or did not, have a lower risk of death from CHD? Dying is not really something you can fake, and once a cause of death has been recorded it cannot be changed at a later date. So how can someone seem to die of something – yet not die of it?
The answer is that you take the bare statistics, then you stretch them and bend them until you get the answer you want. Firstly, you adjust your figures for established risk factors for coronary heart disease – which may be justified (or may not be). Then you adjust for markers of poor health – which most certainly is not justified – as you have no idea if you are looking at cause, effect, or association.
Then, when this doesn’t provide the answer you want, you exclude a whole bunch of deaths, for reasons that are complete nonsense. I quote:
‘After adjustment for established risk factors for coronary heart disease and markers of poor health and exclusion of 44 deaths from coronary heart disease that occurred within the first year, (my bold text) elevated total cholesterol levels predicted increased risk for death from coronary heart disease, and the risk for death from coronary heart disease decreased as cholesterol levels decreased.’
Why did they exclude 44 deaths within the first year? Well, they decided that having a low cholesterol levels was a marker for poor health, and so it was the poor health that killed them within the first year.
The reason why they believed they could do this is that, a number of years ago, a man called Iribarren decreed that the raised mortality always seen in those with low cholesterol levels is because people with low cholesterol have underlying diseases. And it is these underlying diseases that kill them. (What, even dying from CHD. And how, exactly does CHD cause a low cholesterol levels….one might ask).
In truth, there has never been a scrap of evidence to support Iribarren’s made-up ad-hoc hypothesis. [A bottle of champagne for anyone who can find any evidence]. However, it is now so widely believed to be true, that no-one questions it.
Anyway, without chasing down too many completely made-up ad-hoc hypotheses, the bottom line is that this paper stands a perfect example of how you can take a result you don’t like and turn it through one hundred and eighty degrees. At which point you have a conclusion that you do like.
Young researcher: (Bright and innocent) ‘Look, this is really interesting, elderly people with low cholesterol levels are at greater risk of dying of heart disease.’
Professor: (Smoothly threatening) ‘I think you will find…. if you were to look more carefully, that this is not what you actually found….. Is it? By the way, how is your latest grant application going?’
Young researcher: (Flushing red at realising his blunder) ‘Yes, by golly, how silly of me. I think I really found that elderly people with high cholesterol levels are at a greater risk of dying of heart disease.’
Professor: ‘Yes, excellent. Be a good lad, find a good statistician to make sure the figures make sense, and write it up.’
For those who wonder at my almost absolute cynicism with regard to the current state of Evidence Based Medicine, I offer this paper as a further example of the way that facts are beaten into submission until they fit with current medical scientific dogma.
As a final sign off I would advise that any paper that has the word ‘clarifying’ in its title, should be treated with the utmost suspicion. I think George Orwell would know exactly what the word clarifying means in this context. Facts do not need clarification.
1: Corti MC et al: Clarifying the direct relation between total cholesterol levels and death from coronary heart disease in older persons. Ann Intern Med. 1997 May 15;126(10):753-60
Here is Wikipedia on the wisdom of Karl Popper:
“The classical view of the philosophy of science is that it is the goal of science to prove hypotheses like “All swans are white” or to induce them from observational data. Popper argued that this would require the inference of a general rule from a number of individual cases, which is inadmissible in deductive logic. However, if one finds one single black swan, deductive logic admits the conclusion that the statement that all swans are white is false. Falsificationism thus strives for questioning, for falsification, of hypotheses instead of proving them.”
Sorry, although I am a great fan of Popper, his language is a bit, well, pedantic. What he is saying here is that science starts with a hypothesis e.g. ‘all swans are white.’ If you find white swan after white swan, then you will mildly strengthen the hypothesis. However, once you find one black swan, the hypothesis is dead. (Unless you decree that, as all swans are white, a black swan cannot – by definition – be a swan).
One of the great white swans of cardiology is that Familial Hypercholesterolaemia (FH) causes heart disease. When I give talks to other doctors informing them that the cholesterol hypothesis is bunk, one of the ‘facts’ that is triumphantly used to knock me down is that ‘People with Familial Hypercholesterolaemia die very young from heart disease.’ Case proven, raised cholesterol causes heart disease, now move on.
A little bit of context is needed here. Familial Hypercholesterolaemia (FH) affects about one in five hundred people. It is a genetic condition where those who have it (I refuse to use the words suffer from it) have very high Low Density Lipoprotein (LDL) levels. As everyone knows LDL is known as ‘bad’ cholesterol, which is considered to be the number one risk factor for heart disease. (Of course LDL is not cholesterol at all but, hey, why let scientific accuracy get in the way of…. Well, science).
Goldstein and Brown established that the cause of FH is a lack of LDL receptors on cells. LDL receptors are the things that bind on to LDL molecules and then remove them from the bloodstream. Cells manufacture LDL receptors when they are low on cholesterol and need more.
Once the receptor is made it is pushed out through the cell membrane to attract an LDL molecule. When an LDL molecule has been caught, by binding on to the receptor, the LDL and the attached receptor are pulled back into the cell and broken down. Because they function this way, LDL receptors only work once. If a cell wants more cholesterol, then it needs to manufacture more LDL receptors.
Clearly, if there are not enough LDL receptors being manufactured, the entry of LDL into cells is restricted. This means that blood levels of LDL rise, and you will be diagnosed with Familial Hypercholesterolemia. If, that is, you have a blood test.
Moving sideways for a moment I need to mention that most people with FH are heterozygotic, by which I mean they carry one gene for FH. Their LDL levels are therefore about double that of the surrounding population. However, those with homozygotic FH (carrying both genes) have LDL levels that can be twenty times ‘normal’. More on this group in a later blog.
Back to FH. If you have a heart attack when young, by which I mean under about 55, and you have FH, doctors will nod sagely and that that ‘it was the FH that did it.’ (If you don’t have FH, they will say it was something else that did it).
Sometimes the relatives of those dying young of CHD with FH, are contacted. It is often found that there is a higher rate of FH and premature CHD in relatives. This type of evidence has been used as proof that FH causes CHD. Maybe. Maybe not. If someone dies young from CHD, and has FH, and other relatives have a higher rate of both FH and CHD, what have we actually proved? We have proved nothing – for certain.
All we have done is to establish that relatives of people with FH and premature CHD also have FH (as they must, as it is a dominant gene) and also have a higher rate of CHD. Now, it could be that the FH is the reason for their CHD. Or it might not. It could be that something else, genetic of behavioural, is causing their high rate of CHD.
Given this problem of inherent bias, how could you tell if the FH is causing the CHD or not? Or, better, how could you falsify the hypothesis that FH causes CHD? Can you find a black swan?
Well the best way to find a black swan in this ara is to turn your study inside out. Instead of looking at people with FH and premature CHD, then looking at their relatives to find FH and CHD, you need look for premature CHD first (knowing nothing of FH status), then see if FH is more prevalent in first degree relatives.
How do you do this? Well, firstly you ask hundreds thousands of students if their father had a heart attack, or died of heart attack before the age of 55. Then you measure the LDL level of those students to see if they have FH. At the same time you find age and sex matched control students to see if they have FH.
Now, if FH really were a major cause of premature CHD you would expect to find that FH was far, far, more prevalent amongst those students whose fathers suffered CHD before the age of 55.
Such a study was done once, in the Netherlands. The results were as follows:
In the EARS (European Atherosclerosis Research Society) studies, University students whose fathers had proven CHD before the age of 55 years, were recruited …Age and sex-matched controls were recruited from the same populations for each case.
Thus, the prevalence of FH in both groups was not significantly different at approximately 1 in 500, which is the estimated prevalence of the condition in the general population. The evidence that heterozygote FH is, of itself, a cause of atherosclerosis is unsatisfactory.
http://www.bmj.com/content/322/7293/1019/reply
In short, when someone finally did a study on the association between premature CHD and FH, where selection bias was removed, they found that FH was no more common in those with, and without, a strong family history of CHD. This was the blackest of black swans.
However, there is a twist to this tale. Which is that this study was never published anywhere. The only reason that I know about it, is that I was reading the responses section in the British Medical Journal, and the lead investigator of the study wrote the above letter in reply to a discussion on FH. (Something more than easily missed).
I contacted him, and asked why the study had not been published. He did not provide any answer that made any sense to me. The end result of the lack of publication is that the blackest of black swans is not actually black. It is invisible. Until now, of course.
P.S. As for homozygotic FH, I shall deal with this later.
For hundreds of years, medicine was driven by anecdote and personal beliefs, without the slightest supportive evidence. In the nineteen twenties the most common operation done was ‘removal of toxic colon.’ Toxic colons were believed to be responsible for almost any symptom you could think of.
Surgeons became blindingly wealthy cutting out significant lengths of the large bowel in those who could afford it. This operation, and the greed and stupidity that drove it, is outlined in the book ‘Doctors Dilemmas’, by George Bernard Shaw. He went on to say that: ‘If you pay people to cut things out of you, then that it exactly what they are going to do.’
Not many people have their toxic colons removed nowadays, in fact no-one does, as the condition no longer even exists. But many people still have coronary artery bypass grafts done. Although there is not the slightest evidence that this does any good either. For more on this read Bernard Lown’s essay
Anyway, over time doctors began to recognise that if you were going to cut things out of people, or prescribe drugs, it would be nice to know if any of this activity actually did any good. And so began the dawning of the age of evidence based medicine (EBM). (Evidence based medicine is a far more recent movement than you might think, not really getting under way until the 1980s).
The individuals who really drove this forward e.g. Sackett, Cochrane, Muir-Gray were extremely hard working idealists. They were highly ethical and had the patient’s interest at heart. They taught EBM on wards with students, and looked for evidence wherever they could find it.
This was a much more difficult thing to do before the advent of the world wide web. I remember searching around for papers in medical libraries, taking literally hours to find the papers I was looking for. Something I can now do in seconds on the Internet.
In theory, of course, EBM should be a very good thing, and in some ways it has been. However, EBM relies entirely on the belief that the evidence you are using is accurate, or true, or believable, or unbiased, or whatever form of words you are most comfortable with. This may have been true once upon a time, but things have most certainly changed.
In the early days a great deal of research was carried out in major teaching Universities. Doctors and researchers would set up the trials, run them, and analyse the results. However, the turn of the millennium less than a third of drug related studies were being done in academic units.
To quote from the New York Times:
‘The removal of research from academic centres also gives pharmaceutical companies greater control over the design of studies, analysis of data, and publication of results.
The end result: among even the highest quality clinical research the odds are 5.3 times greater that commercially funded studies will support their sponsor’s products than non-commercially funded studies. The authors conclude, “Readers should carefully evaluate whether conclusions in randomized trials are supported by data.” Careful readers with enough time can sometimes spot discrepancies between data and conclusions in published studies. However, the drug companies typically retain control over the data from their sponsored trials so the majority of the researchers don’t have open access to the results from their own studies.’ Petersen M. ‘Madison Ave. has growing role in the business of drug research.’ New York Times, November, 2002.
In a similar, if less emotive vein, the most downloaded paper within recent medical scientific literature was written by John Lonnadis. It was entitled ‘Why most published research findings are false.’
The vast majority of people have never heard of this paper. The vast majority of those who have heard of it have never read it, and the vast majority of those who have read it, have clearly not understood the implications of what they have just read. Or, if they have…they are too frightened to do anything about it.
The shortest summary of his research is, as follows:
‘Moreover, for many current scientific fields, claimed research findings may often be simply accurate measures of the prevailing bias.’ J Lonnadis.
These words sound relatively mild, but the implications are explosive. Basically, many researchers are claiming that they have proved something to be true, but all they have actually done is to manipulate their research in order to confirm what they already ‘knew’ to be true.
In essence, medical research has become horribly biased, to the point where David Sackett (a hero of mine) has virtually withdrawn from the arena
‘According to the founder of Evidence Based Medicine experts are hindering the healthy advancement of science.
Writing in this week’s British Medical Journal (BMJ), Canadian-based researcher, David Sackett, said that he would “never again lecture, write, or referee anything to do with evidence based clinical practice”. Sackett is not doing this because he has ceased to believe in evidence based clinical practice but, as the BMJ comments, because he is worried about the power of experts in stifling new ideas and wants the retirement of experts to be made compulsory.
Sackett claims that the prestige of experts (including himself) gives their opinions far greater persuasive power than they deserve on scientific grounds alone.”Whether through deference, fear, or respect, others tend not to challenge them, and progress towards the truth is impaired in the presence of an expert,” he writes.
He also argues that expert bias against new ideas operates during the review of grant applications and manuscripts. “Reviewers face the unavoidable temptation to accept or reject new evidence and ideas, not on the basis of scientific merit, but on the extent to which they agree or disagree with the public positions taken by experts on these matters.” http://www.abc.net.au/science/news/health/HealthRepublish_124166.htm
When the man who virtually invented evidence based medicine states that research has become institutionally biased, where can we look? I am not sure. I will leave you with a thought from Professor Bruce Charlton
The decline of honesty in science
Anyone who has been a scientist for more than 20 years will realize that there has been a progressive decline in the honesty of communications between scientists, between scientists and their institutions, and between scientists and their institutions and the outside world.
Yet real science must be an arena where truth is the rule; or else the activity simply stops being science and becomes something else: Zombie science. Zombie science is a science that is dead, but is artificially kept moving by a continual infusion of funding. From a distance Zombie science look like the real thing, the surface features of a science are in place – white coats, laboratories, computer programming, PhDs, papers, conference, prizes, etc. But the Zombie is not interested in the pursuit of truth – its citations are externally-controlled and directed at non-scientific goals, and inside the Zombie everything is rotten…..
Scientists are usually too careful and clever to risk telling outright lies, but instead they push the envelope of exaggeration, selectivity and distortion as far as possible. And tolerance for this kind of untruthfulness has greatly increased over recent years. So it is now routine for scientists deliberately to ‘hype’ the significance of their status and performance and ‘spin’ the importance of their research.
Bruce Charlton: Professor of Theoretical Medicine
So, what can be done?
Excess salt intake is one of the great issues in preventative medicine. Last year I watched a bus go by, with an advert for reducing salt plastered all over the side. Some restaurants have taken salt cellars off their tables, to protect customers. Many foodstuffs now have their salt content clearly labelled, with high salt content given a red sticker.
Given all of this you would think, would you not, that the case for excess salt consumption causing cardiovascular disease had been made beyond even the slightest possibility of doubt. One of the arguments in support of the dangers of salt consumption (the one that I am looking at in this article), comes from the native peoples living in the Amazon
The Amazon is an extremely low salt environment, and the average salt consumption of those living there is at very low. Several studies have found that the tribes people living in the Amazon have very low blood pressure which does not increase with age. They also have very little in the way heart disease and strokes.
‘Primitive societies who ingest little or no salt have no hypertension1’
Proof, the anti-salt lobby cry, that it is excess salt intake that causes our blood pressure to rise dangerously.
Or is it? When presented with ‘proof’ like this I tend to look for contradiction, rather than confirmation. Are there, I wondered, other populations that fail to demonstrate a rise in blood pressure with age, that do not have a low salt consumption. My attention was drawn to nuns, living in Italy.
‘The powerful effect of psychosocial and acculturating influences on population blood pressure trends seems to be confirmed, through longitudinal observations, in the nuns in a secluded order. After initial observations had been made on culture, body form, blood pressure, diet, and other variables in 144 nuns and 138 lay women, included as a control group, a 30-year follow-up study was undertaken. Most striking were opposite trends noted between the two groups in blood pressure trend. During the follow-up period, blood pressure remained remarkably stable among the nuns. None showed an increase in diastolic blood pressure over 90 mm Hg.’
So, nuns do not develop high blood pressure as they age. What happened to the control women in this study?
‘By contrast, the control women showed the expected increase in blood pressure with age. This resulted in a gradually greater difference (delta>30/15 mm Hg) in systolic and diastolic blood pressure between the two groups, which was statistically significant.’
No difference in diet or salt consumption, yet one population developed the ‘normal’ Western rate of hypertension whilst the other did not. What did the authors of this thirty yearlong study think was the reason for this finding?
‘In conclusion, it seems reasonable to attribute much of the difference in blood pressure and cardiovascular events, to the different burden in psychosocial factor and to the preserved peaceful lifestyle of the nuns2.’
Now I do not know for sure if those living in the Brazilian rain forests have managed to preserve a traditional peaceful lifestyle – but it seems a reasonable assumption to make.
However, the main point I am trying to make here is that you do not need a low salt diet in order to prevent hypertension. You can find populations with a normal salt diet who do not develop hypertension either.
What factor, or factors, appears to link these two populations? The factor appears to be living a preserved peaceful lifestyle. This would suggest that stress is the cause of hypertension and cardiovascular disease, and not salt. Whilst association cannot prove causation, a lack of association disproves it.
1: Freis ED. The role of salt in hypertension. Blood Pressure 1992; 1: 196-200.
2: Timio M, et al: ‘Blood pressure in nuns in a secluded order: A 30-year follow-up.’ Miner Electrolyte Metab. 1999 Jan-Apr;25(1-2):73-9
A day or so ago I received this e-mail from a doctor in London.
Dear Dr Kendrick,
I work as a GP in Wandsworth London and I read that you don’t
believe that much in cholesterol and CHD.
I do agree up to 50% of MI patients have normal cholesterol
but some say what’s normal for UK is actually high. Is this argument valid?
Best wishes
Define ‘normal.’ Does normal mean average? If we took the average height of everyone in the UK we would find (very nearly) that 50% of those dying of CHD (coronary heart disease) were above average height and 50% below. So average is clearly normal, but then again so is being tall, or short.
However, if we decided that average height of everyone living in the UK was above ‘normal’, and we then lowered the definition of ‘normal height’ by three inches, we would find that the vast majority of people dying of CHD were now above average height. At which point we could decree that being taller than normal was a risk factor for CHD.
This would obviously be a completely bonkers thing to do. Yet, you can do it with cholesterol levels and everyone nods in general agreement.
Aha, but the argument goes that our lives are completely different than the lives of our ancestors, which has caused our cholesterol levels to be unnaturally high.
An article in the Journal of the American College of Cardiology best summed up this line of thinking. Under the heading ‘Why average is not normal’, O’Keefe, the lead author, made the claim that: ‘Atherosclerosis is endemic in our population, in part because the average LDL (“bad” cholesterol) level is approximately twice the normal physiologic level.’ In short, according to O’Keefe, our cholesterol level should be about 2.5mmol/l, not 5.2mmol/l.
He based his argument, in part on looking at the cholesterol levels of various animals e.g. elephants, and boars, and suchlike. He also used the argument that very young babies (neonates) have cholesterol level of about 2.5mmol/l. Now, in my opinion, anyone proposing this argument should have their medication increased. We should base our cholesterol levels on those found in other animals species….yes, of course we should. You mean those animal species with an average life expectancy of ten years, for example.
However, this argument is now pretty widely accepted by the medical community. We are all, everyone, living in the West, living in such an ‘unhealthy’ way that our cholesterol levels are unnaturally high. The true normal cholesterol levels is 2.5mmol/l.
Fine, if we re-set normal at 2.5mmol/l we will find that 99% of people dying of heart disease do have a ‘high ‘cholesterol level. Problem sorted, average is no longer normal, and the hypothesis that a high cholesterol level is a risk factor for heart disease is now true.
Hold on, I’ve got an idea…
It may surprise some of you that read this blog that, amongst other things, I still work as a doctor in the jolly old NHS. Yes, one can be a critic and still remain inside the system….although for how long, who knows. In fact, in some ways I am quite establishment, as I sit on the main BMA negotiation committee for GPs, the General Practitioners Committee (GPC). I am also on the Local medial committee (LMC) and local negotiation committee (LNC).
From within the NHS you can more clearly see how the world of medicine is gradually going completely bonkers.
In one of my jobs I do Out of Hours (OOH) General Practice work. That is working in the evenings and weekends. In East Cheshire, where I work, we had a system which was highly rated by patients and everyone who came into contact with it. However, in line with the rest of the country we were told we were now to be incorporated into the Government’s latest and currently stupidest idea, called NHS111. The 111 bit being the single telephone number for people to call for urgent – not 999 care.
NHS111 call handlers get about six weeks training, and are supposed to act as front line troops to direct patients to the correct urgent service. Before this we had nurse triage, with experience nurses dealing with local residents and their health issue. We now have non-medically trained staff given superficial advice on how to go through a treatment algorithm. First question: ‘Are you alive or dead?’ Not quite, but nearly.
At the end of asking ten thousand questions, or so, the call handler reaches the end of the algorithm where it states ‘You must see a GP.’ Actually, not quite true. If there is anything actually wrong, then the call handler tells them to phone an ambulance immediately [Yes, ambulance calls under NHS11 have risen stratospherically]. In my opinion, these people are not doing triage, they are just appointment Clerks.
As we repeatedly warned the Government NHS111 rapidly went wrong. In East Cheshire and many other areas, NHS111 immediately collapsed the moment it went live, and we had to take back all the call handling. Why, primarily because the private providers running the service had so badly underestimated demand that the system went into melt-down, and patients were left waiting for hours to be called back. (Oh the joys of competitive tendering. In order to get the contract you have to bid so low that you cannot actually provide the service).
Anyway, we still get some calls coming through from NHS111 (A system now running in parallel – at double cost – with the old system). With the old system we used to get the key facts e.g. a rash, non-blanching, child floppy, temp 39oC, mother worried. Now we get the following (this is an actual transcript of a very, very simple case, with any patient identifiable data taken out – by me).
As you can see, if you bothered to read it, 99% of this is just meaningless guff, stating irrelevant negative findings. But it does take a considerable amount of time to read. Some of it just made me despair. For example, the report states that: ‘An injury or health problem was the reason for the contact.’ Well really, how completely amazing. Someone calls a health line and they may have an injury or health problem. Who’d a thunk?
This is followed later by…’ An illness or health problem was the main problem.’ Well at least they had narrowed it down from an injury or health problem to an illness or health problem. [So it now seems that illnesses are not health problem?]
What did I actually need to know? I needed to know that a child had a cough that was getting worse. Whilst it is possible to establish this from reading the report (just) other key information was conspicuous by its absence. Past history of asthma, for instance (which this child had) or other respiratory problems? Any medications? That type of thing.
As with most new initiatives in the health service I am now getting swamped with information – but the vast majority of it is completely and utterly useless, and just gets in the way of finding out what I want to know.
This, by the way, was a very small part of the report that the GP (in hours), will receive. They will get about ten more pages of other extraneous guff that they have to wade through. At some point my consultation (the only bit they are interested in) will appear so they will know what I found and what I did – and if they need to do anything. This will not be at the front of the report, no, it will be stuck in the middle, surrounded by information about when the call came in, how long it took to respond, what pathways were used etc. etc. etc. thud.
This, ladies and gentlemen, is the type of nightmare bureaucrat driven nonsense that is turning healthcare in the UK from something local, flexible, and responsive to patient needs, into a flabby form filling, algorithm following, arse-covering exercise. Millions of hours spent producing lengthy reports that have no value; they simply get in the way of providing useful information and de-skill, demotivate and de-professionalise everyone involved.
I imagine the UK is not alone in this. Somehow or another we need to fight back.
[I was contemplating risk the other day, when someone forwarded me an article I wrote a couple of years ago on risk. I think it is still highly relevant to what is happening today with the mangling of medical statistics]
I have only just recovered from the idea that everyone in the whole world over the age of fifty-five should spend the rest of their lives on six different medications, all stuck together in one great big pill. The following was headline from a study in the BMJ.
‘Polypill—A Statin plus 3 Blood Pressure Drugs plus Folic Acid plus Aspirin. Authors claim Polypill would reduce risk of dying from coronary heart disease by 80%. The authors of the polypill article in the BMJ made the claim that taking their polypill would reduce the risk of dying of coronary heart disease (CHD) by 80%.’
You may have seen the non-story about the, yet to be marketed polypill, peddled in the British Medical Journal (BMJ). I was stimulated to look again at the concept of risk.
Whether or not you believe their figures—and I don’t—I sense that this figure of 80% would be taken by most people to mean that eighty out of one hundred people would be saved from death if they took this magic tablet. But this figure, if true, could only possibly be a relative risk reduction. And a relative risk reduction means almost nothing, by itself.
However, because everyone’s eyes glaze over whenever you start talking about statistics, most researchers manage to get away with using relative risk reduction figures when, in reality, they should be shot for doing so. Now, here’s a challenge. The challenge to make a short article about statistics interesting. Okay, that’s not possible. But maybe a little bit interesting?
You must know the time period, and the absolute risk, for the relative risk to have any meaning
When you talk about a risk, you need to know the absolute risk of a thing happening. For example, the risk of getting struck by lightning. I don’t actually know what this risk is, but I would imagine it is about one in five million. But again, that figure means little unless you put a time scale on it. Is this a one in five million risk over a hundred years, or one year, or a day? If you don’t put a time scale in, you can claim pretty much anything you like.
For example an astronomer could attempt to shock you by stating that ‘The Earth will be hit by a big Asteroid. This is one hundred per-cent certain.’ – stunning announcement from A.N. Astronomer. Read all about it. And of course, this is true. The Earth will be hit by a big Asteroid, sometime in the next three billion years or so. The odds ratio for this event is 1 = 100% certain. I am even willing to take a bet on it. What you probably want to know is however, is, what is the likelihood of this happening in my lifetime. Sorry, no idea.
Anyway, I hope this makes it clear that you must define risk in two ways, the possibility of the nasty thing happening, and the time period during which it is likely that the thing will happen. With lightening strikes, I would guess this is about a one in five million risk, over a five year period. Not high.
However, whilst the time factor is important, people don’t just bend statistics by ignoring the time factor. What also happens is that people inflate the risk by using relative instead of absolute risks.
For example, the chances of dying of lung cancer, for a non-smoker, are about 0.1% (lifetime risk). If, however, you live with a heavy smoker, your chances will increase to about 0.15%. (These figures are for illustration only, and are not completely accurate).
Now, you can report this in two ways. You can state that passive smoking can increase the risk of lung cancer by 0.05% – one in two thousand. Or, you can state that passive smoking increases the risk of lung cancer by fifty per cent (0.15% vs 0.1%). Both figures are correct. One is increase in absolute risk, the second the increase in relative risk.
If you are an anti-smoking zealot, then I would imagine you would prefer to highlight the second figure. The relative risk figure. And when it comes to reducing cardiovascular risk, exactly the same procedure is used (in reverse).
Let’s say that the chance of dying of CHD over the next five years, in a healthy fifty-five year-old, is 1%. By reducing this risk to 0.2%, you can claim to have reduced the relative risk of dying of CHD by 80%. The absolute risk reduction is 0.8%. Mangling statistics is easy when you know how. It’s even fun.
Anyway, now you know the difference between a relative risk and an absolute risk, and I hope this makes it easier for you to hack your way through the misinformation that spews forth from the great medical research machine.
By the way, I believe the Polypill will achieve a 0.00% absolute and relative risk reduction. But we shall see.
A few weeks ago, a sixth year student at Westminster School sent me an essay she had written on cholesterol, and why it does not cause CHD. She wants to go to medical school. No one made her do any of this. She just looked at the evidence and made her mind up. She wrote me this e-mail
Dear Dr Kendrick,
I am a final year student at Westminster School who intends to study medicine. I am extremely interested in your research and reading your book enthused my and led me to spend a large portion of my time researching studies which you and other authors on the same topic have referenced. The Chief Medical officer came to speak to us today and after her talk I quizzed her about what I have read in your book as well as a large wealth of research I have done myself. (Attached, if you care to look, is a copy of an essay I wrote which won the top prize in school essay competition based on this research). She was extremely defensive of the cholesterol causes heart disease hypothesis and claimed that NICE had on a population level declared this to be the case. She said that the evidence did not add up on a small study level, but when studies were put together (I assume by NICE) that the conclusion is in favour of cholesterol causing CHD.
I would love to know your thoughts on this and where I can find this population based evidence.
Kind regards,
Francesca Greenstreet
I wrote back to her, to say that there was no population based evidence. Or, if there was, it very clearly demonstrated no link between cholesterol levels and heart disease. The Chief Medical Officer was just blustering – as most people do when confronted with someone who dares to question medical dogma.
I thought her essay was extremely well written and makes all the points that I have been making for years. It is just gratifying to see that the evidence on cholesterol and heart disease is clear to anyone with a brain.
The American government, the British government and the NHS, three venerable bodies respected as sources of dietary advice, currently recommend a diet low in saturated fat and cholesterol.[1] The predominant reason this advice is given is the accepted belief held within the scientific community that high serum cholesterol levels are linked causally with the accumulation and build up of atheromas which lead to atherosclerosis and Coronary Heart Disease (CHD).
The commonly accepted and taught theory which links cholesterol to heart disease, the Lipid Hypothesis, states that cholesterol is carried from the liver to the rest of the body’s cells in Low Density Lipoproteins (LDLs) and carried back from the rest of the body’s cells to the liver in High Density Lipoproteins (HDLs). After being transported back to the liver by HDLs, Cholesterol is broken down by the liver or passes out of the body as a waste product. The Lipid Hypothesis states that eating saturated fat raises LDL levels. The cholesterol from LDLs forms fatty deposits, atheromas, which build up beneath the endothelium of the arteries. The build up of atheromas narrows the arteries and pieces of the atheromas can break off and become lodged in narrower arteries .Clots can form in the narrowed arteries which prevent blood flow and can starve organs of oxygen and nutrients. When clots or blockages form in the coronary arteries, necrosis occurs. This leaves part of the heart muscle not contracting and relaxing and can lead to a myocardial infarction.[2]

Figure 1: Sudan-stained aorta of a rabbit fed 61 egg yolks over a 70-day period, showing lesions in red.
The Lipid Hypothesis was brought to attention following a series of studies, the first of which was carried out by Anitschkow, a Russian scientist, in 1913. Anitschkow fed rabbits a diet of purified cholesterol dissolved in sunflower oil and examined the cells and the arteries of the rabbits after killing them. [3] Rabbits which were fed the purified cholesterol were found to have vascular lesions which bore a close resemblance to atheromas found in humans (Figure 1). Following Anitschkow’s study, Dr John Gofman led a team to similar findings and hypothesized that serum cholesterol was the cause of the lesions developing.[4] The similarity of the lesions to those found in humans suffering from CHD was catalytic in the formation of theories that a high cholesterol diet might be linked to CHD in humans.
The ideas behind the Lipid Hypothesis were formalised by Ancel Keys when, in a study in 1953, he used data from six countries to show a direct link between the percentage calories from fat in the average diet and the number of CHD deaths per 1000.[5] Furthermore, he found the incidence of CHD deaths in those six countries was best predicted by the intake of saturated fat.[6]
However, not all scientists and physicians are in agreement with the Lipid Hypothesis. Regarding Anitschkow’s rabbit study, it has been pointed out that cholesterol does not form part of the natural diet of a rabbit and thus it is possible that the rabbits had an allergic reaction to the high cholesterol diet, or that they were otherwise incapable of processing the chemical. It is significant to note that similar experiments carried out on dogs and rats showed that a rise in blood cholesterol did not lead to a rise in atherosclerosis.[7] This is potentially due to the fact that dogs and rats, unlike rabbits, consume cholesterol as part of their natural diet. The lack of cholesterol in a rabbit’s natural diet, combined with the failure to replicate the findings in dogs or rats, whose natural diets are much more similar to our own, is a significant flaw in the reasoning behind Anitschkow and Gofman’s conclusion: that a high cholesterol diet is linked to atherosclerosis in humans.
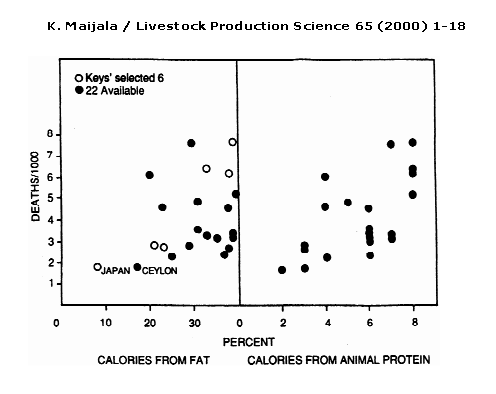
Figure 2: Keys’ (1953) selection to show relationship of fat intake to heart disease deaths of 55–59 yr. old men in 1951–53 (open circles left)and the 15 other available countries (closed circles). The relation of heart diseases to animal protein intake is on the right (Mann, 1993). (Adapted from WHO Ann. Epid. and Vital Statistics).
Another flaw in the Lipid Hypothesis is that Ancel Keys selected with purpose the countries for which he presented data in his study in 1953, rather than choosing them at random. “Yerushalmy and Hilleboe (1957) observed that Keys would have had available data from 22 countries, which would have given a much weaker correlation “(Figure 2).[8]
Figure 2 shows a very weak correlation between deaths per 1000 (from CHD) and percentage of calories from fat when all 22 countries are plotted on the same graph. It is interesting to note that the correlation between deaths per 1000 (from CHD) and percentage of calories from animal protein has a similar and even slightly stronger correlation than between deaths per 1000 (from CHD) and percentage of calories from fat. All of this data would have been available to Keys, so his focus on the link between percentage of calories from fat and the number of deaths per 1000 (from CHD) is curious.
The data sample presented by Keys gives a correlation of coefficient of +0.84, a strong positive correlation, whereas “in the simulation study by Wood (1981) on the consumption statistics of 21 countries a total of 116280 different samples of six countries were found, and the correlation between consumption of animal fat and CHD mortality varied from -0.9 to +0.9, the average being -0.04.”[9] Such a difference in correlation coefficients between similar studies indicates some bias in Keys’ selection of the six countries or insufficient data, since Wood’s study uses many more countries and therefore is more likely to be accurate. As it is obvious that Keys had sufficient access to data from the 22 countries, it seems that his selection was biased.
There have also been many studies which investigate serum cholesterol level in relation to atherosclerosis and CHD in Humans rather than in animals. A notable example is the study led by Paterson entitled: “Serum Cholesterol Levels in Human Atherosclerosis”. 800 patients who were permenantly confined to hospitals and 100 war veterans who were in hospital for dimiciliary care were given 2500-3000 calories a day in their daily diet, of which 25 to 35% was derived from fat. Serum cholesterol was determined annually or semi-annually and when any patients died, the severity of atherosclerosis was determined using six differnet criteria: crude morphological grading, measurement of the thickness of the largest plaque, determinations of the total lipid content, lipid concentration, total calcium content and calcium concentration. Figure 3 shows a graph showing the abscence of a correlation between Serum Cholesterol in mg.% and Total Lipid in Mg. This shows that for the criterium of total lipid content, there is no correlation in the age group of 60-69 years.
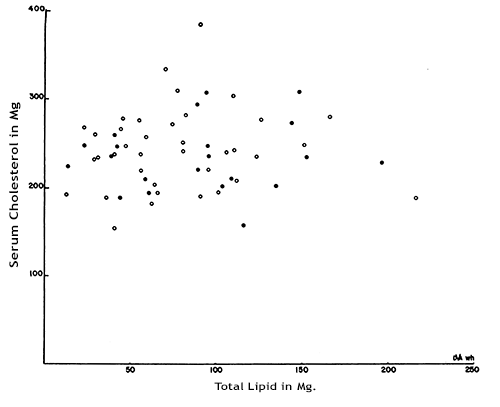
Figure 3: Total coronary artery lipid and serum cholesterol levels in patients 60-69 years. The open circles represent cases without complications of coronary atherosclerosis; the closed circles, cases with complications.
Similar findings were observed in the other age groups with a significant number of participants (70-79 and 80-89). The study concludes: “In the 58 cases in the age group 60-69 years, significant relationships between the serum cholesterol and the severity of the disease were found only once in 40 statistical analyses, and the complications of atherosclerosis were just as frequent in cases with low serum cholesterol levels (150-199 mg. %) as in cases with moderately high ones (250-299 mg. %).”[10]Considering the emphasis from the government and the NHS to reduce cholesterol and saturated fat intake because cholesterol causes heart attacks, this seems to be a remarkably weak correlation.
The Paterson study was not alone in its findings: Sigurd Nitter-Hauge and Ivar Enge published a study in The British Heart Journal in 1973 which reported: “No significant correlation was found when total coronary arterial score was correlated to serum cholesterol values or to triglycerides.”[11]
Not only is there strong evidence to show that serum cholesterol levels have no link to atherosclerosis, but there is also strong evidence to suggest that high cholesterol consumption does not raise blood cholesterol levels. The Framingham Heart Study, which set out to prove that eating more cholesterol in your diet increases your blood cholesterol levels, in fact showed that there was minimal difference in the blood cholesterol levels of the subjects despite subjects consuming cholesterol in widely varying amounts. [12] Scientists working on the Framingham Heart Study also studied the intake of saturated fats but eventually concluded: “There is, in short, no suggestion of any relation between diet and the subsequent development of CHD in the study group.”[13] It is difficult to stress the importance of this finding enough: there was no connection found whatsoever between diet and the development of CHD.
Further evidence that eating a diet high in saturated fat does not lead to CHD was published in The American Journal of Clinical Nutrition in 1981. The study compared the diets of two populations of Polynesians living on atolls near the equator. It also assesses the effect the diets have on the serum cholesterol levels in the populations. One of the populations, the Tokelauans, obtained a very high percentage of energy from coconut (high in saturated fat) compared to the Pukapukans, 63% compared with 34%. The Tokelauans had serum cholesterol levels 35-40mg higher than the Pukapukans. However , “vascular disease is uncommon in both populations and there is no evidence of the high saturated fat intake having a harmful effect in these populations.”[14]
Taking all these studies into account, it would appear that not only does having a high serum cholesterol level not have any connection to CHD, but that a diet high in cholesterol does not lead to high blood cholesterol levels and that a diet high in saturated fat does not have any link to CHD.
One final argument used to support the Lipid Hypothesis is the apparent effectiveness of statins in treating CHD. If, so the argument goes, statins reduce levels of serum cholesterol and they also reduce the risk of CHD, then reducing serum cholesterol levels must be the reason for the lower incidence of CHD. However, this reasoning contains two fallacies: firstly it assumes that statins have been shown to reduce the risk of CHD, and secondly it assumes that lowering serum cholesterol levels is the only effect of statins that could lower the incidence of CHD.
Both of these assumptions are false. A study was carried out by the University of British Columbia, part of the not-for-profit Cochrane collaboration, which concluded: “If cardiovascular serious adverse effects are viewd in isolation, 71 primary prevention patients have to be treated with a statin for 3 to 5 years to prevent one myocardial infarction or stroke.”[15] Small mortality benefits from statins have been shown for high-risk middle aged men.[16], [17] However, these trends are not seen in women and the elderly.15, 16 Even an advertisement for LIPITOR (atorvastatin calcium), one of the best-selling statins in America, has a disclaimer which includes: “LIPTOR has not been shown to prevent heart disease or heart attacks.”[18]
For the small minority of people who are protected by statins, there is another explanation. Statins have been repeatedly shown to act as “potent anti-inflammatory” agents in patients with cardio vascular disease[19]. The reason for their effects in reducing incidence of CHD could be due to those effects rather than the reduction of serum cholesterol levels. This means that it is innappropriate to use the limited protection against CHD by statins as evidence for high serum cholesterol levels being a cause of CHD.
Gathering together the arguments made in this essay, we can conclude that it is very likely that there is absolutely no causal correlation between high cholesterol, either in the serum or in the diet, and CHD. Nor is there any causal correlation between a diet high in saturated fat and CHD. The emphasis placed on the Lipid Hypothesis by the government and other organisations concerned with public health is potentially due to the inital panic after the publication of Keys’ and Anitschkow’s studies. The feeling of urgency to act in order to prevent ever increasing numbers of deaths from CHD led to premature acceptance of the Lipid Hypothesis without sufficient evidence. The long term effect of this view has been the demonisation of diets high in saturated fat and cholesterol without sufficient justification from otherwise reputable organisations for the past thirty years.
Word count : 2431 words
(excluding title, name, biliograph and references)
Bibliography
“Trick and Treat” (Barry Grroves,2008)
“The Great Cholesterol Con” (Dr Malcolm Kendrick, 2007)
“The Cholesterol Myths” (Uffe Ravnskov, M.D., Ph.D., 2000)
“Seven Countries: A Multivariate Analysis of Death and Coronary Heart Disease” (Ancel Keys, 1980, Introduction, p. 1-17)
KIM CRAMER, SVEN PAULIN, LARS WORKÖ, 1966. Coronary Angiographic Findings in Correlation with Age, Body Weight, Blood Pressure, Serum Lipids, and Smoking Habits. Circulation; 33:888-900
U. RAVNSKOV, 2002. Is Atherosclerosis caused by high cholesterol?. Q J Med; 95:397-403
Prevention of Coronary Heart Disease. British Medical Journal , 21 September 1968; No. 5620, p.689
Sigurd Nitter-Hauge, Ivar Enge, 1973. Relation between blood lipid levels and angiographically evaluated obstructions in coronary arteries British Heart Journal. 35, 791-795.
J. R. CROUSE, J. F. TOOLE, W. M. MCKINNEY, M. B. DIGNAN, G. HOWARD, F. R. KAHL, M. R. MCMAHN, G. H. HARPOLD, 1987. Risk factors for extracranial carotid atherosclerosis. Stroke; 18:990-996
Mukesh K. Jain, Paul M. Ridker, 2005. Anti-Inflammatory Effects of Statins: Clinical Evidence and Basic Mechanisms, Nature Reviews Drug Discovery 4. 977-987
Ian A. Prior, M.D., F.R.C.P., F.R.A.C.P., Flora Davidson, B.H.Sc., Clare E. Salmond, M.Sc., and Z. Czochanska, DIP.AG., 1981. Cholesterol, coconuts, and diet on Polynesian atolls: a natural experiment: the Pukapuka and Tokelau Island studies. The American Journal of Clinical Nutrition 34, p. 1552-1561.
Kannel WB, Gordon T., 1970.The Framingham Diet Study: diet and the regulations of serum cholesterol (Sect 24). Washington DC, Dept of Health, Education and Welfare.
J.C. PATERSON, M.D., LUCY DYER, M.Sc. and E.C. ARMSTRONG, M.D., London, Ont., 1960. Serum Cholesterol Levels in Human Atherosclerosis. Canad. M. A. J., 1960, vol. 82
Scandinavian Simvastatin Survival Study Group, 1994. Randomised trial of cholesterol lowering in 4444 patients with CHD: the Scandinavian Simvastatin Survival Study (4S). Lancet; 344: 1383-1389
Kalle Maijala, 2000. Cow milk and human development and well-being. Livestock Production Science 65 1–18
Daniel Steinberg, 2004. Review series: The Pathogenesis of Atherosclerosis. An interpretive history of the cholesterol controversy: part I, The Journal of Lipid Research, 45, 1583-1593.
GOFMAN, J.W.;LINDGREN, F.; ELLIOT, H.; MANTZ, W.; HEWITT, J.; STRISOWER,B.; HERRING, V.; LYON, T.P., 1950.The role of lipids and lipoproteins in atherosclerosis, American Association for the Advancement of Science Vol. 111pp. 166-171; 186
National Service Framework for Coronary Heart Disease – Modern Standards and Service Models, March 2000.
http://www.nhs.uk/conditions/cholesterol/pages/introduction.aspx
http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001224/
http://www.health.gov/dietaryguidelines/dga2000/document/choose.htm
Figure 1: Daniel Steinberg, 2004. Review series: The Pathogenesis of Atherosclerosis. An interpretive history of the cholesterol controversy: part I, The Journal of Lipid Research, 45, 1583-1593.
Figure 2: Kalle Maijala, Cow milk and human development and well-being, Livestock Production Science 65 (2000) 1–18
Figure 3: J.C. PATERSON, M.D., LUCY DYER, M.Sc. and E.C. ARMSTRONG, M.D., London, Ont., 1960. Serum Cholesterol Levels in Human Atherosclerosis. Canad. M. A. J., 1960, vol. 82
[1] http://www.health.gov/dietaryguidelines/dga2000/document/choose.htm
[2] http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001224/
[3] Daniel Steinberg, 2004. Review series: The Pathogenesis of Atherosclerosis. An interpretive history of the cholesterol controversy: part I, The Journal of Lipid Research, 45, 1583-1593.
[4] GOFMAN, J.W.;LINDGREN, F.; ELLIOT, H.; MANTZ, W.; HEWITT, J.; STRISOWER,B.; HERRING, V.; LYON, T.P., 1950.The role of lipids and lipoproteins in atherosclerosis, American Association for the Advancement of Science Vol. 111pp. 166-171; 186
[5] “Trick and Treat” (Barry Groves, 2008, p.61-62)
[6] “The Cholesterol Myths” (Uffe Ravnskov, M.D., Ph.D., 2000, out of print – available at: http://www.ravnskov.nu/myth4.htm)
[7] “Trick and Treat” (Barry Groves, 2008, p.59)
[8] Kalle Maijala, Cow milk and human development and well-being, Livestock Production Science 65 (2000) 1–18
[9] Kalle Maijala, 2000. Cow milk and human development and well-being. Livestock Production Science 65 1–18
[10] J.C. PATERSON, M.D., LUCY DYER, M.Sc. and E.C. ARMSTRONG, M.D., London, Ont., 1960. Serum Cholesterol Levels in Human Atherosclerosis. Canad. M. A. J., 1960, vol. 82
[11] Sigurd Nitter-Hauge, Ivar Enge, 1973. Relation between blood lipid levels and angiographically evaluated obstructions in coronary arteries British Heart Journal. 35, 791-795.
[12]“Trick and Treat” (Barry Groves, 2008, p.63)
[13] Kannel WB, Gordon T., 1970.The Framingham Diet Study: diet and the regulations of serum cholesterol (Sect 24). Washington DC, Dept of Health, Education and Welfare.
[14] Ian A. Prior, M.D., F.R.C.P., F.R.A.C.P., Flora Davidson, B.H.Sc., Clare E. Salmond, M.Sc., and Z. Czochanska, DIP.AG., 1981. Cholesterol, coconuts, and diet on Polynesian atolls: a natural experiment: the Pukapuka and Tokelau Island studies. The American Journal of Clinical Nutrition 34, pp. 1552-1561.
[15] “The Great Cholesterol Con” (Dr Malcolm Kendrick, 2007, p.164-165)
[16] “Trick and Treat (Barry Groves, 2008, p.52)
[17] Scandinavian Simvastatin Survival Study Group, 1994. Randomised trial of cholesterol lowering in 4444 patients with CHD: the Scandinavian Simvastatin Survival Study (4S). Lancet; 344: 1383-1389
[18] http://www.westonaprice.org/cardiovascular-disease/dangers-of-statin-drugs
[19] Mukesh K. Jain, Paul M. Ridker, 2005. Anti-Inflammatory Effects of Statins: Clinical Evidence and Basic Mechanisms, Nature Reviews Drug Discovery 4. 977-987
I recognise that I spent a lot of time telling people what does not cause heart disease, and what does not protect against heart disease. My sister told me… ‘well, what advice would you give people, then?’ I usually shrug my shoulders and reply ‘there is no shortage of advice around, I don’t think I need to add to the daily bombardment.’
However, I shall break the habit of a lifetime and, with slight trepidation, announce that I strongly believe that Potassium is good for you. If you consume more of it you will, most likely, live both longer and in better health.
How much should you consume? A couple of extra grams a day should do the trick. Having said this, I do recognise that most people will not have the faintest idea how much potassium they consume and, frankly, neither do I. But you are probably not consuming enough, and your kidneys will easily get rid of any excess.
For those who are not keen on bananas, spinach and broccoli, and other foods high in potassium, you could take it as a tablet. Potassium bicarbonate or potassium citrate appears to be the best formulation. Depending on which brand you decide to buy, it should cost about £15 – 20/year.
Why this sudden potassiumophilia? Well, there is a growing body of research which points to the fact that potassium is very good for you. The first time I became aware that it might be good for you was when I first looked at the Scottish Heart Health study. The researchers looked at twenty seven different ‘factors’ they thought might cause, or protect against, heart disease – and overall mortality. The authors noted that:
“[There was] an unexpectedly powerful protective relation of dietary potassium to all-cause mortality,” the study concluded.
The paper showed that:
The study can most easily be found here http://www.ncbi.nlm.nih.gov/pubmed/9314758
I immediately liked this finding. Mainly because it was almost completely unexpected, and unexpected findings are always far more likely to be correct than expected findings. Also, this was a very large effect indeed. It turned out that increased potassium consumption was very nearly as protective as smoking was damaging.
Of course, this was an observational study, so I filed it under – most interesting – but did nothing much more about it. As the authors said themselves: ‘ Potassium excretion was very significantly related to risk of death from all causes, having a protective role, whereas its role in coronary events was weaker and that of sodium excretion weak and even paradoxical. These results are unifactorial, without correction other than for age and sex. Our findings need corroboration from elsewhere and more detailed analysis with more events from longer follow-up.’
Since then, a large number of other studies have followed up, and appear to have confirmed that potassium has considerable health benefits. Some of these studies were not just observational, they were interventional. Here is summary of the potential beneficial effects. Potassium:
These benefits have been confirmed in a number of different studies. However, as this is a blog, I am not going to turn it into a medical paper and provide references for every statement, so I will stick to a couple of referenced studies. (If enough people are interested I can point you at additional papers).
With regard to blood pressure, a study published in 1997 found that adding roughly 2 grams (2000 mg) of potassium per day lowered blood pressure in older people by 15/8 mm Hg. As good, if not better, than any antihypertensive drug1. And with no side-effects at all.
When it comes to stroke, it has been found that having a low potassium level is a very potent risk factor for both bleeding (haemorrhagic) and clotting (ischaemic strokes). In an American study it was found that in those with low potassium levels the relative risk of ischaemic stroke increased by 206%. The relative risk increased by 329% for haemorrhagic stroke2.
Admittedly, these two studies were done in people with high blood pressure to start with, but these effects are also found in healthy people. However, to my mind, the most important thing about potassium is that I cannot find any study, anywhere, which suggests that increasing potassium consumption may be harmful. In short, it seems to be something that does only good.
I do recognise that a lot of doctors will shudder at the thought of adding potassium to the diet, as they have all been taught that a high potassium level is something terribly dangerous. A condition that needs immediate treatment, or else it will cause arrhythmias and death.
It is true that you need to be careful of adding potassium to the diet of patients taking medications that can raise potassium levels. These are mainly drugs used to lower blood pressure. However, even in this group the risk of overdosing on potassium is exceedingly small. For everyone else the risk seems to be zero. This is why I now recommend potassium supplementation as a good way to live a longer, healthier life.
My goodness, I think this is the first time I have ever recommended a dietary supplement. Must go and lie down.
1: ‘Long term potassium supplementation lowers blood pressure in elderly hypertensive subjects’ Fotherby M.D. et al: Int J Clin Practice 1997 41(4): 219 – 222)
2: Smith NL, et al: ‘Serum potassium and stroke risk among treated hypertensive adults.’ Am J Hypertens. 2003 Oct;16(10):806-13
‘Don’t trouble me with the facts my mind is made up.’ Foghorn Leghorn
So, now the great obesity initiative is to be rolled out across the UK, driven by the UK Academy of Medical Royal Colleges (AOMRC). Some time ago I wrote a blog in which I outlined exactly what they would say….and lo, they have said it. The main recommendations are:
There is more such stuff, mainly about taxing and banning. It was all wearyingly predictable. This is exactly what the ‘experts’ have been saying for the last thirty years – this time with an ‘amazing 50% added legislation’. If what you have been doing doesn’t work. Then redouble your efforts, with added punishments. That’ll work. Just like prohibition worked in the states.
Even if these were the right things to do, and had some chance of working, I would not support them. Social control through legislation absolutely must be the last resort of a democratic society. Making people do what is good for them….hmmm. Aldous Huxley had something to say on this matter. That, however, is a broader issue.
Looking specifically at some of the recommendation, starting with the concept of putting a duty on all sugary soft drinks. This will inevitably mean that people will drink more ‘diet’ drinks- without sugar in them. Will this be a good idea? Well, here is a study from the USA, and the conclusions thereof:
‘Findings from this cohort of adolescents yielded strong evidence for cross-sectional associations between diet soda consumption with weight status in both boys and girls. Specifically, youth who consumed diet soda were more likely to have a higher BMI and PBF (percentage body fat) compared to those who did not.’ http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3402912/
This is consistent with other studies which show that drinking ‘diet’ soda is strongly associated with a greater risk of obesity than drinking sugary soft drinks. Such evidence is not hard to find. It is rather more difficult to interpret, but that is – again – another issue.
As for trying to reduce saturated fat consumption. I can say here and now that there is not one molecule of evidence to suggest that saturated fat consumption causes obesity. Not one. As for impact on heart disease….again, nothing.
My favourite quote on this comes from the Framingham study. The single most influential study on heart disease in the world.
‘In Framingham, Massachusetts, the more saturated fat one ate, the more cholesterol one ate, the more calories on ate, the lower people’s serum cholesterol.’ Dr William Castelli, Director of the Framingham study. 1992
[Not that I think cholesterol has anything to do with heart disease, but for those of a conventional view point, lowering cholesterol is supposed to be a good thing].
As for salt….where did this come from? I have yet to see any evidence linking increased salt intake to obesity. And why would it. How could it? Salt has no calories in it; it has no impact on any metabolic parameters that I know of. And I would challenge anyone to show me any evidence from any controlled randomised study that salt restriction (in health adults) has any benefits on cardiovascular disease.
I could go on, and on. But the main point is that the ‘experts’ are trapped with a mind-set that they cannot and will not change. Like all the best zealots, they know what the causes of obesity are. To misquote from Terminator.
‘Listen, and understand. That obesity initiative is out there. It can’t be bargained with. It can’t be reasoned with. It doesn’t feel pity, or remorse, or fear. And it absolutely will not stop, ever, until you are dead.’
Energy cannot be created or destroyed, merely converted to a different form. And matter, as we all know, is a form of highly concentrated energy.
Looking up Wikipedia I discovered that one gram of matter contains 9.0×1013 joules. (Theoretical total mass-energy of 1 gram of matter). This is approximately the same energy yield as the fat man atomic bomb used in World War Two.
However according to Flora and the British Heart Foundation (who have joined forces to inform the world of the terrors of saturated fat, and cholesterol, and the benefits of Flora), ten grams of matter can easily be gained or lost on the average kitchen stove.
How so, you may wonder. Surely, losing ten grams of matter would create a serious risk of releasing enough energy to wipe out a major city, and all residents contained within. Not so, it seems that if you fry an egg, it weighs 60grams. However, if you boil an egg, it weighs 50grams. See the Flora BHF poster for further detail on this remarkable fact: http://www.flora.com/PDFAuth.aspx?redirectURL=/Resources/others/pdf/HCPPdf/Fat%20Swaps.pdf
Ten grams of matter can simply disappear when you boil an egg? Quite remarkable. I think we should ask CERN to close down the large hadron collider straight away. Their search for the Higgs Boson, the reason why mass exists, and naïve reliance the Unified Field Theory itself, are clearly misguided.
All you need do, to disprove the existence of the mass/energy equation is boil an egg, and ten grams of matter simply disappear. 900,000,000,000,000 joules of energy……just gone. How remarkable is that.
But the wonders of Flora and the BHF do not stop with disproving the existence of the Higgs Boson, and the uselessness of all theoretical physicists. They can also do maths which prove that you can alter the amount of matter contained within the egg as well.
According to this self-same remarkable British Heart Foundation/Flora poster, a fried egg contains 2.4 grams of ‘bad’ fat, and 4.5 grams of good fat. On the other hand a boiled egg contains a mere 1.6 grams of ‘bad’ fat and 3.0 grams of good fat. So, eating a boiled egg means that you reduce intake of ‘bad’ fat by 0.8 grams. (Bad fat is saturated fat, by the way).
For those of you with a mathematical bent, you may have noticed that if a fried egg weighs 60g, and boiled egg weighs 50g, it is 20% heavier. Yet it manages to contain 50% more bad fat (2.4g/1.6g = 1.5). Aha, you might be thinking, when you fry an egg good fat (polyunsaturated), is converted to saturated fat – or something of the sort.
Well, clearly not so (and biologically impossible). Because a fried egg also contains 4.5 grams of good fat, whilst a boiled egg contains 3.0 grams of good fat. So, the ratio of good fat in a fried egg and a boiled egg is also 1.5 (3.0/1.5 = 1.5). In other words, exactly the same ratio as in a fried egg.
So, not only do fried eggs weigh more – 20% more. They also contain significantly more good and bad fat – 50%, at the same time. Bringing all this information together we find that, according to the scientists at Flora and the BHF, a fried egg ends up 1.2 times as massive as boiled eggs and contains 1.5 times as much bad and good fat at the same time. Yes, of course.
My solution to all this is simple, sneak up on the eggs from behind, and damn well fry the ones that thought they were going to be boiled. In this way you can reduce bad fat in a fried egg from 2.4 grams to 1.6 grams. Hah! I bet the scientists in Flora never thought of that – did they.
I am so glad that the British Heart Foundation have brought keen scientific rigor to their partnership with Flora. If I wasn’t laughing, I’d be crying.
At what point, exactly, does credibility snap? When does the difference between what we are told, and what we observe, reach such a state of dissonance that it is no longer possible to believe both. Sometimes it seems the answer is ….never.
Here is one example. The clinical trials on statins found that they have virtually no adverse effects. Or, to be a little more accurate, that adverse events were virtually identical to placebo. Here, for example, is part of the press release from the Heart Protection Study (HPS).This was the last major placebo controlled statin study done in people with already diagnosed cardiovascular disease.
As the benefits of statins are now thought so wonderful it would be considered unethical to do a placebo controlled study anymore. You would be withholding statins from people who need them. Which means that you are not going to get any more evidence in this area – ever again. The HPS results were published around ten years ago, and the press release contained the following
‘Although muscle pain was reported by the participants, this happened about as commonly among those allocated the active simvastatin as among those allocated the placebo tablets. Despite 20,536 randomised patients having been followed for an average of five years, blood tests among people reporting muscle symptoms found only 11 simvastatin-allocated patients and 6 placebo-allocated patients with a rise in the muscle enzyme creatine kinase (CK) to more than 10 times the upper limit of normal Of these, 14 met the definition for “myopathy” (i.e. muscle symptoms associated with such CK elevations) of whom 10 were in the simvastatin group and 4 in the placebo group.’
http://www.ctsu.ox.ac.uk/~hps/June02QandA.shtml
Teasing these figures out a little more it seems that an extra six people taking simvastatin suffered muscle ‘problems’ than those taking the placebo. This is six people, out of more than ten thousand taking simvastatin. This represents in one thousand seven hundred and eight 1/1708 (over five years).
If this were true, then muscle problems should be exceedingly rare. The average GP with about two hundred of their fifteen hundred patients taking a statin should see a patient with muscle pains/problems about once every twenty five years. At this rate, you would not even know you had a problem.
Yet, wrapped around my copy of the BMJ last week was an advert for rosuvastatin [Crestor]. The strap line shouted out ‘Myalgia on his initial statin?’ [Myalgia is the medical word for muscle pain]. The main message the advert was… ‘If your patient was suffering muscle pains on their initial statin, they should switch to Crestor 5mg.’
Their ‘initial statin’ will almost certainly be Simvastatin 40mg. The drug, and the dose, used in the HPS study. The same drug, and the same dose recommended by the National Institute of Clinical Excellence (NICE).
Now, you do not run an expensive advertising campaign without doing a lot of market research first. What the market research must have told AstraZeneca – who make Crestor – is that a lot of people are suffering muscle pains on 40mg simvastatin.
Which means that simvastatin, which caused no discernible increase in muscle pains in the clinical study…… actually creates such a massive burden of muscle problems that a pharmaceutical campaign is running a major advertising campaign highlighting this, exact, adverse event.
What does this tell us, gentle reader? It tells us many things. Some of which would be considerable slanderous if I said them out loud. The most outstanding thing it tells me is that, although we have all been repeatedly informed that statins have no more side-effects than placebo, I now find that AstraZeneca encouraging doctors to switch statins due to the burden of side-effects.
F Scott Fitzgerald opined that …“The test of a first-rate intelligence is the ability to hold two opposed ideas in the mind at the same time, and still retain the ability to function.’
I would suggest that there comes a point where you have to decide between which idea is right, and which is wrong. With regard to statins, I did this many years ago when I recognised that they cause a gigantic burden of adverse effects, with muscle pain the single most outstanding. I knew that the clinical trials had somehow or another managed to bury this fact.
Yet, when I speak to most doctors they continue to tell me that statins have very few side-effects, as do most opinion leaders. This belief, whilst AstraZeneca starts up an advertising campaign based on side-effects reported by doctors. F Scott Fitzgerland would be impressed by all these first class intellects. I just despair of them.
Now that Ben Goldacre’s book Bad Pharma has come out, exposing the fact that much medical research is controlled by, and manipulated by, the pharmaceutical industry, I thought I should revisit a short article I wrote six years ago:
Gosh, Really, You Don’t Say:
Sometimes you read something of such blinding obviousness (if that is actually a word), that you wonder why anyone even bothered writing it at all. You know the sort of thing – ‘constant criticism of children does not lead to a sense of self-worth.’ ‘A centralized command economy does not create wealth for citizens.’
But the blindingly obvious can be critically important depending on who says it. I can bang on and on about the fact that medical journals have basically turned themselves into advertorials for the pharmaceutical industry, and be readily dismissed as a fringe lunatic.
However when Richard Smith, editor of the British Medical Journal (BMJ) for many years who resigned last year, says it, then it would seem that even the cosy ‘establishment’ may be starting to feel the first cold fingers of doubt creeping in. Perhaps things really have started to go too far. So read and enjoy a short section from an article in the BMJ, 21st May 2005.
“Medical journals are no more than ‘an extension of the marketing arm of pharmaceutical companies’ because a large proportion of their revenue comes from drug advertisements and reprints of company funded trials, claims former BMJ editor, Richard Smith.
“Dr. Smith argues that although medical journals make a sizeable income from drug advertisements this is the least of their ‘corrupting form of dependence’ on the industry, since the advertisements are ‘there for all to see and criticize’.
“Dr Smith’s strongest criticism is levelled at the fact that journals publish clinical trials that are funded by the industry. Unlike advertisements, trials are seen by readers as the highest form of evidence, he says. Trials funded by drug companies rarely produce unfavourable results and make up between two thirds and three quarters of the trials published in key journals.
“The potential profits from reprints of such a trial can run to $1m (£0.5m; €0.8m), says Dr Smith. And it is this potential income that can have the biggest corrupting influence on a journal because many editors are charged with ensuring their journal makes a profit.
“Editors may be confronted by ‘a frighteningly stark conflict of interest’, writes Dr Smith They may be forced to choose between publishing a trial that will bring $100,000 of profit or meet their end of year budget by making a member of staff redundant.”
Will this article in the BMJ change anything?….. You have GOT to be joking……
And you know what changed in the last six years. You got it. Nothing.
A friendly journalist asked me if I had seen the paper from Norway which looked at cholesterol levels heart disease and overall mortality. Amazingly, as I have sensitive antennae for such things, I had not heard of the HUNT 2 study. Not quite so amazingly, no-one else seems to have heard of it either.
Strange, in a world where the most ridiculous dietary studies are plastered across the front pages of the newspapers, and get top billing on the BBC. You know the type of thing…. Eating red meat regularly ‘dramatically increases the risk of death from heart disease’ A typical headline from the Daily Mail.
But when a ten year study looking at cholesterol levels, overall morality, and heart disease comes out….Silence. I wonder why? Perhaps it has something to do with the results. (See below) http://onlinelibrary.wiley.com/doi/10.1111/j.1365-2753.2011.01767.x/pdf
A friendly journalist asked me if I had seen the paper from Norway which looked at cholesterol levels heart disease and overall mortality. Amazingly, as I have sensitive antennae for such things, I had not heard of the HUNT 2 study. Not quite so amazingly, no-one else seems to have heard of it either.

The graph on the left looks at overall mortality vs. cholesterol levels. The one on the right looks at ischaemic heart disease and cholesterol levels in both men and women.
As you can see, for women the story is very straightforward indeed. The higher the cholesterol level, the lower the risk of overall mortality. With regard to heart disease alone, the highest risk is at the lowest cholesterol level. For men there is more of a U shaped curve, but overall mortality is highest at the lowest cholesterol level.
This was a ten year study done in Norway, looking at fifty thousand people – with no pre-existing heart disease. So what we have here is five hundred and ten thousand years of observational data.
These findings do not surprise me in the least, for I have seen many other studies demonstrating exactly the same thing. The lower your cholesterol level, the shorter your life expectancy. Just to take one example. An Austrian study twice this size of this Norwegian one came to the following conclusions:
‘In men, across the entire age range, although of borderline significance under the age of 50, and in women from the age of 50 onward only, low cholesterol was significantly associated with all-cause mortality, showing significant associations with death through cancer, liver diseases, and mental diseases.’ http://www.ncbi.nlm.nih.gov/pubmed?term=adam%20%20eve%20cholesterol%20austria
Added together these studies looked at two hundred thousand people, with a total of two million years of observational data which is a pretty damned impressive amount of work and figures.
I am willing to bet that you have heard nothing about either of them. But how could you? The Austrian study passed by the mainstream media without a whisper, as did HUNT 2. The boy tried to shout that the Emperor had no clothes, but the crowd had stuck in ear plugs. For who wants to hear such an annoying message anyway?
I am against over-medicalisation in all its forms. So, apart from being very skeptical about preventative medicine in the area of heart disease, I also worry about other forms of preventative medicine. Breast cancer screening is one area where the balance between benefit and harm may well slip towards harm. Yet, it is presented as an absolute good.
One man who is very critical of breast cancer screening is Professor Peter Gotzsche, who is the clinical director fo the Nordic Cochrane Collaboration Centre, and has written a book called ‘Mammography Screening. Truth, lies and controversy.’ He outlines exactly what has been going on in this are, and makes it very clear that there are significant problems. Primarily with overdiagnosis (there are other problems, but no time for everything in one blog).
Overdiagnosis means finding ‘lumps’ of other suspcious things on mammography ‘lumps’ that would never have caused any problem. How big is this problem. Well, detailed pathological studies done in Australia found that in women who had died of other thngs (not breast cancer) had the following pathologies, any of which could lead to a ‘diagnosis’ of breast cancer if found on a biopsy :
| Hyperplasia | 12.6% |
| Carcinoma in situe | 13% |
| Focal secretory changes | 24.1% |
| Perilobular hemangioma | 11.2% |
| Radial scars (precursor of infiltrating ductal cancer) |
7.7% |
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1977023/?page=1
In other words, a very high percentage of women have ‘cancerous’ lesions in their breasts. Yet, around 4% of women die of breast cancer. In the words of the authors of this study…
‘….in any case, the high frequency of ductal hyperplasia and CIS (carcinoma in situ) 25.6% suggests that only a small proportion of these must ever progress to invasive carcinoma.’
If only a small proportion of ‘cancerous’ lesion actually progress to invasive carcinoma, then the majority of those found would never cause any harm to the woman. Thus overdiagnosis must be a very major problem indeed. Ironically, the more detailed an accurate screening beomces, the more overdiagnosis will occur.
Anyway, I was unsurprised to see the recent headline:
‘Breast cancer screening does ‘more good than harm’ http://www.bbc.co.uk/news/health-19571173
‘Breast cancer screening saves the lives of two women for every one patient who receives unnecessary treatment, according to a major European review. There has been a fierce debate about the use of screening, and policy is being reviewed in England.
The latest study, published in the Journal of Medical Screening, said at least seven lives were saved for every 1,000 women screened. Health charities say the findings will provide further clarity for women. Tens of thousands of women die from breast cancer across Europe each year. The effectiveness of screening programmes across the continent was evaluated in a series of studies.
It concluded that for every 1,000 women screened, between seven and nine lives were saved and four cases were over-diagnosed.. Mammograms spot dangerous tumours, increasing the chances of survival, but also detect lumps that are essentially harmless, exposing some women to undue anxiety and surgery.
Screening doesn’t just save lives today or tomorrow, it saves lives 10-20 years down the line” Prof Stephen Duffy Queen Mary, University of London.’
I know that there is no possible way that anyone can know that for every seven and nine lives ‘saved’ four cases were overdiagnosed. This is scientific nonsense. The reality is that more cases must have been overdiagnosed than future invasive cancers diagnosed.
I have asked someone to forward me the full studies on which this BBC story was based. I have only one part of it so far, and it is a part that worries me greatly, for it makes the following statement.
‘What these papers tell us is that the time has come to move away from relying solely on the older randomized trials of mammographic screening for the evidence-base, and to use data regularly collected and monitored from service screening programmes, with proper statistical analyses in addition to the results from the randomized trials. The authors of these articles set a precedent for how this could be done effectively.’ http://xa.yimg.com/kq/groups/14947167/193204470/name/benefits%20and%20%20harms%20of%20mammograms%202012.pdf
The time has come to move away from relying on randomized trials!
Once you move away from randomized trials you are no longer doing science. You are doing dogma. At which point the truth can never, ever, be obtained. When someone tells me we should use data regularly collected and monitored from service screening programmes with ‘proper’ statistical analysis – I know that THE TRUTH is being buried.
So long science.
