
Epidemiology
If you are going to try and explain what causes cardiovascular disease (CVD) you need to study epidemiology. By which I mean, how many people die of heart disease and strokes in different countries, and communities. Also, what has been happening to CVD death rates over time.
You might think this would be relatively straightforward. If so, please think again. Then keep thinking again until your brain bursts. After that, start again. The reality is that there is almost no fact about CVD epidemiology that I have not seen challenged. Quite rightly challenged in many cases.
You might believe that when someone dies, it is pretty clear what they died of. Again, if you think that, please think again, and keep thinking until your brain bursts. You might further believe that that what is written on death certificates is an accurate record of cause of death… Ho ho.
When I started in medicine, if a patient was old, and developed a cough, then died, they would most likely be recorded as dying of chronic bronchitis. Thus it came to be that, chronic bronchitis was one of the most common causes of death. At least in the UK. Then, one fine day, it was decreed that you could not use Chronic bronchitis as a primary cause of death on a death certificate. And lo, no-one died of chronic bronchitis ever again. A fantastic medical achievement in curing the UK of chronic bronchitis?
Change your definitions, and codes, and you can cure the world of a disease – at the stroke of a pen.
Until 1948, not a single person died of Ischaemic Heart Disease (IHD), (IHD is what most people would call heart disease), anywhere in the world. Then, suddenly, millions were dying of IHD. IHD is a relatively broad diagnostic code, which incorporates myocardial infarction (MI).
What was the cause of this epidemic? Well, in 1948 the WHO decided that disease diagnoses ought to be standardised around the world, so that researchers would have some idea what they were actually looking at. So they created the International Classification of Disease (ICD). Which included IHD. And lo, an epidemic of IHD swept the world. Not, of course, in France, where they use their own diagnostic system – until 1968. A heart attack (MI) was called Cardiac Insufficience (I believe – I may be wrong on this exact terminology).
However, even after 1948, were people really diagnosing CVD/MI in the same way around the world. Were pathologists being accurate, or not. Were doctors simply writing the most likely cause of death on a death certificate, without having the slightest clue what the person actually died of? Who knows – for sure.
One thing I do know for sure is that, before 1948, you can forget looking at epidemiology for any answers, about anything to do with CVD. Now, you can argue this if you want, but I think the data are just too messy to rely on. In truth, you can probably forget anything before about 1960. Do you really think the entire worldwide medical community was suddenly diagnosing everything, in the same way, accurately, all of sudden, from 1948 onwards? If so, you need to go and lie down for a bit.
It was perhaps not until much later that a real effort was made to start ensuring that CVD diagnosis and deaths was actually standardised.:
‘The MONICA (Multinational MONItoring of trends and determinants in CArdiovascular disease) Project was established in the early 1980s in many Centres around the world to monitor trends in cardiovascular diseases, and to relate these to risk factor changes in the population over a ten year period. It was set up to explain the diverse trends in cardiovascular disease mortality which were observed from the 1970s onwards. There were total of 32 MONICA Collaborating Centres in 21 countries. The total population age 25-64 years monitored was ten million men and women. The ten year data collection was completed in the late 1990s, and the main results were published in the following years. The data are still being used for analysis.’ http://www.thl.fi/monica/
Accurate at last? Certainly more accurate.
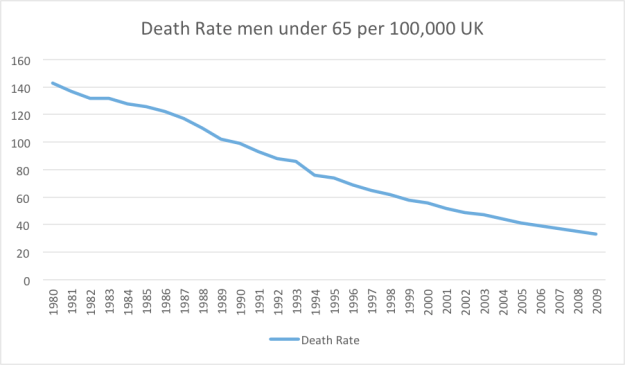
So, what sort of things do these newly accurate figures tell us? Well, looking at the UK, and looking at men under the age of 65, and looking at the death rate from heart disease (IHD), it has been falling and falling, year upon year.
In 1981 the death rate, per 100,000/year was 143. By 2009 (latest figures from MONICA) it was 33.
In case you were wondering, the other graphs: for women under sixty-five, and older men and women, have almost exactly the same shape. I must say, I love graphs like this. I can spend hours trying to work out what these figures mean. I also try to avoid jumping to conclusions (subtle hint to everyone reading this blog).
I also enjoy it when people claim that statins are responsible for the fall in CVD in the UK over the last twenty years. When were statins first introduced? About 1990 (ish). Although, of course, hardly anyone was taking them at first. Not until about the year 2000 did statin prescribing really take off. Look hard at that graph and see if you can see anything dramatic happening. A slight levelling off perhaps?
However, you are not going to learn a great deal just looking at one country. It is far more interesting, and useful, to compare and contrast. If we move from Western to Eastern Europe, the pattern over time is dramatically different. For example, in Lithuania, there is a very differently shaped graph indeed.

As you can see, in Lithuania, the figures are generally much higher, although it is still possible to discern a general downward trend over time. Obviously, however, there was a pretty dramatic blip that started in 1989. What could this be? Let me think? You know what, I think the Berlin wall fell in 1989, as did the entire Soviet Republic.
What then happened in Russia, you may ask. Of course the wall came down in 1989, but Gorbachov managed to remain in power until 1991, keeping things relatively stable within Russia itself. At which point he was overthrown by the rather more mercurial Boris Yeltsin.
As you can see from the graph, in 1992 the rate of death from CHD accelerated rapidly, then it fell, then it went up again in 1999. In 1999 Yeltsin resigned, or was pushed, and appointed Putin as his successor. [At which point, of course, Russia became a peaceful and stable democracy]

In my opinion, the different patterns of social upheaval in Lithuania and Russia, perfectly match the different pattern of deaths from heart disease. I think it would be true to say that Lithuania suffered a sudden, gigantic, social upheaval in 1989. Since then it has become a very different place indeed. Joining the EU, becoming fully democratic etc. In short, things settled down fairly rapidly.
On the other hand, Russia was not immediately affected by the fall of the Berlin wall, at least not to the same extent as Lithuania. It was not until Gorbachev was overthrown by Yeltsin two years later, that all hell broke loose as the social structures totally fragmented. Russia has also gone through many more difficult changes since 1991 with continuing social upheaval, including wars with Chechnya, Georgia and the Ukraine.
Now you can, of course, explain these graphs in different ways. I am sure that people will choose their own favourite interpretation. Mine was, and is, that psychosocial stress/social upheaval is the single most important cause of death from CVD.
In the next instalement I will demonstrate how psychosocial stress links to the processes of endothelial damage and abnormal clot formation.

What a thought provoking series of posts. I have long been a fan of MK’s work (would read/buy anything he writes) but this is quite brilliant. No easy answers at the end, I suspect, but a deal closer to the complicated truth than some vested interests would wish.
You put it so well Dave Nockels. I do hope this is all the basis for the next book…
“Do you really think the entire worldwide medical community was suddenly diagnosing everything, in the same way, accurately, all of sudden, from 1948 onwards? If so, you need to go and lie down for a bit.” Just love your style, Dr K. That’s a phrase I might borrow, if I may, when occasion demands… Brilliant, the whole series. Thank you again for all the work, research, courage and humour.
Death Certificates today just state ” Congestive Heart Failure”. Du … their heart stopped. I view that as being lazy on the part of the Physician or they do not know how to spell a real cause of death. Codes … to many, to get anything straight. My four Sisters died in the last three years … all death cerificates state CHF.
re: Death Certificates today just state…
I suspect what they say varies dramatically depending on whether written by an attending physician or a coroner. Absent an autopsy, CoD may often be little more than a guess. We can’t really compare the data for the two pathways, because autopsy results are overly biased by the presence of foul play.
re: Codes … to many, to get anything straight.
In the institutional setting, the Administration is probably leaning on the staff to code the CoD toward whatever has the most favorable impact on the bottom line, or is the least embarrassing to the enterprise.
There is, however usually little doubt that the deceased is indeed a dead parrot, whatever the cause, and there is usually some confidence in how old the departed was upon departure. This is useful and reliable information.
This circles ’round to all-cause outcome results in trials and studies. The thing that people need to focus on is the “not dying prematurely of anything” part, and not the flimflam “13% relative risk reduction of dying prematurely of isolated ailment XYZ” part.
I wonder if sometimes the pronouncing doctor just takes the easy way out and picks a diagnosis that fits the patient’s history. When my husband died earlier this year, the COD was listed as “massive GI hemorrhage.” Well, yes, he’d had a significant problem earlier in the month that sent him from his nursing home to the hospital. But he’d mostly rallied from that and returned to the nursing home. I was told he passed quietly after eating breakfast. There was no mention of any new bleeding event. Perhaps the earlier bleeding qualified as a COD because it had been only a short time since he returned to the nursing home. I suspect that his actual passing that particular morning had more to do with the amount of morphine he was being given by the hospice team; but that’s a story for another day.
Kathy
This was another “epidemic” that suddenly disappeared off the web sites of the US NHBLI and CDC.
Fact Sheet
National Heart, Lung, and Blood Institute
National Institutes of Health
https://wayback.archive-it.org/3635/20130901052131/http://library.thinkquest.org/27533/facts.html
Data Fact Sheet
http://wayback.archive-it.org/3635/20130901052131/http://library.thinkquest.org/27533/facts.html
Congestive Heart Failure in the United States: A New Epidemic
It is very easy to dispose of “epidemics” when they are embarrassing as in association with statins and cholesterol lowering. One just wonders how many other truths have followed the same line
Disappeared from the websites? Inconvenient finding. And no data since 1993. Make it disappear, like the epidemic of autism.
Yes!
Everything is down to politics….so there we are..after all these months of deliberation, we have discovered the solution to the headline question of this intriguing blog.
So, if politics is to be blamed for poor cardiac health, should we start a political, ( rather than medical), blog, discussing the causes of heart disease?
I have always seen politics as the core of health issues since I started my NHS career in 1965.
Actually, I have mused whether it is the other way around. There are studies that link high PUFA intake with increased aggression in mice and men. We have also seen posted in this very blog comments that statins act in many ways similar to PUFA.
With a significant portion of the population in Western countries nowadays being on statins, antidepressants, PUFA and fructose, maybe this can explain how people are riled more easily and more willing to support demagogues of the worst kind recently?
If course, it comes full circle. If people are angry because they feel short changed by those higher up and powerless to change anything, this will certainly bring on stress, which we are bound to see as an increase in CVD?
Treacherous waters here…
Interesting point. Unfortunately there is too many “conflicts of interests” both in medicine itself and what might be called “medical politics” relating to money and status as an recent editorial in the BMJ has demonstrated. Until these are negated, progress (if any?) will be very slow.
This is all making complete sense.
one of my gt gt grandmothers has written on her death certificate: “Cause of Death: Senile Decay”. I don’t suppose that anyone dies of senile decay any more, so presumably that’s another disease that’s been eradicated, along with pthisis? The heart attack that I suffered three years ago came out of the blue – though rather overweight, I was fit and active with low blood pressure. It occurred following an extremely stressful period in my life and at the time my GP and the coronary care team at the local hospital attributed it to stress. So we all know this stuff, but are brainwashed into pretending that we don’t by obfuscatory pseudo-scientific drivel!
Like your ancestor, my great grandfather died at 96 of alleged ‘senile decay’, according to the death certificate I unearthed. The real cause(s) of death were always known to the family: the elderly live-wire broke his leg after tumbling from the trap he was racing against others through the village where he lived. While subsequently immobilised he developed pneumonia, and died peacefully. The local doctor disapproved of elderly folks gadding about, and insisted GG had died of approved causes. I imagine ‘senile decay’ covered many eventualities!
So is there any reason that suggests itself for the huge decline in CVD deaths in the UK since 1980? From over 140 to 35 or so is a decline of some 75% – obviously significant unless the figures are somehow wrong. I rather doubt it could be due to falling levels of stress, though.
The Lithuanian and Russian graphs do look as if they could be stress-related. And that reminds of a topic you briefly touched on at the end of “The Great Cholesterol Con” – that the French have much less CVD because they have a calmer culture and in particular because they eat meals in a quiet, relaxed atmosphere.
The heroic Dr. K charges on with another great post.
So who escapes psychosocial stress, nor many I would suggest. The poor, painful marriage breakdowns, bereavement/loneliness, so much more. It is quite profound to look at disease this way and I entirely agree with your thoughts about the importance of this on CVD. During the industrial revolution with all its horrors, children working in mills and mines, people did not live long enough to develop CVD and other diseases, they died from the associated diseases of poverty, TB and such. Those in the big house fairing better. We watch our children cope in a fast and furious world, but are they coping. Another fabulous instalment Dr Kendrick.
Dr. Kendrick, I know how easy it is to hare off on these rabbit trails in the search of truth (or at least something that makes sense!), but I remember you commenting a while back that you would be doing a post on prevention. Is that still on the agenda (I hope so)?
If this is in fact true, the heart attack rates in the US will be through the roof in at least part of the last 8 years. It’s my opinion – even when the stress ends (assuming it does) the damage is done and rates will continue to climb for awhile. Self-induced yes, but I’m not sure the US has ever been under more stress than today. The future numbers will speak for themselves.
I thought Iran would have a low CVD death rate because of diet and famine but looks like I was wrong. According to http://www.worldlifeexpectancy.com/top-20-causes-of-death-by-country their death rate by CVD is about 11% higher than the US. A nation that’s starving has to be a good example of very high stress.
Iran starving? Who gave you that idea? This is not what I have been getting from the media (equivalents of the Guardian) and personal reports of travel.
Russia is trending upward since 1992 and Lithuania downward. Opposite trajectories. Your underlying point is undoubtedly true. I wonder what the figures will say for the years following the economic crisis of 2008. We’ll have to wait for that, but I suspect that economic stressors are near the top of the list, and will show up in the CVD rate fairly broadly.
Hi MK —
Once again, another excellent article! And this just mainly concerns those who’ve died.
One of my greater frustrations in learning of CVD “events” is how often they are by doctor’s opinion without being independently confirmed through device measurement. I’ve had at least three doctors I’ve spoken to confirm this, that if a patient complained of acute chest pains that then passed, and nothing was found via EKG, etc., it’s the doctor’s discretion as to whether to rule it a CV event given their profile. So for example, if the doctor knows one has high LDL, it might be considered an undetectable, but passing MI. If low LDL, it might be considered indegestion and they are sent home.
The problem is that this human opinion without independent, objective verification can find its way into studies, just as the death rates you detail above do.
Thanks!
Psychosocial stress is probably the biggest contributing factor to depression. And depression, of course, is associated with heart disease.
Dr. Kendrick: “The reality is that there is almost no fact about CVD epidemiology that I have not seen challenged. Quite rightly challenged in many cases.”
Yes. I read a book by W. E. Stehbens last year call “The Lipid Hypothesis of Atherogenesis” he made a great case that vital statistics from death certificates are unreliable at best. He wrote that Japanese statistics, for instance, can’t be trusted because the cause of many deaths was not certified by a qualified doctor. Also that coronary heart disease wasn’t a desirable cause of death by the Japanese culture. So stroke, thought to be indicative of intelligence, was over-certified and over-represented.. Wink wink! “He dies of stroke, he was a smart guy!”…
So, as you say. Not only should we consider times of great societal stress, but we should probably also consider the cultural biases that have existed in these populations throughout various time periods..
At any rate, when assertions and conclusions are tossed out there based on the historical vital-stats and death certs with no mention of why these “stats” can be massively skewed on way or another – my eyebrows go up.
Thank you!
The “epidemic” in the West could have been due to heart attacks becoming fashionable. It was the era when the hard-charging Type A executive who dropped dead of a heart attack was regarded as a hero instead of a damned fool.
The rise and fall of smoking probably also had something to do with it.
Particularly among the elderly, who is to say what the “real” cause of death was? “Felt lonely and didn’t want to live any more” or “Didn’t want to be a burden” are not appropriate to put on a death certificate.
Among bizarre causes of death was the elderly female relatives of a crusty 80-year-old I worked with who said, “They died of knitting.” He explained they sat hunched over all day in overstuffed armchairs knitting and gossiping and never moved. That’s what killed them.
He himself was very fit and used to growl that depression was simply a lack of physical fitness. Having recently slimmed down and become fitter and feeling happier, I think he had a point.
He died suddenly of an unidentified lung infection. Afterwards, I remembered we’d had a lot of problems with the building’s air conditioning system where we worked. I suspect it was Legionnaire’s Disease.
And at times of social upheaval, with people out of work and not able to access health care so quickly, perhaps causes of death are more briskly and sloppily diagnosed…
Chronic stress (environmental, psycgological…) prevents repair by stem cells, decreases their regenerative potential.
Thank you Dr. K. Such a clear (and funny) account of how epidemiological information can be construed and misconstrued. It’s something I have wondered about in my own search for information about the mortality rates of Idiopathic Pulmonary Fibrosis.
When I was diagnosed with IPF 5 years ago, I scared myself silly reading all the dire, horrific prognostications I came across. Most commonly something like “this devastating disease carries 100% mortality within 2 to 5 years”. When I got to thinking about it, I wondered just how ‘they’ knew that. Was there a central agency which kept statistics? And how would that information be gathered? Was it from doctors’ offices? Were there people assigned to call everyone who had been diagnosed, every six months or so to see if they’d kicked the bucket yet? (Can you imagine that call…oh, Mr. So and So, is that you? Guess you’re still alive, that’s good. I’ll call you next year ). If a person with IPF died of a heart attack, or cancer, or was hit by a bus, was also a smoker, would IPF also be listed as a cause of death on the death certificate? It turns out that no formal statistics were being kept. Just information that filtered in from Drs’ offices. So how on earth can those authoritative statements be made, terrorising those of us unfortunate enough to believe them. As it happens they do not apply to me for one. Five years later I am still doing well, I saw my Respirologist last week for my check up and he was all smiles. No deterioration for four years. I don’t have to see him again for a year. I attribute my continuing health to a strict mostly ketogenic diet. But my Respirologist is not impressed with that, he thinks I’m just lucky!
Maureen,
This is exactly my feelings about the “medical corps”. They love to deliver death sentences and when such a sentence is not executed by a disobedient patients doing “the opposite” it is just a question about pure luck as my own cardiologist phrased it.
Sunds like you are a succesellful part of the strict LCHF-league 🙂
Came across the following Youtube presentation by Dr Wilmhurst. I find it very disquieting particularly when the vast majority of frontline medics are doing there best.
One is left wondering about medical research. Polderman was sacked by the Dutch authorities but the UK GMC seems more likely to cover up false research to protect the establishment.
Of course heart attacks are caused by stress. The only problem is we are unable to medicate the b******ds who cause the stress. Preferably out of existance.
I know to whom I am referring.
“In the next installment I will demonstrate how psychosocial stress links to the processes of endothelial damage and abnormal clot formation” and will also, FINALLY, list those 10 (or more) things that I think everyone should be doing to keep his or her heart as healthy as possible. You know, like I promised to do waaaaaay back in March.
Nota bene: Dr. Kendrick is known to have a great sense of humor, right? 🙂
Eeh, Dr. K., That’s gradely, And fantastic for me to be getting such an education at my age. I’m loving every bit of it. Thank you
Believe me … you gotta start young.
Kathy B, I agree absolutely with you ……but better late than never.
Everyone seems to recognise that stress being a CVD-cause and when “my” cardiologists scratched their heads 1999 looking at the “numbers” and didn’t find “anything” (except low cholesterol) they actually said “It must be the stress!”
And I couldn’t do more than fully agree although my later “research” indicated that the “overconsumption” of PUFA’s and sugar, being a cookie “monster”, may have been the culprit.
What is the definition of stress? The consumption of PUFAs and sugars surely cause as much stress as does psychological stress. I am beginning to think that there will never be any one identifiable cause of any dis-ease. Too many stresses upset homeostasis, and the body struggles to heal itself. It is notable that ancient medical traditions tended to be holistic, treating the person instead of the particular ailment/s.
I know that the more pressure I am under the more I want to eat cookies and other sweets.
Interesting read
My favorite cause of death — found on a 19th-century Lancashire death certificate: “Senile decay.” The man was in his 70s as I remember.
Has anyone looked at those who’ve used the likes of Prozac to ride out personal psychosocial tragedies?
Can such artificial easing of stress be beneficial?
Are we talking here about the downstream effects of stress on our autonomic nervous systems?
Stress> overactive sympathetic response> heart disease. ??
Using psychotropic drugs will likely worsen your morbidity/mortality outcomes, not improve them. Two books to start with: “Anatomy of an Epidemic” and “Deadly Psychiatry and Organized Denial”.
If one would like to engage in a similar thought experiment as the one posed by Dr. Kendrick, take a look at the increase in suicide of teens following the introduction of the black box warning on SSRIs (that subsequently led to a reduction in prescriptions). I’m not a medical provider (I’m a child psychologist), so I don’t really have a horse in this race (outside of keeping children safe). I certainly work with patients (particularly those on the Autism spectrum) who report a reduction in the constant flood of anxious thoughts and feelings. I don’t doubt that this class of medications is overprescribed, but it’s important to consider overall data when considering the balance of risks/rewards.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2799109/#b4-ptj34_7p355
There’s plenty of data that SSRIs actually increase suicides, especially in children and teenagers. If that wasn’t the case FDA wouldn’t have added black boxes. Nor would GSK agree to pay over $2 billion in fines, admit wrongdoing AND agree to start trial registry. A good book on the whole saga is “Side Effects”. A good book on how antidepressants don’t perform better than placebos is “The Emperor’s New Drugs” by Dr. Kirsch.
Not only are these drugs vastly over prescribed, some of the most knowledgeable researchers in the field believe they should not be prescribed at all.
SSRI’s can make platelets more slippery. They have a slight association with increased GI bleeding that seems dose dependent. So perhaps an SSRI might help reduce clotting related to platelets which might have some effect on CVD.
Very good
Dr Kendrick,
Another great post, thank you. I sincerely hope this whole series will form the basis of your next book, the whole series is wonderful.
Re: death certificates. I am told by GP friends, that the cause of death entered on a death certificate will often change depending on which doctor completes the certificate.
For example, if a patient is under treatment for cancer, and perhaps that patient’s body, immune system, CNS and CV systems are all suppressed by disease and treatment, if that patient then suffers an MI and is rushed into hospital and dies in hospital, the physician in the hospital will have to complete the death certificate, likely recording MI as the cause.
But should that patient survive the MI and return home some days later, then die quietly at home the following week, perhaps the family GP will complete the death certificate showing cancer as the cause of death.
Same patient, same medical history, different ending by 1 week, different cause of death recorded.
Does this match your own experience?
Many thanks again, long may your excellent work continue.
It is nice to get onto epidemiology, because just as I think I maybe understand a medical discussion, a someone throws in a whole new set of issues! That 75% reduction over recent years has to be telling us something! I can’t imagine that is just stress – it probably correlates better with the log of the number of transistors in one’s personal gadgets!
I am going to guess at some of Dr K’s recommendations for staving off CVD!
1) Avoid stress as far as is possible.
2) Take a fair amount of exercise (without it itself becoming stressful).
3) Share your house with a pet (my suggestion) and a mate.
4) Have the odd alcoholic drink with your evening meal.
5) Take a 75 mg aspirin, and maybe some omega 3 fish oil.
6) Don’t take a statin – because even if you live longer, you will wish you hadn’t.
7) Try to keep up social contacts.
It also sounds as if Brexit will be a bad idea because it will be an upheaval, but since I have campaigned for it for some time, it will be stressful to me if we don’t achieve it!
I believe he has outlined these factors over the years as have others.
Stop smoking
Get exercise
Eat real food and reduce sugar
Get exercise
Reduce stress
Get vit d out in the sun
Reduce alcohol consumption if it’s high (whatever that is)
I would add roll the dice cos most of us are all in the middle of the distribution so we would only be making marginal differences.
My stress levels are up, as the sky will fall, the moon stop orbiting and pixies will come out of the ground and bite our knees off when we leave on the 23rd.
Uricon:
I’d be very disappointed if Dr. K’s “10 (or more) things to do” came down to just those “things.”
I’m just pulling his leg, anyway, in an (apparently futile) attempt to get him to list them before I croak. I admit that I’m not the most patient person in the world (HPA axis dysfunction?). I love the Kendrick Roman Numeral Series with all my heart, but I’d really like to see that list. I think others would as well.
I kidded him in the past about needing more Roman numerals than Moses needed to write the laws by which Christians and Jews are supposed to live their lives. This long wait is causing me to have a huge problem with that Third Commandment, for example. 🙂
Plus
Take care of your microbiome, eat plenty of cold spuds, cold rice and green bananas. If you can eat them together you deserve to live forever!
What??
It is all about resistant starches! http://www.dietdoctor.com/potato-starch-lchf-resistant-starch
Anna: He’s talking about resistant starch, which is food for our gut bacteria. Potato salad (“cold spuds”) is always tasty, but green bananas? Count me out. As for cold rice, sushi (one of my favorites) would qualify.
re: Take care of your microbiome, eat plenty of cold spuds, cold rice and green bananas.
This cold rice presumably started out as cooked rice (which might as well be sugar). The question is: how much of the simple saccharide repolymerizes to the resistant form? My understanding is: not much, perhaps 15%. A glucometer can arbitrate this. In addition, rice contains wheat germ agglutinin (an adverse lectin), and is at high risk of inorganic arsenic uptake (this is farm-dependent, and “organic” won’t protect you on this). I personally avoid rice in all forms.
Anna said: What??
Whole raw potato and green banana are, metabolically, dramatically different than their cooked potato and ripe banana forms. As raw/green, they provide prebiotic fiber (resistant starch) which is not cleaved to sugar by your enzymes, but instead feeds your gut flora, which use it to produce other important things, chiefly short chain fatty acids. Flour forms of these raw/green starches need further caveats I won’t wander off into.
Getting ample prebiotic fiber has a role in naturally obtaining a more favorable lipid profile (lower TG), reducing BP, lowering blood sugar, improving mood and sleep, as well as gaining significant other benefits not directly related to CVD.
Anna:
I think Uricon is referring to “resistant starches.”
https://authoritynutrition.com/resistant-starch-101/
Bob, WGA attacks glucosamine. Guess what the endothelial lining of blood vessels is made of?
Back to resistant starches:
Still, the Japanese seem to be doing better even if they have plenty of hot and cold rice. Hot rice there is typically overcooked in rice cookers to obtain that mellow, sticky quality. Rice for Sushi is cooked similarly but in addition to being chilled, it also gets soaked in Mirin (vinegar) for a few days. Maybe the cooking and/or the vinegar help in coverting starch?
Bob, this page
https://selfhacked.com/2013/09/30/sourdough-bread-degrades-gluten-and-heals-your-gut/
contains text excerpts and links to various papers that sourdough and even just soaking in acidic water will initiate grain enzymes that break down gluten and potentially WGAs. My hunch about mirin may have been right…
Found it:
Click to access 2010__rizzello__eur_food_res_technol__230_645-54.pdf
Sourdough treatment and baking removes WGA activity even in wheat germ!
@Eric, Thanks for the links on complex bread prep, but my household stopped consuming the seeds of grasses 5 years ago, and we seen no reason to revisit that. My guess is that entirely safe low-carb bread mimics are going to get to market before a safer wheat bread does.
The elaborate processes to reduce WGA, and perhaps deal with the gliadin only address two of a long list of charges on the wheat rap sheet. A new one lately arose, Ochratoxin A (with oats being the leader of that gang). Consuming grains has been a 10,000 year old Faustian Bargain (with considerable CVD risk), and the deal has gotten significantly more adverse since 1960.
On rice, if anyone in the US insists on consuming it, Lundberg Family Farms might be a reliably low-arsenic brand. The simple carbs and WGA they can’t do much about.
Bob, sourdough is the traditional way to make bread, and most organic bread is made this way and quite a few round the corner bakeries still use this method also in this corner of the world. Similarly, sushi rice is soaked in slightly acidic water, which should have the same effect. There is one company in Québec that sells packaged sourdough pasta, but they don’t yet seem to ship to Europe. I found some recipes, though, and will try that.
I suspect that acidic soaking or fermentation by lactic bacteria will also get rid of some other friendly lectins grains may have in store but I doubt they will destroy mycotoxins.
Myself, I find I like bread and pasta way too much to forego them completely, but I now have an explanation why I both like sourdough bread much more and feel more satisfied by it. I try to eat bread only for dinner, and if, rarely, I have pasta or rice for lunch, it will still be confined to a 6 hour window together with dinner, and that works very well for me.
Still, I am ready to read up on the rap sheet. You got a read this first list for me?
Thanks
Eric
@Eric: Still, I am ready to read up on the [wheat] rap sheet. You got a read this first list for me?
Rev 0.9 just completed. “The Wheat Rap Sheet”
https://www.cureality.com/forum/topics.aspx?ID=19033
In the context of the present discussion, for heart health (or any kind of health for that matter), wheat intake needs to be dialed to zero. Ditto for the other gluten-bearing grains, probably rice, and the remainder of the grains need to be considered not-very-complex sugars.
Epidemiology relies, I think, on comparing like-with-like populations over time, to look for variations. It seems to me that this is made particularly hard for CVD-related illness in the context of changing human mobility (as Dr Kendrick has pointed out, tha is frequently associated with times of high stress as well), strong changes in the environment (deprivation, smoking, diet, agrochemicals, etc.) and who knows how many other factors.
Following Dr Kendrick pointing to WHO data (a reply to part xvi) I tried to understand the results for the UK in the context of other results I’d seen, but quickly realised that there are very many ways a population can be divided up and it is far from obvious how to compare these data with those provided by ISDScotland, BHF studies, etc. (At least it goes far beyond the effort I’d be willing to put in.) In particular I noticed varying upper age limits (up to 65 or up to 74 inclusive, for example), and those look very different. The age of death from CVD seems to have moved up, and that raises questions whether it is the same sub population that would have died in their 40s to 60s who are now having CVD related deaths in their 60s+ or some other group.
I looked into a couple of studies connected to my local area, but the results were too complicated and subtle for me to learn much at all. It looks difficult to come up with solid conclusions based on epidemiology.
You forgot about time spent in the sun? And Brexit will still be stressful for you because ‘happy stress’ is still stress…..remember the incidence of heart attacks going up after your football team wins?
Gerry, Heart attacks go down after a football team wins.
The study by Berthier and Bouley in this issue of Heart adds to this small body of growing evidence linking sporting events and cardiovascular events. Their study, again centred around an important football match, this time in France, found a significant decrease in mortality from MI in men on the day France won the 1998 World Cup of football, with a similar but non-significant decrease in women. The resultant euphoria after the victory was heightened by the fact that the game took place in France. The authors hypothesise that the observed phenomenon may have been caused by a decreased level of activities during the day of the game and the “euphoria” of victory. Interestingly, there was also a decrease in mortality from MI in men two days after the game, on 14 July, a national holiday in France. The authors suggest that a day off of work may have been a contributing factor; indeed, the incidence of MI has been shown to be highest on Mondays, possibly from the stress of having to return to work. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1767636/
I wonder what will happen after the coming referendum,
BREXIT
Now that was an interesting event. But I think most will agree that the STRESS is still to come. You aint seen nothing yet.
In years to come researchers will scrutinise the heart disease graphs to conclude the level of stress it caused. This will be fascinating.
Hi Dr K, your clotting disorder hypothesis – it’s amazing how everything falls into line with it.
“In hypercholesterolemia, the high concentration of plasma
cholesterol can cause higher content of erythrocyte plasma
membrane cholesterol. It can result in the deformability of
red blood cells and the worsening of haemorhelogical properties.”
from
Can J Physiol Pharmacol. 2003 May;81(5):485-92.
Effects of simvastatin and pravastatin on peroxidation of erythrocyte plasma membrane lipids in patients with type 2 hypercholesterolemia.
Koter M, Franiak I, Broncel M, Chojnowska-Jezierska J.
http://www.ncbi.nlm.nih.gov/pubmed/12774855
So even whatever association there is between cholesterol and CVD left over from the traditional lipid hypothesis is consistent with your idea!
I had wondered how it could explain atherosclerosis in cholesterol-fed rabbits, but I can see now that it would work well even in that model.
Joe: I’d say that between Dr. Kendrick and the comments there have been at least a couple of dozen preventive measures discussed-for example, an entire post about the importance of sun exposure. Eliminating sugar. Going to church. Food. Avoiding industrial seed oils. Avoiding statins. Not certain if anyone mentioned meditation, but that’s a good one. Being skeptical of whatever conventional medicine wants to do to you. And so forth.
Gary, yes, that’s true. But I’d like to see Dr. K’s list. I’m a big fan of the good doctor, and his opinion really matters to me.
PS: I would opt for castration over taking a statin drug.
If you took a statin you wouldn’t need the castration option. The statin would do it for you.
I’m reading through all comments waiting for the same list.
Gary….couldn’t put it better myself. I was writing my own list, when I came across yours, so I do not need to repeat.
I might have emphasised LCHF under ‘food’, and possibly added “give and receive all forms of love”.
I feel that following this blog for over 2 years has helped me to understand the ‘why’ and the ‘how’ of the need to be personally empowered regarding my own health status.
Knowledge is power.
Jennifer: So right about the blog. This exchange of ideas, and the implementation of some of them, has made a real positive change in both my physical and mental health. Dr. Kendrick is based in Scotland, but he has a multi-continent practice.
Puddleg, good points. But correct me if I’m wrong about the rabbit studies. If I remember well, no matter how much cholesterol they fed the rabbits, they never could precipitate an MI, correct? If so, this would suggest the coagulation cascade was not affected significantly and atherosclerosis was more of a storage disease in rabbits, maybe, rather than due to endothelial damage. Makes me think of the Massai.
Who cares about psychosocial stress that cannot be measured with a couple of simple tests, and then treated with a pill? It’s all in the head!! Now, here’s your number and prescription – and everybody’s happy (except of course us here).
Keep going Dr K 🙂
Interesting research here:
http://www.news-medical.net/news/20160607/Rice-study-takes-deeper-look-at-how-inflammation-bridges-stress-and-diabetes.aspx
linking stress to diabetes
One area that has interested me for a while is heart rate variability (HRV) and the relationship to stress on the one side and heart-attacks on the other.
The heart rate varies in response to many factors, and the most natural state when relaxed shows some randomness, but is largely coherent with a gentle and smooth increase then decrease with a cycle taking around 6 seconds (a bit like the period of waves at the shore).
There are several studies that discuss “heart rate variability heart attack prognosis” (try your favourite search engine). I quite like Tsuji et al. from a subset of Framingham data.
It seems easy to appreciate how stress can damage the balance. I’ve used HRV biofeedback to feel the association of good coherent HRV and a sense of calm, and can use it (or even a memory of it) at times of stress to restore my HRV and calm (they go together), e.g. by thinking of waves on the shore coming in every 6 seconds.
I could easily imagine that poor HRV correlated with those times (like Monday mornings here, oh dear) of poorest outcomes for CVD.
I’m curious how or where this fits into the model.
Ken
Ken,
Me too!
That 6-second cycle in rate variability is called breathing. It’s well known that younger and more athletic people have a greater rate variability in sync with their breathing. Speeds up on inspiration, slows down on expiration. The amount of variability could be considered a rudimentary indicator of fitness level.
So I wouldn’t be at all surprised if it correlated to cardiac mortality. Actually, I’d be surprised if it didn’t.
I am confused: I thought an average adult breathes 15-20 times per minute. Why do you say that 6 second cycle is breathing?
If you can slow your berating to six a minute (actually five point five), this appears to have important effects on vagal tone, resulting in a more coordinated heart rate variability (HRV), calmness and relaxation. This rate, coincidentally or not, is used by many religions around the world. See paper below:
Breathing at a rate of 5.5 breaths per minute with equal inhalation-to-exhalation ratio increases heart rate variability.
Lin IM1, Tai LY2, Fan SY3.
Author information
Abstract
OBJECTIVES:
Prior studies have found that a breathing pattern of 6 or 5.5 breaths per minute (bpm) was associated with greater heart rate variability (HRV) than that of spontaneous breathing rate. However, the effects of combining the breathing rate with the inhalation-to-exhalation ratio (I:E ratio) on HRV indices are inconsistent. This study aimed to examine the differences in HRV indices and subjective feelings of anxiety and relaxation among four different breathing patterns.
METHODS:
Forty-seven healthy college students were recruited for the study, and a Latin square experimental design with a counterbalance in random sequences was applied. Participants were instructed to breathe at two different breathing rates (6 and 5.5 breaths) and two different I:E ratios (5:5 and 4:6). The HRV indices as well as anxiety and relaxation levels were measured at baseline (spontaneous breathing) and for the four different breathing patterns.
RESULTS:
The results revealed that a pattern of 5.5 bpm with an I:E ratio of 5:5 produced a higher NN interval standard deviation and higher low frequency power than the other breathing patterns. Moreover, the four different breathing patterns were associated with significantly increased feeling of relaxation compared with baseline.
CONCLUSION:
The study confirmed that a breathing pattern of 5.5 bpm with an I:E ratio of 5:5 achieved greater HRV than the other breathing patterns. This finding can be applied to HRV biofeedback or breathing training in the future.
P.S. You are right, the normal breathing rate is much higher than six a minute
Thank you Dr Kendrick. Socratic Dog talked about 6 second breathing cycle which works out to be 10 bpm. It picked my interest because that rate correspondents to ancient Chinese acupuncture texts but they don’t mean respiration, even though it often is translated as “breaths”. What you talk about probably has connection with pranayama but pranayama and yogic practices aren’t really religion… I am not aware of other practices that attempt to regulate the breath, maybe you can tell me.
News in the popular press (UK) today of a blood test for IgG factors that can predict chances of a heart attack in the following 5 years. No idea what an IgG factor is, but something to do with a strong immune sysytem? Interesting comments on this including the possibility that those on statins with strong immune systems may be advised to cease taking them…..
I got that this morning as well, the full report doesn’t seem to be on the website as reported. It stands for Immunoglobulin G. Given the onus on inflammation and the idea that statins may no longer be relevant I am surprised this place isn’t awash with comments. IgG is found in bovine colostrum which used to be used as a cure all and still taken by some athletes. Unpasturised milk farms sometimes sell it in the UK. Interestingly IgG is associated with gout through the crystalisation of uric acid process but still some mysteries as to why.
Hi Gerry. Seems rheumatoid factor and coagulation are interlinked: http://www.ncbi.nlm.nih.gov/pubmed/20593110
Immunoglobulin G (IgG): https://en.wikipedia.org/wiki/Immunoglobulin_G
I’m more acquainted with IgM problems, sigh, as in Macroglobulinemia.
How very stimulating I find all comments here!
It makes my head swirl!
When I visited the local mall area here in Gällivare in northern Sweden and I was shocked how theya are pushing the carbs into your brain immediately when entering the”remodelled” grocery department. The indigenous lappish population is today doomed, as most of these kind of populations around the world seem to be, in my eyes and obviously running into the obesity trap at full speed.
I know what you mean, but it occurs to me that if it becomes widely aknowledged that a large percent of a general population cannot thrive on a high carbohydrate diet it leaves us with some major problems – such a diet is cheap in comparison to LCHF (or other varients thereof), and the poorest are already most at risk of obesity and all its ills for this reason. Economic forces also come into play – countries that export grains, those that import them….right down to the local biscuit factory laying off staff as demand falls….this stuff has consequences beyond the odd butter shortages I suspect. We have always had health inequalities I know, but as people become better informed they will understandably become angrier…quite justifiably!
Gerry,
The Sweden LCHF-grassroot movement is in the world in the forefront and there is frequent shortages of butter in our stores. At the same time we hear that the factory bakeries are laying off their employes.
I just wonder when this trend is going to “hit” our health care system. What agony!
I still remember reading Gary Taubes great book “Good Calories & Bad Calories” a few years ago where he describes the situation on the South Pacific very isolated small island Tokelau when the supply boat was wrecked and the island was totally isolated from “western goodies” during half a year.
During that time the two thousand (?) inhabitants had to return to their coconuts and fish and at the same time the “market” for the local small health care centre dwindled and an obvious closure of that unit was close by.
But a safe health care market returned as soon as a new supply boat appeared.
Market forces are brutal and don’t care the least about our health if no money can be made.
Being in northern Sweden i am just studying how the market forces during more than a thousand of years during the last 100 of years today are much more efficient in ruining the health of the indigenous population. It might be that they during thousands of years to some extent have been adopted to the mainly meat based subsistence on reindeers and therefore especially sensitive to the temptations on the carb market.
Still we met two youngsters who entered into the top cabin yesterday where we were dwelling in front of the heater (bad cold weather again!) and who where halfway on their 22 km mountain tour and needed to get reheated. And both declared that they were LCHF-adherants. Encouraging that it is not only the very metabolically trapped people like me and my wife who understand what it is “all about” and what has to be done.
There is hope 🙂
Göran, about a week ago, in the other thread, you stated that you could not tolerate sweets and beer and had to stick to wine and whiskey. I was curious about your reasoning why wine and whiskey would be ok but not beer. Ethanol is metabolized much as fructose, so not heart healthyily. Beer may have a few extra carbs thrown in, but they are not fructose, plus its alcohol content is much lower. Much as I prefer wine over beer, I don’t see why it would be a healthier choice.
Eric,
It is an interesting subject you bring up about beer, wine and liquor.
I think the key word is “moderation” and as you mention fructose and alcohol metabolise in about the same way in the liver. In excess you will get the fatty liver and die early.
A few years ago I plunged into this subject and arrived at a university specialising on the subject where it was claimed that there was basically no difference between beer, wine and liquor regarding longevity – it was all about the alcohol consumed in moderation being “optimal”. Probably it is a question of the relaxation effect – boosting the parasympathetic nervous system.
Still we have the well known “beer-belly” syndrome and here I suspect the excess carbs involved.
There is evidently also residual agricultural poisons like glyphosate in beer that comes along with the heavy spraying of the crops which may attack the gut flora and cause metabolic havoc if we should trust Dr. Stephanie Seneff at MIT among others. Dr. David Perlmutter brings this up in his recent book “Brain Maker”. It is probably not by coincidence that the ubiquitous glyphosate is now very closed to get banned in Europe.
Perhaps a rather smokey whisky is the best choice or organic red wine which I presently enjoy together with the grilled deer heart.
Göran, found this.
http://www.dietdoctor.com/low-carb/alcohol
The problem is: they don’t count ethanol as a carb (which it is). They seem to count fructose, though, even if much of the prose blabs about glycemic response. Ethanol and fructose generate no glycemic response but they are metabolized as VLDLs.
Dr. Göran: Still we have the well known “beer-belly” syndrome and here I suspect the excess carbs involved.
Suspect also the grain proteins. Barley, rye and wheat, the principal ale/beer/lager ingredients after water, are all gluten-bearing. Standard brews are essentially liquid bread. A growing number of gluten-free beers have appeared on the US market, but only a fraction of them are also low carb, as they typically just switch to other grains. Those which are both GF and LC seem relatively harmless.
re: I think the key word is “moderation” and as you mention fructose and alcohol metabolise in about the same way in the liver. In excess you will get the fatty liver and die early.
One or two 120ml (4 US fl.oz.) glasses of a dry organic wine per day might be optimal, and this prescription has the support of at least one cardiologist here.
Too much stressing here over what and how much to drink. Much less stressful to just drink, and enjoy it. The reduction in stress level will make up for any potential harm.
I’ve observed before, this blog does bring out the hypochondriacs.
Well if chronic stress is a cause I suspect women the world over would be keeling over like ninepins. They aren’t.
I think Dr Kendrick may have mentioned (forgive me if I’m wrong, its been a long series of posts!) that the coping mechanisms for stress may differ between genders, resulting in a delay in onset of heart problems? Women are generally presumed to have better social networks than men for example, whereas increasing rates of suicide in men has been linked to the combination of economic stressers combined with social isolation? Just a thought.
They can multi stress!
Hmm, your comment seems to assume that women lead more stressful lives than men the world over. I certainly doubt that, but I have been predicting that in countries like the U.S. where I do think women are under abnormal stress that they are not metabolically designed to handle, there is going to be an increase in women’s health problems and a lower their age at death.
Hi Malcolm,
Re: your latest on epidemiology, I think the term that was used back then was Coronary Insufficiency.
Very best wishes,
David
Ta. I was trying to be posh and French
This is slightly off topic for part XVII but directly relevant to the previous. An item on the radio this am:
http://www.abc.net.au/radionational/programs/breakfast/researchers-identify-genetic-link-to-the-onset/7528354
Dear Mr Kendrick You are one of the few honest doctors around, it is so good to hear a doctor who cares about giving patients the right Information. Could I ask what you know about toxic poisoning on the endocrine and nervous system and cell tissues?
Sent from my iPhone
>
I’m curious: what if you compare data for Israel and Switzerland for the same period?
Currently they have approximately the same population (number), and yet surely have a dramatically different history and psychosocial stress pattern over the same period. Perhaps too they’re both outliers, at opposite tails of the distribution. And they both have modern Western healthcare systems with presumably comparable record keeping practices.
Can anyone help with this?
Patrick
I wonder if it is even necessary for HFLC to be more expensive. I’ve heard for years that there are a lot of subsidies for big ag, including cheap oil. But the way people live may soon change as more people are becoming interested in growing some of their own food. Keeping kitchen gardens and hens in the back yard could become more common again. Perhaps if corn were not so heavily subsidized, it wouldn’t make economic sense to take vast numbers of cattle and pen them up and feed them corn. I’ve got some neighbors out here in the country who raise up a pig or two and a steer or two and then have them butchered. Grass fed and sunshine. The creek is in the pasture, the grass grows for free…
You see these ridiculous stats on how many gallons of water it takes to produce a pound of beef. It’s over by at least one order of magnitude, and who cares anyway if the water falls from the sky? But places that don’t have water and pasture ought to have low populations and not be in the beef business.
Meanwhile, growing food is a very arduous task, and therefore must in some sense be expensive. Since I started gardening 3 years ago, I can attest to that. Mostly labor. Allocated land. Some hand watering necessary when plants are seedlings. But with cheap oil we can raise food, both meat and plants, which are dollar-cheap but look at the reality: 10 calories of energy, mostly oil, for every calorie of food. Think about that. It’s a suicidal path. It can only continue until it can’t anymore. Our dependency on oil is another whole topic, but it is a stupid and ruinous use of the resource. It is all about greed which now rules the world, not health. And along with that desire to have one huge megafarm raise a vast quantity of plants is the requirement for poison pesticides and top soil abuse and loss.
I’m no longer interested in propagandistic comparisons of real food with unsustainably raised food. Come back in a few hundred years and see how food is raised. Probably much sooner.
(It was a rant, but I think a comprehensible one.)
Anna,
HFLC or as we say in Sweden LCHF tells that you first reduce the carbs and then replace them with healthy fats rather than with excess protein. In my eyes it is a completely “new” way of living in our modern society and therefore very provoking to most healthy people I guess. Conflicts easily develop within your own family (I know!) where people tend to “defend” their sweet carbs at all cost.
What we initially found when “converting” 7 years ago is that the LCHF living was about 10 % more expensive. When you leave all processed food behind and make your own meals from scratch you are saving a lot of money. And we are frequenting restaurants much less today. I haven’t done any recent estimates but I think you are right that it is about the same price tag although a tremendous quality difference from a nutritional and health point of view.
Besides getting generally interested in nutritious food you may arrive at organic grass fed beef but especially the organ meat which people are shunning today although it is the best food you can eat. Market forces let you then buy the best food you can get for about one third of the price you pay for the lean muscle meat which the indians traditionally reserved for their dogs.
The cost for the two deer hearts I acquired here in northern Sweden, and still devouring, was about one quarter of what I would have paid for the “best” beef but with its questionable fat composition. Wild game is optimal. Though you have to add butter since it is often very lean.
Today my wife, honouring her Lappish roots, will make sausages from reindeer blood where you must add a lot of animal fat. And the sausages you eat with butter only. All this is ridiculously cheap if you don’t count the time you put into the preparation.
Dr. Göran Sjöberg
“Today my wife, honouring her Lappish roots”
Interesting. Sami people surely had a deep knowledge of (medicinal) mushrooms. Do you also pick and eat some?
Anna: Well said. The Great Central Valley of California, where I live, is all grassland, quite brittle in the south, less so in the north, but suitable only for raising grazing animals. So what are they doing? “Investors” are plowing up the grass to plant almonds (very thirsty crop) for export to China, while we’re in our fifth year of drought.
Sorry OT: Aren’t the water drawing rights in California grandfathered so that it would be difficult to obtain water for new plantations?
Eric: California water rights are somewhat complex, and they apply only to surface water. Basically, those who have a pre-1914 right get first dibs on available water, and whatever is left over (sometimes none at all) is allocated to those with a post-1914 right; there are also riparian rights, but these only apply to farmland adjacent to flowing streams and rivers which have been in continuous production. Part of the problem with this system is that the allocations (like those for Colorado River water) were made during especially rainy decades (prior to 1940). But the bulk of new almond plantings use water pumped from the aquifer, and this is almost entirely unregulated. The high price that almonds command and the fact that they have few pest problems makes the expense of pumping tolerable for the investor. However, draining of the aquifer is causing serious sinking of land, and may cause the California Aqueduct to require very costly repair.
I seem to recall reading that water left over from fracking is now being used for agricultural irrigation in California. Puts me of the idea of buying their almonds!
Ezetimibe, or Zetia. What is this stuff?
I told my doc that I’ve been off my prescription of atorvastatin for a couple of months now and will not be going back. (I was sick, or so I thought, all Winter. Quitting atorvastatin was the complete cure.) He took it in stride, but recommended that I consider Zetia.
He claims the stuff lowers cholesterol AND that it therefore reduces CVD.
Sounds suspect to me.
What’s your take?
JD
Ezetimibe is supposed to take cholesterol out of your gut. As far as I know, was approved on basis that it lowered cholesterol. But it doesn’t make you live longer. IMHO avoid
Statins – increase the risk of hemorrhagic strokes, or bleeding into the brain.. Anybody else notice since lipitor went off patent more of these knocks are coming out. http://www.scientificamerican.com/article/do-statins-produce-neurological-effects/
Dr. Kendrick, Have you heard about 116 year old Emma Morano?
https://en.wikipedia.org/wiki/Emma_Morano
Sorry for joking, but she’s been living in two millenia and three centuries.
I gather from the reports that this woman has been living a very calm life. It’s as if she chose at one point to stop worrying. They report that she eats raw eggs every day, since a doctor recommended that because an anemia she had when she was 20. No other doctor ever told her to “stop the treatment”, so she kept on.
Obviously, not worrying would not stop a firing squad or a famine or a virus. But if you manage to survive to political disasters and pandemias, perhaps calmness as a life attitude will prevent diseases such as CVD. (Add some eggs, just in case.)
According to the Wikipedia article, she eats three eggs a day, possibly all of them rare (which I would not recommend for supermarket eggs).
Fred Kummerow also said in an interview that he has a boiled egg with milk for breakfast every day.
Onto something?
You might think this would be relatively straightforward. If so, please think again
Having been involved in epidemiology since 1956, I am entirely in agreement with this statement. At that time (pre-easy access computers) in the veterinary field risk was called “challenge” and medical “risk” was involved in infections, mostly of vector borne diseases such as malaria. Even in this type of disease which compared to CVD is relatively simple, it is still very complex as I have learnt to my cost. Things go well until the appearance of some totally unexpected factor; in my case it was the appearance of a predator fly that attacked and ate the vector snail of the liver fluke and lead to the end of a beautiful system of calculating of risk. Such is epidemiology!
With respect to CVD it seems to me that apart from age and stress the next major factor may be nutrition, a subject that is sadly neglected in medical education which is largely directed at the use of pharmaceutical drugs.
However, in this series of articles, Dr Kendrick has introduced the concept of nutritional and physiological factors into the system (epidemiological) leading to CVD for which I wholeheartedly congratulate him. Indeed I repeat my request that he publishes these articles in a book. While I doubt that it covers the panoply of factors involved, I think that he has probably teased out some of the major factors involved.
Nutrition is at the top of the list. I have had two episodes with the heart two years ago. I use food /natural base vitamins with my food every day. On my last Dr visit and after a Echo Cardio he said ” In two years, you have come along way, most people take five years to get as healthy as you are today, keep up the walking and strength training.
Kathy,
Nutrition is certainly a major factor. At present, through changes in nutrition and supplements (again following Dr Kendrick’s observations) I am struggling to stabilize my BP. Even at much reduced dose rates, my SBP at “supine” rest approaches 90 and is often in the 100s. Suggestion by my GP (a Kendrick fan) that L-arginine along with Vit D, C, etc may be the cause but pointed out that “n” = 1. On the other hand, like adverse reactions, for sufferers it 100% though in the herd it can be very rare.
are you saying that that that L-arginine along with Vit D are causing your high blood pressure?
Bravo. Cause and effect has to be the goal and Dr. Kendrick seems to be getting close.
In regard to mine, your health status … right on !!! Knowledge is Power.
To J D … You feel great … stay off the statins, you will live a healthy life with out them. Statins are prescribed to enhance the bottom line of everyone except the person taken the pill. They know the RISKs … Good Luck in your choice.
Dr. Kendrick’
As you have listed ACE inhibitors as positive action against heart disease, I recalled reading a doctor’s column some years ago with a comment on them. I’ve located the research reference and thought your readers might be interested in the contents. I have been on ACE inhibitors for more than 20 years and I have never been advised either by my GP or pharmacist that they should be taken at night. Hope the link works.
http://www.medicalnewstoday.com/articles/224989.php
Hanna
Hanna
You may be interested in this NHBLI report (no Big Pharma involvement apparently)
http://jama.ama-assn.org/cgi/content/full/288/23/2981
JAMA. 2002;288(23):2981-2997 (doi:10.1001/jama.288.23.2981)
ALLHAT Research Group
Chlorthalidone better than Calcium channel blockers(amlodipine) and ACE inhibitors (lisinopril) and doxazosin (early termination of the doxazosin (doxazosin mesylate, a quinazoline compound) arm of the trial
On checking my records I see that I have done an expert report for this drug on its pre-clinical data. Clinical medical reports I cannot do as I am a Vet (the only species outside my remit)
Amlodipine
Chlorthalidone triggers a constant sympathetic response. Not good.
Chlorthalidone Messes with your insulin. Not good.
The fix? Spironolactone added on. Look up the side effects of that. Feminization. Gynecomastia. You don’t want that even if you’re a woman.
http://hyper.ahajournals.org/content/60/2/319.long
Hanna,
Two points:
1. There is a fairly common phenomenon called “escape” wherein the enzyme that’s inhibited from changing angiotensin I to active angiotensin II is replaced in its function by alternative bodily enzymes. In other words, after several years, the stuff no longer works. Happened to me after a dozen years on lisinopril. Now I’m on the ARB valsartan and wondering if the same thing might be happening.
I get Dr office systolic pressures of 160 to 190. I’m told that momentary spikes like this while under STRESS don’t matter — but I wonder.
Anyone?
2. I was taking my ARB at bedtime like a good boy, but I would get this nasty surge on waking – middle-of-night or morning – going suddenly from very low pressure to operating pressure.
Don’t most MIs happen in the morning? Don’t I want to avoid daytime spikes? So, I started splitting pills. Half with breakfast, half with dinner. Better. Not best.
I would suggest getting a home BP monitor and testing your own BP. You will find there is some considerable natural variation – something you never get to see when you get it taken in the surgery. The stress of going to the surgery and expecting bad news from the BP test may be enough to disturb the measurement – reminds you of Quantum Mechanics, doesn’t it!
Chrono-Biology! Now one has to wonder what happens to patients that have to get up in the middle of the night, with naturally somewhat lower blood pressure at that time, and the ACE-inhibitors kick in fully. That might not be a lot of fun.
I myself had a close encounter with a bath tub edge due to low blood pressure (was severely sick & dehydrated at that time – partially my fault). I was quite surprised when I woke up in the tub. No permanent damage was done. A frail person might have cracked his or hear head open or worse. Falls in elderly & frail people can be quite terminal.
With regard to the effects of ACE-inhibitors, I find the following paper rather interesting! Guess what, Vitamin D3 again. Get some sunshine! Combine that with a decent low-carb diet, which is naturally diuretic (via low insulin & Sodium shedding in the kidneys), and much could be improved naturally. The right food & sunshine!
“Vitamin D 3 Therapy Corrects the Tissue Sensitivity to Angiotensin II Akin to the Action of a Converting Enzyme Inhibitor in Obese Hypertensives: An Interventional Study”, J Clin Endocrinol Metab. 2012 Jul; 97(7): 2456–2465.
http://press.endocrine.org/doi/pdf/10.1210/jc.2012-1156 [open access]
Robert
Thank you for the reference. Interesting but 14 is a very small sample. Not my idea of reliable.
Pat
Well, if the mechanism is sound & biology agrees, I don’t think we need 100 years of RCTs.
Just like with parachutes 🙂
Robert – interesting link. Thank you. Needs more work with a larger sample – “Fourteen of the remaining 17 subjects ” is somewhat small.
Hi Robert, that’s a good idea if you’re taking ACE inhibitors for blood pressure. Another thing that helped me is reducing my insulin resistance, through a combination of intermittent fasting (IF) and LCHF. Now, I also have lost 50 pounds, so I can’t say it’s due solely to IR reduction, as too many variables are moving at once. However, I lost about 20 pounds on LC and did not change my blood pressure. I then added in IF and HF, and my blood pressure plummeted. Unfortunately (or fortunately, depending on how you look at it ;-), my weight also decreased another 30 pounds. Again, too many factors are moving at once.
However, I take an ACE inhibitor for idiopathic dilated cardiomyopathy, not high blood pressure. My blood pressure when I was diagnosed was about 120/80 and my blood pressure now is about 105/65 (I also take a beta blocker). I have almost three years of data to prove this.
I asked the cardiologist whether the body gets used to either of these drugs, and he said no. However, I no longer believe anyone, after reading about statins and nutrition. Everything the “experts” say is wrong, so I have a difficult time believing my cardiologist. I have not, however, had the time to research all the studies on my condition. I do know insulin resistance is implicated in it, which is one reason I researched how to decrease my insulin resistance.
@Pat M:
Here’s another one, showing a mechanism how D3 deficiency increases blood pressure (in mice). Once renin and everything downstream is directly affected, I start to “believe” in a real effect.
“Vitamin D Deficiency Induces High Blood Pressure and Accelerates Atherosclerosis in Mice”
http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0054625 [open access]
Now, I don’t know if the atherosclerosis aspect in this paper can be applied 1:1 from mouse to human (e.g. different diet), but I guess blood pressure regulation is a common feature in mammalian physiology.
how much vd3 do you need to reduce blood pressure
The only answer to that can be, surely, how much vitamin D can you get from sunshine. I don’t think you can get much over 25,000iu per day because the UV radiation also breaks it down, and people who get that much sun exposure aren’t as healthy as people who get a bit less; I reckon about 10,000iu is a reasonable exposure (also, if you were adapted to very high exposure, you’d have darker skin, so get less). And the sun doesn’t shine every day.
So my estimate, which I use, is to take 10,000iu if the sun hasn’t shone for a while, then cut back to 5,000iu, which is the average I’d like to be getting from the sun if it shone every day.
YMMV, but this is working for me at keeping my psoriasis at bay this winter, which is the only test I have to judge the effect of vitamin D3.
@Mal
I do not know! I’m not a medic 🙂
Some guidelines ( http://press.endocrine.org/doi/10.1210/jc.2011-0385 – open access ) say “take 800 IU/d” as a maintenance dose. In elderly people with absorption problems (or lactating women), this might be pushed up to 2000 IU/d from what I’ve read. If you’re truly deficient, you may be prescribed 10.000 IU/d or more. In one of the previous papers I posted, the patients took 10.000 IU/d I think. Please verify it yourself.
However, as far as I understand, this is to prevent D3 deficiency symptoms, which is not necessarily a “normal” or even optimal level for it. If my memory serves me correctly, 15-20 minutes full body exposure to mid-day sun can synthesize quite a lot of D3 in the skin. Don’t quote me on this, I think I’ve read somewhere that in summer you need 6 minutes for 1000 IU or thereabouts (no sunscreen, no shirt on). So one could argue that nobody dies from D3 poisoning by walking naked for 6 minutes in the sun, some people do a lot more! Taking the equivalent by food / supplement sounds sensible to me, if there is insufficient sun exposure or deficiency.
Now, what is a good D3 level in the blood, not just a sufficient one? Some people argue that you should have blood levels like someone living near the equator. I don’t know what these numbers are.
According to this paper from 2010 ( https://www.ncbi.nlm.nih.gov/pubmed/20352622 ), one should shoot for 100 nmol/L (40ng/ml) of D3 (based on Canadian data). People with much sun exposure (like life-guards or “traditionally living populations”) can be higher: “The mean serum 25(OH)D concentrations of Maasai and Hadzabe were 119 (range 58–167) and 109 (range 71–171) nmol/l, respectively.”
http://journals.cambridge.org/action/displayAbstract?fromPage=online&aid=8735073&fileId=S0007114511007161 – open access
What dosage is required to go there? The following paper ( http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0111265 – open access ) – Figure 1 – shows a relationship between daily D3 intake and blood levels in healthy test subjects. It might give you a hint at how much you might need. Probably somewhere between 1000 and 5000 IU/d, unless you’re severely deficient.
So… have a chat with your GP, have some blood taken & start your science project. Alternatively, get out in the sun regularly & see if your BP goes down after a few weeks of doing that.
For Science !
@puddleg58
Any insights on whether K2 is required / optional at those high dosages of D3? You get some with dairy, but if one were to limit that for weight loss…?!? Of course the argument about D3 vs.sunshine still holds, yet a supplement may prove to be not quite the same.
robert: Vitamins A, D, and K2 work synergistically. Chris Masterjohn has written much about this. Worth a read.
You’re not going to get K2 from sunlight, so it’s not intimately connected with the benefits of vit D3; it’s good to have but the trials of K2 for CVD don’t seem to have produced anything.
I’m going to put out an idea here – LDL is the delivery system for fat soluble vitamins, and it’s been shown that requirement for vit E to get it into vascular endothelial cells is increased by hyperlipidemia. Simply, the fat soluble vitamins are diluted if blood lipids are high, and maybe it takes a little more then to keep blood vessels healthy. Which is not a problem if your lipids are high because you’re eating the fatty foods that supply these vitamins, but may be if lipids are high because of high sugar, refined fat diet.
Maybe.
Hanna, it’s too bad that study was done on mice. It would’ve been nice to have a follow up study on humans.
In terms of the list for staving off CVD perhaps we can add to it “read Dr K’s Blog” as the humour in his writing certainly lowers my stress levels and often raises an audible chuckle. Great stuff.
🙂 he he I agree
Here’s a thought experiment, but I don’t know what the outcome would be. Any comments?
There are two twins, Fatty and Poofa. They are genetically identical and eat a healthy diet with plenty of unsaturated fat. Their Total Cholesterol count is identical. Then Poofa reads that saturated fat is dangerous and replaces it in his diet with PUFAs. His diet is otherwise identical to Fatty’s. Same calories, same protein, same veggies etc etc.
What will happen to Poofa’s TC count?
1. His TC will go down, because as every conventional doctor knows, replacing saturated fats with PUFAs lowers your cholesterol count. That’s why they recommend “heart-healthy” seed oils and margarine.
2. His TC will go up, because as Dr. Cate Shanahan points out, some of his LDL will be oxidised because of the PUFAs. The body does not recognise this oxidised LDL, therefore his liver will produce more cholesterol to compensate until it reaches the correct level (i.e. the same as Fatty’s). His TC count will be increased over Fatty’s by the amount of oxidised LDL circulating in his blood.
(I’m assuming that TC is measured by centrifuging blood and measuring the amount of oily/fatty liquid that separates out.)
re: Here’s a thought experiment, but I don’t know what the outcome would be.
You might find answers in the various papers linked from:
https://wiki.xtronics.com/index.php/Health_effects_of_different_fatty_acids
(not my site – that’s by a user on a forum I frequent)
Information on fatty acids cobbled together by a bunch of electronic engineers — I don’t think the answers lie there. Anyway, the point of the thought experiment is to highlight that two authoritative statements lead to conflicting outcomes. Which authority do we trust?
@Martin: Information on fatty acids cobbled together by a bunch of electronic engineers…
That’s just one engineer (Karl), as I understand the situation, and one who was failed by consensus medicine over a decade ago, and has been doing independent investigation ever since (a story much like Ivor Cummins, The Fat Emperor, and also an engineer).
re: — I don’t think the answers lie there.
It’s pretty clear to me, just based on results, that the majority of CVD relief can be had from a grain-free very-low-net-carb, high specific (and low-inflammatory) fat, moderate protein diet that is attentive to common micronutrient deficiencies including ω3 DHA&EPA, Vitamin D, iodine (and underdiagnosed hypothyroid generally), Mg and perhaps some others.
If a population does that, but a few still have lingering CVD issues, where do we look next?
There are a number of candidates. I’m keeping a list, and ω6LA (linoleic acid) is on it. The consumption trend of ω6LA-heavy industrial grain and seed oils is a perfect correlate to some contemporary chronic non-infectious diseases. Unlike some other correlates (aluminum being an example), I’m inclined to weight ω6LA away from coincidence and toward contributory.
Karl contends that the half life of ω6LA is 600 days in the body. If true, this makes it very difficult to run studies, much less trials. He’s running an N=1 low ω6LA experiment. I avoid the stuff, but probably not as ruthlessly as he does.
«Which authority do we trust?»
The one in the mirror, primarily. If consensus medicine is mistaken (and they are, on multiple ailments), are you more likely to learn about from insiders or outsiders?
Other than convenience, there’s rarely any downside to avoiding novel (post 19th century) ingredients in diet.
On reading Peter Attia’s blog post, it seems the LDL particles do not get oxidised while floating in the blood. It is only after they have burrowed into the arterial wall that they get oxidised, therefore they would not appear in a blood test and cannot increase the TC score.
Can LDLs themselves get oxidized or is it cholesterol particles that get oxidized?
My understanding (of this murky area) is that LDLs are oxidised in the artery wall. This is part of the process whereby macrophages attack foreign material with NO (thus oxidizing said particles) before ingesting them. Thus oxidized LDL particles represent parts of the healing process (which can go wrong/be overwhelmed). Others call this healing process ‘inflammation’ and thus further confirms their view that inflammation is the underlying cause of plaque development.
Thank you. I wonder why drugs that significantly lower LDL have such minute effects on CV events? Is it because by then atherosclerosis is so far advanced that lowering LDL hardly makes a difference?
Dr K,
This presents me the opportunity to again ask: Ought we to consider INCREASING inflammation when it occurs rather than decreasing it? Encourage those various cytokines to get along and do their job?
Possibly. I would worry about interfering with the body’s natural healing processes
“I wonder why drugs that significantly lower LDL have such minute effects on CV events?”
Possible explanation: The body obviously needs LDL, otherwise it wouldn’t be making it. The coronary arteries, being closest to the heart, will get first dibs on any LDL going, so be relatively unaffected by any lowering of LDL levels. Then the other arteries will take their share, and finally the capillary-fed tissues will have to make do with what is left. It is the extremities, such as the hands, feet, brain, and skin, that will be starved of LDL and show the effects, if any.
Interesting, thank you. I wonder what others on here think of this proposed patho mechanism.
The first place to get dibs on LDL would be the portal vein. The liver does not make LDL, it makes VLDL (very low density lipoprotein). As VLDL loses fat/triglyceride it shrinks down to become LDL – after several passes round the body. Just about the last place to get any LDL would be the coronary arteries. Although the level of LDL remains pretty much constant day in, day out. Same in arteries as veins.
Thank you!
“For every problem, there is a solution that is simple, elegant, and wrong.” — H. L. Mencken
Drat! I thought I had it all figured out. *sad face*
I’m sort of with Joe. This is all fascinating, but hard to do anything about.
Not that a simple list of dos and donts would necessarily be easy to follow, and I have multiple issues, none of which are CVD, currently, so maybe it doesn’t really matter to my quest to eek out another decade or so.
When our great midsummer festivities now having arrived in Sweden I wonder if the very smokey type of whisky (Ardbeg 10 years) is the best medicine choice. Smoke tend to keep the mosquitos away, well known among the lapps for millennia, and with these small creatures on the increase today in northern Sweden I will try my best to keep them away from the inside this way. In a store I though saw an ingenious devise with a price tag of 1000++ USD (11 000 Swedish Krona) which promised to keep them away from the outside.
But I am an ultimate sceptic so I will try the safe smokey internal way instead. I will get 20 bottles of Ardbeg ten years for the same amount of money and that will for sure take away any worry about the mosquitoes. Although I have just got one bottle which I probably will have to share with friends anyway. That is the way it goes 🙂
Goran,
Whisky academy last night tasting Jura whiskies. Jura whisky is said to prolong life, one man saw 180 christmases.
Why do you go for Atdberg, the most peaty of whiskies?
I believe there is at least one Swedish whisky, do you know where?
Chris
There are numerous whiskies around the world including Swedish. I have not tested all. Moderation! And we need to honour Malcolm so I tend to go for the Scottish ones.
Highland Park is my favorite
Is it wicked to say I love the American bourbons, don’t know if they are classed as true whiskies. Can be persuaded to have an Irish or a Scottish.
Dr. Sjoberg:
You want smoke? Try Lagavulin 16. It won’t help with the mosquitos, but you won’t care.
Bob:
I think it all matters. Many health issues are interrelated. CVD and diabetes, for example. There are exceptions, of course, but what’s good for one issue is usually good for others.
I hope you get your decade, Bob, plus a few more.
A double whammy – cardiovascular disease and cancer – Vit K. Lots of studies. Key take away – keeping the walls of the blood vessels supple. http://www.ergo-log.com/you-ll-live-longer-if-your-diet-contains-lots-of-vitamin-k.html http://www.ncbi.nlm.nih.gov/gene/2677
Dr. Kendrick:
Have you seen this and can you give us your
take on it? Atherosclerosis by Valadimir Suppotin: http://static1.squarespace.com/static/52faa95ee4b0b0a74811f732/t/576ed362b8a79bc10875b866/1466880934734/2016+Vladimir+Subbotin+Paper+-+ATHERO+.pdf
I have seen it. It is very interesting, I am attempting to think it through
The new Subbotin paper and the recent Peter Attia post directly disagree with each other on endothelial thickness and lipoprotein entry vector. Readers of the blog (including Ivor Cummins) have asked Peter about this, and he has responded. Here’s one:
http://eatingacademy.com/cholesterol-2/heart-disease-begin-tell-us-prevention#comment-1039900
Both appear to agree that consensus dogma is crackpot, consensus therapy largely useless, and that matters are already well out of hand by the time conventional tests detect anything.
Why should the opinion of someone called Attia matter? Did he even read Subbotin’s paper?
@Diana: Why should the opinion of someone called Attia matter?
Because he, like Drs Kendrick and Subbotin, is a prominent dissident voice on the topic of lipidology and heart disease (and also quite an authority on ketogenic diet and athletic performance). Attia is also crediting Thomas Dayspring for much of the theory.
re: Did he even read Subbotin’s paper?
It appears so, and I frankly wonder if he wrote his blog article on CVD etiology as a response to it.
What we have here are two respected investigators disagreeing on a key aspect of CVD. Part of that dispute (endothelial thickness) might be straightforward to resolve, and depending on how resolved, might then make the need for a vascularisation theory vanish. This appears to be an honest scientific debate, and one quite germane to Dr. K’s series here.
Bob Niland
I’m sorry but my standards are somewhat higher when using expressions like “prominent voice” and “respected investigator”. It seems Dr. Attia was repeatedly asked by commenters what he thinks of Dr. Subbotin’s paper, and the only answers he managed was this (shortened):
“Do you believe the endothelium is only one layer thick:”
PA: Yes.
and
“Have you seen this recent description of the mechanics of atherosclerosis? It’s quite different from the version you describe. What do you make of it?”
PA: “Yes I have seen this and don’t find it as compelling as this model.”
and
“Have you read Vladimir Subbotin’s latest paper? It seems all is not well with the orthodox view of atherosclerosis development (including the leaky ‘single-cell’ endothelium…) Vladimir certainly takes a pathologist’s view of the phenomenon…and then some ”
PA: “Yes, familiar with his work. I don’t agree, obviously, but not quick response so this will have to wait.”
Attia reveres Dayspring.. and maybe rightly so. I’ve followed and learned from Dayspring, myself. Learned MUCH from his lecturepad website and have watched and listened to many of his lectures and interviews over the years.
You never know what’s in a man’s heart, so maybe this is unfair.. But I feel as if Dayspring’s been nuancing and tweaking his view of heart disease (how it progresses and what the so-called “risk markers” of the disease are and what therapeutic targets need to take priority) on the fly to allow him to continue to recommend statin-therapy.. Indeed, he makes the case (quite slyly?? -maybe unfair to use that word) that a huge chunk of the population has been overlooked for statin-therapy… I get the feeling that he’s tying himself in a pretzel knot trying to figure out how he can continue to recommend statins..
/shrug.. just one man’s opinion.
repsort: I have no scientific or medical training or expertise, other than what I’ve learned here and elsewhere, but I have to say that I find the Subbotin paper compelling. Initially he says: “Facts showed: (i) normal tunica intima invariably consists of multiple cellular layers; and (ii) initial lipid deposition occurred in the deepest layers of the tunica intima.” In the paper he provides photographic evidence for both claims, shows how the tunica intima grows in size from infancy to adulthood, and that the tunica intima forms a thicker layer than the tunica media in adulthood. He says the fatty streaks (initial lipid deposition) are apparent in children by age ten. Whence their origin? If from arterial blood, how and why do they migrate through several layers of cells to be deposited so far below the endothelium? It seems to me that “invariably consists of multiple cellular layers” compels a revision or modification of our understanding of atherosclerosis, at least in regard to the endothelium. Is it a normal process of aging? Is it always pathological? Or, what makes it pathological? Kind of makes your head spin.
@Diana, regarding Dr. Attia’s terse replies, I think we will need to wait for further remarks by both gents. Note that although Dr. Subbotin included “…and constitutes a therapeutic target…” in his paper title, we didn’t get any real detail on that: “Although this review suggested that … is … a potential therapeutic target, the analysis intends only to outline practical implementation of this suggestion.”
It may be some time before CVD theory is settled. In the meantime, practicing physicians (such as Attia) need to apply what is found to work, paying close attention to markers that correlate with outcomes, and of course, eventual outcomes. What is working is not Standard of Care. Of these two authors, I think I’d prefer Attia for a personal consultation, but I’m very interested in what Subbotin has to say (as well as what insights Dr. Kendrick might have on the Great Endothelial Debate of 2016).
“regarding Dr. Attia’s terse replies, I think we will need to wait for further remarks by both gents. ”
Good luck waiting!
Very well presented.
” this review suggested that the uncontrollable cell proliferation in coronary tunica intima, followed by neovascularization, is the initiation of coronary atherosclerosis and a potential therapeutic target,”
I love Dr. Subbotin’s references to very old papers, and Clause Bernard. Worth reading.
“Therefore, one should anticipate that, after this publication in 2002, all studies on coronary atherosclerosis would be grounded on well-documented facts of coronary artery morphology (…) but, as my readers have probably already guessed, this is not the case.” LOL
It seems that he is not finished: “In the future we will analyze coronary pathologies that are completely unrelated to coronary atherosclerosis yet bear the same initiation hallmark – cell proliferation in the coronary tunica intima.”
Indeed. Subbotin is a true “man of science” and cares deeply about finding truth, no matter where that might take him.
I fell in love with his work a while back and have had extensive, friendly, email discussions with him over the years. Much of his work is self-funded.. Had he asked more “conventional” questions that sought to reinforce the consensus theory there is little doubt that a mountain of money would have been accessible to him to fund his research..
When asked why he does it, he replied:
“Because it is the meaning of my life…”
I respect him very much.
Does this mean he is correct? That’ll be for smarter men than me to debate.. Men of science who are unafraid of where the truth will take them.
Men like Dr. K 🙂
Wow.
I guess you mean CLAUDE Bernard, the 1900-th century physiologist!
He is on of my favourites when talking science in medicine.
Sure, it was a typo. Claude -> Clause. My apologies.
bill: That’s a very interesting paper. Like you, I’m hoping Dr. Kendrick will give his analysis of its implications for heart disease.
Mike Cawdery, thanks for the link. I ploughed through some of it but had to take an extra pill and go lie down. A bit too technical for me but got the gist. I replaced my thiazide with L-taurine as my potassium dropped too low. Finding the right combinations is a bit hit and miss too. I suspect a lot of hypertension is caused by anxiety and white coat syndrome.
Like many here, I have returned to using butter rather than margerine, and use olive oil for frying so as to avoid PUFA’s, while reducing my intake of sugar fairly substantially.
I have noticed that the osteoarthritis in my knee (patella) has nearly vanished, and I wonder if this welcome change could be attributed to my change in diet.
David Bailey: The Wulzen factor, found in butter, is anti-arthritic.
Hah! Yet another biochemical I had never heard of before!
This really adds to the absurdity of the decision to demonise butter, because arthritis can obviously reduce the quality of life (mine was fairly minor), and it can also reduce the amount of exercise that people take – which will impact on their health.
If it is the Wulzen factor, I would say it is quite powerful.
David Bailey: The full name is “Wulzen anti-stiffness factor,” called so because it was discovered by Rosalind Wulzen, a UC physiologist. It is a plant sterol called stigmasterol, found primarily in plant fats, but obviously the rumen of a cow somehow makes it from grass. Some say that pasteurization destroys it, but according to Mark Sisson, there is no real evidence that it does. I did have some arthritis problems in my forties and fifties, particularly when I ran more than 20-25 miles a week. But they vanished when I started eating piles of butter (each month about 2/3kg, along with 2 liters cream, which is little more than emulsified butter). All raw and pastured. I think drinking a cup of bone broth each day (with butter and sea salt) helps, too. Zero joint problems, and good mobility, with the workout I do.
Gary,
Thanks, I looked it up as well.
I guess my point was that so often one is told that this or that food is good for you, that I normally ignore such advice – particularly after learning about the ‘evidence’ against saturated fats.
However, when the effect is seemingly so pronounced (and I only use it as a replacement for margarine, so I eat far less than you do) it is extraordinary that this has been neglected. I mean even if saturated fat really had been bad, this compound could still have been extracted (it is a quite different kind of chemical), and would have made a huge difference to many people’s lives.
Stigmasterol is a “plant sterol” but it is actually produced by endophytic fungi (shown also for many other phytosterols).
China is stealing our almonds?
Their prices have risen to outrageous levels indeed. I always blamed it on the Californean drought.
On the topic of CVD. I shall apologize for not having posted this earlier. Topic (Migraine) belongs in the previous thread really, but who reads stale comment threads?
Dr. Strunz from Germany reported more than once that adaequate (which means for the rest of us, really high) levels of magnesium seemed to help with migraine.
Now I am lucky never to have had any migraine attacks, and unlucky not to be able to afford Dr. Strunz, so this is not even anecdotical evidence. Dr. Strunz is also known to be pretty optimistic about his orthomolecular therapies.
Still it would seem to me that one could ponder the ad-hoc hypothesis that a lot of Mg prevents migraines (somewhat). Mg and K are known to counteract Na CVD effects. Those lucky enough to have enough Mg would, then, perhaps suffer less migraine and less CVD/HT problems, which would then show up as a migraine – CVD association.
Wheels within wheels. I will just chew some Mg before sleep every night.
This program about the microbiome is interesting, and also blows away the conventional saturated fat theory:
http://www.bbc.co.uk/programmes/b07ff0hl
If you download it before listening, you can skip the rather trivial start if wish.
Gut Microbiome:
Please read Brain Maker by Dr David Perlmutter. up to date and fascinating. Also recommended by Goran – thanks Goran for the recommendation, really enjoying this book.
Dt. Graveline (spacedoc.com) in a recent newsletter has raised the issue of genes and incidence of adverse reaction citing the following:
PHARMACOGENETICS OF SLCO1B1: POPULATION GENETICS AND EFFECT ON STATINS
Marja Pasanen ACADEMIC DISSERTATION Helsinki 2008
available as
ISBN 978-952-92-4677-9 (paperback)
ISBN 978-952-10-5090-9 (PDF, https://helda.helsinki.fi/handle/10138/22995)
This thesis was available in 2008 – 8 years ago but unnoticed (??? or ignored???) by the so-called experts. I leave you to judge.
Dr Kendrick – just in case you hadn’t spotted this: http://eatingacademy.com/cholesterol-2/heart-disease-begin-tell-us-prevention
I have just read Dr. Attia’s post also – a very worthwhile read for us all. You will recognize much in common with what Dr. K wrote, what has been discussed here, and also with what Dr. Cate Shanahan said about oxidized fatty acids. All very interesting, and if it is true, then we all already have fatty streaks in our arteries.
Attia, “The endothelium is a protective one cell layer lining the surface of the artery lumen. ”
Wrong. And if we’re to understand this disease and answer the question, “What causes heart disease?” we must understand the organ’s normal morphology..
http://www.sciencedirect.com/science/article/pii/S1359644616301921
repsort: The Subbotin paper renders the Attia post concerning the development of atherosclerosis fundamentally wrong. Interesting that he calls the latter the “consensus view.” I wasn’t aware that consensus had positive value in science, but he is probably correct in using this terminology. Subbotin tells us that the infiltration and deposition of lipids in the artery wall begins deep in the tunica media, brought there by new vasculature which develops as the artery wall thickens and requires a blood supply to provide oxygen to its tissues, rather than from arterial blood via the endothelium. Hoping Dr. Kendrick can sort this out. I can’t see any middle ground here, or perhaps both processes are in operation? Subbotin’s paper has a powerful evidentiary base.
Didn’t Dr Kendrick endorse the latter view (from arterial blood via the endothelium)?
It’s over. The debate is settled. It’s sugar, not fat, that causes heart attacks. http://www.huffingtonpost.com/dr-mark-hyman/sugar-heart-attack_b_4746440.html
Debates never end when there is money involved. Science is unimportant. Truth was never the issue. The desire for money is everything. And there is not a better swindle than one that has the stamp of approval of some authority.
In my tiny experience the cause of death written on the death certificate has almost no relationship to what killed them 😦
On a different note : your graphs illustrate Smoking/Vodka kills!
Are there any stats with which to compile graphs of “debilitation rate”, i.e. the rate at which people become permanently debilitated?
Here’s my theory.
In the normal course of events, LDL passes through the endothelial layer and carries cholesterol and other lipids to the artery walls where they are used in the cell maintenance which is always going on.
However, if there happens to be a local concentration of some Factor X in the bloodstream, possibly glucose or insulin, which gets carried into the artery wall with the LDL, the LDL becomes oxidised and does not get safely disposed in the normal way. Instead, it builds up into fatty streaks which eventually develop into full-blown arteriosclerosis.
As the blood passes on through the capillaries, the Factor X gets used up in maintaining the other tissues in the body, so by the time the blood reaches the veins there is not enough Factor X remaining to affect the LDL in the walls of the veins, thus there are no fatty streaks found in the veins.
Hemodial Int. 2016 Jun 29. doi: 10.1111/hdi.12439. [Epub ahead of print]
Effect of vitamin D supplementation on endothelial dysfunction in hemodialysis patients.
Karakas Y1, Sahin G2, Urfali FE3, Bal C4, Degirmenci NA3, Sirmagul B5.
Abstract
Introduction Patients with chronic kidney disease (CKD) commonly experience 25-hydroxyvitamin D3 (25-OH-D3) deficiency, and these patients have a higher incidence of cardiovascular diseases (CVDs) due to endothelial dysfunction (ED). The aim of our study was to investigate the effect of 25-OH-D3 deficiency and its supplementation on ED in patients with CKD. Methods Twenty-nine uremic patients on dialysis and 20 healthy controls were evaluated for ED by high-resolution Doppler ultrasonography of the brachial artery. In addition, 25-OH-D3-deficient patients (25-OH-D3 < 30 nmol/L) with CKD and healthy controls were evaluated for ED before and after 8 weeks of oral vitamin D (cholecalciferol, 50,000 units) treatment. All subjects were evaluated for percent flow-mediated dilatation (%FMD), percent endothelium-independent nitroglycerin-induced vasodilatation (%NID), and bilateral carotid intima-media thickness (CIMT). Findings Patients on dialysis had lower %FMD and %NID 6.11 [2.27-12.74] and 10.96 [5.43-16.4], respectively, than controls 15.84 [8.19-22.49] and 21.74 [12.49-29.4], respectively (P < 0.05). Patients on dialysis had higher left and right CIMT (0.79 ± 0.15 and 0.78 ± 0.14, respectively) than controls (0.60 ± 0.09 and 0.59 ± 0.09, respectively; P < 0.05). In 25-OH-D3-deficient patients with CKD, after vitamin D treatment, %FMD was significantly increased in dialysis patients (10.25 [7.8-12.8]) compared to before supplementation (5.4 [2.77-6.15]; P < 0.001). Discussion These results indicated that dialysis patients had significantly lower blood 25-OH-D3 levels and higher CIMT than healthy subjects. In addition, vitamin D supplementation improved ED and increased %FMD in dialysis patients. Our findings suggest that vitamin D supplementation in dialysis patients might prevent CVD.
© 2016 International Society for Hemodialysis.
Vitamin D deficiency accelerates progression of atherosclerosis in pigs – new study
http://atvb.ahajournals.org/content/early/2016/06/02/ATVBAHA.116.307586.abstract
Exogenous KPNA4 rescued 1,25-dihydroxyvitamin D–dependent suppression of NF-κB nuclear translocation and activation. Vitamin D deficiency caused extensive CAD progression and advanced atherosclerotic plaques, which are linked to increased KPNA4 and nuclear NF-κB levels in the EAT.
Conclusions—1,25-dihydroxyvitamin D attenuates NF-κB activation by targeting KPNA4. Vitamin D deficiency accelerates CAD progression at least, in part, through enhanced chronic inflammation of EAT by upregulation of KPNA4, which enhances NF-κB activation. These novel findings provide mechanistic evidence that vitamin D supplementation could be beneficial for the prevention and treatment of CAD.
I dont think ldl itself is fatty, it is just the transporter but its cargo is fatty. To me it looks like yet another suggestion that excess linoleic acid is a main suspect, it behaves ‘wrongly’ and the resulting mess cannot be cleared away.
Highland Park,
Lagavulin,
Laphroaig (My favorite!),
Etc:
“”We know that even healthy elderly individuals have an elevated basal inflammatory state, known as ‘inflamm-aging.’ Advanced age alone is a risk factor for a poor prognosis after injury or infection. Adding alcohol to the fragile immune milieu of the aged reduces their ability to fight infections,” Dr Curtis added.”
Actually, they’re talking about elderly sloshed mouse individuals.
The questions are: Does this research reliably extrapolate to you and me?
Are their ideas about inflammation sound?
Which commenters are on-the-money?
Am I being a “hypochondriac” by even posting this?
http://www.medscape.com/viewarticle/865526?nlid=107427_2981&src=wnl_dne_160630_mscpedit&uac=25547DG&impID=1142771&faf=1
This comment from the medscape link (above) makes me see red:
“t does not help to have a daily “happy hour” in retirement homes, which Dr Kovacs said may not be that uncommon. In such settings, groups of older people with compromised immune systems may be at higher risk for community-acquired infections.”
By the time you get to be in a retirement home, I would have thought you should do whatever makes you happy – then of all times, you should not be worrying about your long term health!
I agree, David Bailey. I once read about the development of a liquid statin for people who were too old and infirm to swallow pills/tablets. My thought was “WHY???”
Me and my hubby are enjoying life in our own private retirement home…..him with his Laphroaig, and me with any old scotch to hand ( because I drown it with cream and honey). Within reason, we see little point in denying ourselves any pleasures we fancy, as we enter the autumn of our lives. We have worked and provided to the best of our humble abilities, and at last, we are turning our backs on the ‘experts’, who have advised us to follow a rediculously dangerous diet, prescribed inappropriate quantities of toxins for non-existent conditions, and pulled the political wool over our eyes for their own selfish goals.
Give me a top-up pet….and pour yourself another!
Patients with chronic kidney disease (CKD) commonly experience 25-hydroxyvitamin D3 (25-OH-D3) deficiency, and these patients have a higher incidence of cardiovascular diseases (CVDs) due to endothelial dysfunction (ED). The aim of our study was to investigate the effect of 25-OH-D3 deficiency and its supplementation on ED in patients with CKD. Methods Twenty-nine uremic patients on dialysis and 20 healthy controls were evaluated for ED by high-resolution Doppler ultrasonography of the brachial artery. In addition, 25-OH-D3-deficient patients (25-OH-D3 < 30 nmol/L) with CKD and healthy controls were evaluated for ED before and after 8 weeks of oral vitamin D (cholecalciferol, 50,000 units) treatment. All subjects were evaluated for percent flow-mediated dilatation (%FMD), percent endothelium-independent nitroglycerin-induced vasodilatation (%NID), and bilateral carotid intima-media thickness (CIMT). Findings Patients on dialysis had lower %FMD and %NID 6.11 [2.27-12.74] and 10.96 [5.43-16.4], respectively, than controls 15.84 [8.19-22.49] and 21.74 [12.49-29.4], respectively (P < 0.05). Patients on dialysis had higher left and right CIMT (0.79 ± 0.15 and 0.78 ± 0.14, respectively) than controls (0.60 ± 0.09 and 0.59 ± 0.09, respectively; P < 0.05). In 25-OH-D3-deficient patients with CKD, after vitamin D treatment, %FMD was significantly increased in dialysis patients (10.25 [7.8-12.8]) compared to before supplementation (5.4 [2.77-6.15]; P < 0.001). Discussion These results indicated that dialysis patients had significantly lower blood 25-OH-D3 levels and higher CIMT than healthy subjects. In addition, vitamin D supplementation improved ED and increased %FMD in dialysis patients. Our findings suggest that vitamin D supplementation in dialysis patients might prevent CVD.
© 2016 International Society for Hemodialysis.
Hemodial Int. 2016 Jun 29. doi: 10.1111/hdi.12439. [Epub ahead of print]
Effect of vitamin D supplementation on endothelial dysfunction in hemodialysis patients.
Karakas Y1, Sahin G2, Urfali FE3, Bal C4, Degirmenci NA3, Sirmagul B5.
Abstract
Introduction Patients with chronic kidney disease (CKD) commonly experience 25-hydroxyvitamin D3 (25-OH-D3) deficiency, and these patients have a higher incidence of cardiovascular diseases (CVDs) due to endothelial dysfunction (ED). The aim of our study was to investigate the effect of 25-OH-D3 deficiency and its supplementation on ED in patients with CKD. Methods Twenty-nine uremic patients on dialysis and 20 healthy controls were evaluated for ED by high-resolution Doppler ultrasonography of the brachial artery. In addition, 25-OH-D3-deficient patients (25-OH-D3 < 30 nmol/L) with CKD and healthy controls were evaluated for ED before and after 8 weeks of oral vitamin D (cholecalciferol, 50,000 units) treatment. All subjects were evaluated for percent flow-mediated dilatation (%FMD), percent endothelium-independent nitroglycerin-induced vasodilatation (%NID), and bilateral carotid intima-media thickness (CIMT). Findings Patients on dialysis had lower %FMD and %NID 6.11 [2.27-12.74] and 10.96 [5.43-16.4], respectively, than controls 15.84 [8.19-22.49] and 21.74 [12.49-29.4], respectively (P < 0.05). Patients on dialysis had higher left and right CIMT (0.79 ± 0.15 and 0.78 ± 0.14, respectively) than controls (0.60 ± 0.09 and 0.59 ± 0.09, respectively; P < 0.05). In 25-OH-D3-deficient patients with CKD, after vitamin D treatment, %FMD was significantly increased in dialysis patients (10.25 [7.8-12.8]) compared to before supplementation (5.4 [2.77-6.15]; P < 0.001). Discussion These results indicated that dialysis patients had significantly lower blood 25-OH-D3 levels and higher CIMT than healthy subjects. In addition, vitamin D supplementation improved ED and increased %FMD in dialysis patients. Our findings suggest that vitamin D supplementation in dialysis patients might prevent CVD.
© 2016 International Society for Hemodialysis.
It is so easy to get overwhelmed by all detailed information and misinformation in the millions of the medical “scientific” papers and by necessity you have to be very selective about what to read. Unfortunately we all carry a bias and which a sceptical mind might call a preference for “cherry picking”. I note with one of my favourite philosopher Schopenhauer that we must carry such a bias by definition. How would we otherwise be able to orient ourselves in the “real world”?
As many here on Dr. Kendrick’s blog who comments I am fed up with the corruption of medicine as well as with the agriculture corrupting our food. As one may imagine this is not about some misbehaving individuals but about the actual “system”. But how does the system work and is it possible to change?
Having recently read the book “The Truth About Drug Companies: How They Deceive Us and What To Do About It”, of the former long tome chief editor of the “New England Journal of Medicine” Marcia Angell, does not encourage me to try to disentangle the medical literature web further.
Instead I try to get a more comprehensible overview of the “driving forces” behind all this corruption and again it is easy to get overwhelmed by what is available. Just now I am reading a capturing book with the appropriate title “Swimming With Sharks” by the Dutch journalist Joris Luyendijk.
This is kind of a scary reading about how our financial system “behaves” behind all this corruption and how the individuals involved are just trapped in a “greedy” system rather than being themselves rogues. My present thought it is that it is here the major shift has to take place before something fundamentally can be changed in medicine.
We have met the enemy and the enemy is us.
regarding Randall’s linked article above about sugar in the diet causing heart disease, I am finding the article confusing and nonspecific. He and his research seems to be targeting “added sugar” which I take to mean actual white stuff. But this:
“Most of us don’t know that a serving of tomato sauce has more sugar than a serving of Oreo cookies, or that fruit yogurt has more sugar than a Coke, or that most breakfast cereals — even those made with whole grain — are 75 percent sugar. That’s not breakfast, it’s dessert!”
Seems a bit unlikely and I am now wondering if he means carbs and sugar together? Or what breakfast cereal is he talking about specifically. I do not believe that tomato sauce has more sugar than cookies. I bake and I know how much sugar is in cookies, especially that white icing in the middle is mostly pure sugar. It is hard to make anything at 75% sugar. I have been canning up some jam, and I use the low sugar recipe, which comes out less than 50% sugar and this is a very sweet food. Tomato sauce can not possibly have more sugar than a cookie with icing. I am not even disputing the basic premise of the article, with which I agree.
@Anna, regarding Randall’s linked article above about sugar in the diet causing heart disease,
Your reply got disconnected, but that’s presumably in regard to the 2014 Mark Hyman blog post.
re: I am finding the article confusing and nonspecific.
I agree. It’s not clear if the focus is added sugar, native sugar, or just carbohydrates that act like sugar (“…that sugar — and flour, which raises blood sugar even more than table sugar…”) is his only hint that a substantial fraction of the diet can act just like sugar.
On tomato products, tomato sauce has some natural sugar (about 5% by weight, if nothing else is added). This theoretically make it impossible to sell “sugar free” products with any significant amount of tomato content, but that doesn’t stop marketeers from doing so.
Far too many canned and bottled products based on tomato also have added sugars. In the US, the Nutrition Facts panel and Ingredients list are useful aids. One “organic” tomato sauce I just looked at (Kirkland), has added “organic granulated sugar”. Ketchup is usually a glycemic disaster, and all but one or two “no sugar added” ketchups rely on troubling artificial sweeteners.
Sugar itself is too vague a term. The major simple sugars are glucose, fructose or some combination (sucrose, or just a blend as in HFCS). These have separate (but comparably damaging) metabolic effects. Only glucose raises BG promptly. Diabetics are often fooled by “low GI” sugars that are heavy in fructose – won’t spike BG, but their insulin resistance, triglycerides and excess belly fat aren’t going to improve.
In the context of the present series here, those desiring to reduce their CVD risk, by reducing sugar exposure, need to focus on all carbs that are sugars, are rapidly cleaved to sugars by human enzymes, or, due to present dysbiosis, are converted to sugars (rather than SCFAs) by unfavorable gut flora.
With apologies for the colonial units of measure, the metrics for managing this, with some suggested goals, might be:
☤ HbA1c no higher than 5.0%,
☤ triglycerides no higher than 60 mg/dL,
☤ fasting BG no higher than 90 mg/dL, and
☤ postprandial BG peak no higher than 100, but ideally unchanged from FBG.
Yes, these are quite aggressive compared to targets you’d get from a National Diabetes Promotion & Maintenance Association or Statin Advocacy Society.
I am curious how it is physiologically possible to have postprandial BG unchanged from FBG.
Eat fat & protein, e.g. bacon & eggs.
In my case my after-food glucose levels are actually a few points lower than fasting, but I don’t follow a normal diet. My pancreas is more or less “asleep” & only squirts out some insulin when I eat food via the mouth. I guess my phase-1 insulin response is basically gone, as I usually don’t need it (keto diet). All my pancreas makes is “basal” insulin & for some reason I run a bit high fasting (about 100), probably some degree of muscle insulin resistance, as I don’t exercise enough.
Robert: eat just those things? In regards to keeping pancreas asleep. I would be interested in why you figure we evolved to have pancreas and to produce insulin? Sorry, to ask but I am trying to understand the rationale behind some of these diets. Thanks
The pancreas is part of a regulator ‘circuit’, insulin is the negative feedback in the control loop. It is necessary. The question is how much do we want to disturb the equilibrium (fasting state, covered by basal insulin levels, normally quite low) & which disturbances were more common during the time we were “made”.
Very low BG levels are lethal quite rapidly, there are more than one mechanisms to raise them quickly (adrenaline, glucagon…). The normal & healthy body is well protected against lows. On the other hand, the only thing that I know off that rapidly lowers BG is insulin.
One could argue that it has been evolutionarily beneficial to protect more against low than high BG numbers, presumably because persistently high BG via diet has never been an issue in distant ancestors (before onset of agriculture). It would have been a waste of resources to develop & keep an overpowered pancreas, just in case that at some point later in time people might overeat sugar and grains. Evolution doesn’t work like that.
Aggressive lowering of blood sugar in diabetes increases mortality. I would just add that, in diabetes, there are many more players than insulin and blood sugar levels.
In the context of a conventional high carb diet, for sure. Eat whatever you like & just compensate with shots. Make an error with carb counting or insulin (injection site variability…) & you’re either in the 500s or in a hypo coma – BG roller coaster.
The law of small numbers holds. If neither carb intake nor injected fast-acting insulin are high enough to disturb BG significantly, you get a flat line, low HbA1c, and avoid diabetic complications. Of course this means eating very low carb.
ACCORD study? I’m sure you know this paper.
http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(14)60611-5/fulltext
Robert, fasting insulin levels and FBG levels aren’t equilibrium, they are a marker of fasting. Equilibrium doesn’t lead to death while fasting long enough will.
Also, persistently high BG wasn’t an issue not just for hunter gatherers but for most people long after advent of agriculture (unless they were wealthy – a minority). Whichever country you’re in, look back 80 years or so and you will see that you ancestors from that point and back to beginning of time didn’t have high BG levels. Nor is it a problem for many people today – 1/3 of human population are either mal- or undernourished.
@Sasha, re: “I am curious how it is physiologically possible to have postprandial BG unchanged from FBG.”
A very low net carb meal (15 grams or less net carb), high in fat and non-starchy vegetables, and moderate protein, suffices. Attention to microbiome, a number of common micronutrient deficiencies, and having optimized (not to be confused with “normal”) thyroid function helps as well. Several named LCHF diet/lifestyle programs in the US accomplish this.
Anyone not aware of the glycation issue might want to consider this insight on HbA1c from Ireland: http://www.thefatemperor.com/blog/2015/3/21/blood-glucose-and-heart-disease-great-hba1c-associational-study-lchf2015
Dr. Richard K. Bernstein (“The Diabetes Solution”) thinks the HbA1c target needs to be 4.7% max. I doubt that’s possible if the daily BG excursions are allowed to get much over 100 mg/dL.
Bob: these dietary recommendations go against all observational data we have on some of the longest living populations on Earth. What are they based on?
Sasha, your longest-lived communities (with benefits of clean air and plenty of sunlight exposure and so many other confouders) don’t have much CHD, obesity, diabetes, etc
Maybe if they did, their diet would be disastrous for them, maybe not.
Our populations have a high risk of existing disease; we need recommendations that reverse these conditions or maintain health in their presence.
puddleg58, you’re putting the cart before the horse. The reason these populations don’t have diabetes, CVD, etc is because they don’t eat Big Ag food. It’s not that they don’t have those diseases and therefore can afford to eat their traditional diets which are often high in carbs.
The solution is simple: move away from processed foods, cook for yourself, buy clean, organic, local ingredients, and move. Stay away from extreme diets, be they LCHF or vegan. In my opinion…
Au contraire Sasha, my point is the for many the cart is already well ahead of the horse, and the methods for preventing an epidemic may not be the same as the methods for treating it, though they will have much in common.
Organic foods, pastured eggs, and so on are counsels of perfection, and if we can’t prosper without them then the majority are doomed.
More particularly, not everyone everywhere is descended from people who ate wholesome high starch diets. Where I live part of the population are descended from Pacific people who never saw cereal foods at all till a century or two ago and never saw a wholegrain until they visited a commune in the 1970s, and most of the rest of us are descended from Northern European peoples who only had carb dense foods in any quantity in the late mediaeval period, when potatoes, oats, barley, and wheat replaced the turnip, acorn and chestnut.
All this “sugar is evil” and “keep blood glucose down” as much as possible talk sounds like obscession, really. And it has no mirror image in ancestral communities.
Metabolic Responses to Oral Glucose in the Kalahari Bushmen (Joffe, 1971)
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1799259/
The plasma glucose, immunoreactive insulin, and growth hormone levels after a 50-g oral glucose load have been measured in 15 adult Bushmen subjects living in the Kalahari region of Southern Africa. Compared with 10 non-obese white controls, they showed relative glucose intolerance and significantly impaired insulin secretion. Growth hormone responses showed no significant differences between the two groups. Factors such as inadequate or unusual nutrition and stress do not appear to account completely for the abnormalities in carbohydrate metabolism observed in the Bushmen. Of interest are the clinical and hormonal similarities that seem to exist between the Bushmen and the Central African Pygmies.
Diana, I couldn’t agree more. I would say: stay away from processed foods and sugar but do eat sweet potatoes, good quality grains, etc.
All traditional cultures ate those foods, otherwise evolution wouldn’t give us a pancreas.
Do bushmen in their natural habitat eat grains, wonder bread and drink soda? I doubt it. Cereal with skim milk and sugar for breakfast every single day? Nope. Natural honey, maybe, but not whole year round.
Glucose intolerance, either pathological (T2 diabetes) or physiological (glucose sparing while on low carb diet) is not harmful as long as you don’t repeatedly bombard your system with “supra-physiological” / “industrial doses” (Dr. Richard K. Bernstein) of carbohydrates, jacking up BG and especially insulin levels far beyond normal. A state of emergency for the body.
Dear Robert,
I don’t eat many grains, wonder soda etc, nor am I a bushman.
Are your comparisons relevant?
@MrChris
I was replying to a post by ‘Diana’, in which she referenced a paper titled “Metabolic Responses to Oral Glucose in the Kalahari Bushmen”.
Anna, Bob, Sasha, Robert,
When my wife and I recently have been feasting on the “old time” true Lappish fare like a soup on the fattest parts of the reindeer only or on charcoal grilled wild captured fish eaten with butter we have reached those low BG-values also postprandial with e.g. 4.3 and 5.1 measured yesterday for me and my wife respectively. Thus it seems possible even for severely metabolically trapped people to “escape”. Moderate exercise seems here to add benefits as well.
Reading Dr. Jason Fung’s encouraging experiences with his diabetic patients indicating how periodic fasting may make you brake through the metabolic resistance built up over time and where many of us for whatever reason seem to have been stuck.
Diana,
What does it take to be obsessed? How about succumbing to dementia unless you are?
High levels of blood glucose, even high “normal” levels, no matter how they’re acquired, puts you at risk of dementia.
How’s your memory? (How’s mine?)
http://www.nejm.org/doi/full/10.1056/NEJMoa1215740#t=articleTop
@JDPatten
Obsession is when someone thinks and believes that the ideal postprandial BG should be unchanged from FBG. Obsession is contemplating to eat a tomato or a potato and deciding not to eat it because it has some carbs.
I have posted the Kalahari Bushmen study for a start, there are many others (Pygmies, Pima, Kitavans etc.) that show rather conflicting results reflecting their metabolic flexibility and not rigid, mechanistic insulin and blood glucose levels as many like to believe – despite eating high carbohydrate diet. Look it up. I am not going to hijack this thread with this topic.
My memory is excellent, thank you. I eat quite some honey, maybe that’s why.
“Do bushmen in their natural habitat eat grains, wonder bread and drink soda? I doubt it. Cereal with skim milk and sugar for breakfast every single day?”
Do not get me wrong. I am not advocating Big Food Big Agra products. I am simply trying to explain that natural, whole foods are perfectly OK. Tubers, grains, seeds, fruits, mushrooms etc. included.
Diana,
You wrote: “All this “sugar is evil” and “keep blood glucose down” as much as possible talk sounds like obscession, really. And it has no mirror image in ancestral communities.”
As an outsider with a PhD (40 years ago) in an utterly unrelated aspect of chemistry, who really joined this site because of a very unpleasant reaction to statins, I do agree strongly with your statement! There are after all many traditional diets that depend on rice, and potatoes were a staple food for the Irish.
My sense is that Dr Kendrick is also cautious about extreme diets, except perhaps for those who are seriously ill. I sense that glucose could become the new cholesterol – something that patients and doctors compete to eliminate from their blood! There is tremendous value in avoiding excess in any direction!
That said, I do wonder if glucose in the form of sucrose – a big component of a Western diet – may be somehow worse because of the fructose that comes with it – starch breaks down into only glucose, of course.
David
I am looking at sucrose and other oligosaccharides from the point of view of a plant scientists. Environmental stress signalling, ROS scavenging, protection of membranes, role in circadian signalling…the list where sugars are implicated is long.
No, I am not afraid of sugars.
Very well put. LCHF movement should read about Rice Diet of Walter (Something Something? ). And the success he had with diabetics.
Processed sugar is evil no doubt. But overall, I would say listen to Dr Lustig rather than Wheat Belly people.
Diana,
The problem is not our ancestral communities, it is our present world soaked in sugar.
If you, like about 60 % or the world population today, are trapped in the metabolic ‘evil’ syndrome my belief (obssession?) is that it is very wise, like me and my wife, to do your best to get out of it by pressing your blood sugar levels down – though easier said than done if you are severely trapped.
If yo have pulled the long stick in the nutritional lottery world for whatever reason and is immune to this soaking – my congratulations. Then you don’t need to care very much about what you put in your mouth as with 90 % (?) of the world population and by the way myself 20 years ago.
Goran
“The problem is not our ancestral communities, it is our present world soaked in sugar.”
You are probably talking refined sugar added by Big Food to tasteless ” food products”.
I am talking sugar present in plants, or honey etc. that in its unrefined form is perfectly OK because it is accompanied by lots of other compounds and nutrients that the plant decided to pack with it. On purpose. The purpose is not to kill you.
Göran
I do care very much what I put in my mouth, believe me.
P.S. Have you missed my previous question about mushrooms?
Diana,
Dunno ’bout you, but to me, losing my memory and then my mind is a profoundly scary proposition.
Did you look at that link?
You seem quite certain of your viewpoint.
Have you ever had an A1C blood test yourself?
After having taken to heart Establishment Medical conventional wisdom on a “healthful” diet for decades, I recently found myself at the cusp of so-called prediabetes according to several A1Cs of 5.6% to 5.8%. That qualifies as the scary high normal. Four years of strictly whole foods with a strong leaning toward LCHF have not budged my from that mark.
Not being a medical professional, all I can do is get the best – hopefully unbiased – information I can find and then try to decide, as rationally as I can, what to believe and how to act.
‘T’s why I’m here.
I’m healthy, thanks for asking. I am not here to discuss my personal health markers but learn “what causes heart disease” (and compare to my own pet theory).
“You seem quite certain of your viewpoint.”
What viewpoint? Where’s the problem? It seems you advocate “whole foods” and I agree.
@Sasha, re: …these dietary recommendations go against all observational data we have on some of the longest living populations on Earth.
Populations with great health have a lot to tell us, but as I often say about, for example, the Blue Zoners: if you have BZ genetics, live in the BZ, follow the BZ diet and BZ lifestyle strictly, you can expect BZ results. Change anything, and all bets may be off, until more is learned.
re: What are they based on?
Results, mainly: longevity, and markers that strongly correlate to that, and can be minded.
Let’s consider dietary guidelines. Our national nutrition nannies are recommending diets that work for precisely no one, and these authorities have been obstinately blaming the victims for the consequences (“move more, eat less”). In the US, this would presently be the USDA’s MyPlateOfMetabolicSyndrome. Tom Naughton had an entertaining 44 minute take on the underlying policy problem at: http://www.fathead-movie.com/index.php/2013/12/17/speech-diet-health-and-the-wisdom-of-crowds/
The modern LCHF movement in the US can probably trace its roots to Atkins, although a century ago, before exogenous insulin, low net carb was the treatment for diabetes. In my extended family, there’s even a 1920s case of what we would now call a ketogenic diet successfully used to treat what was either acute pancreatitis or incipient T1D.
In the specific case of the program I’m working with, it was a matter of a cardiac physician seeing consensus and vegetarian dietary advice fail, then tinkering to discover what did work to prevent, arrest and reverse heart disease. Is it the final answer? Of course not. It evolves. But it’s effective enough that this MD walked away from a lucrative career as a stent and graft installer, and is now saving more lives writing cookbooks.
98+% of what passes for food in modern markets is unfit for routine human consumption. Many of the hazards presented have pronounced CVD risks (but food doesn’t explain all of it).
Interesting article on death certificates:
Why sugar is bad – the endothelial cells have no GLUT4 (glucose transporter). The endothelium is vulnerable (due to one cell thick) to injuries. What causes the injury – Postprandial hyperglycemia. Why – because the endothelium can’t resist having a high intracellular sugar. This causes OX damage and can kill the cells, then letting white blood cells get under them especially were the arteries are being bend – like around the heart. This is my best theory.
One small step – by the FDA – away from LDL surrogacy. Maybe.
http://cardiobrief.org/2016/06/30/fda-places-roadblock-on-approval-path-of-novel-cholesterol-drug/
Diana,
If yo don’t have a problem you don’t need to solve it.
But if you have a health problem and have solved it in whatever fancy way it sounds like a good idea to stick to the solution.
With a broad brush view I see myself that the metabolic trapping as probably being caused by excess carbs. Anyway, the health problem of both me and my wife resolved by cutting the carbs and replacing them with saturated fats. So – we stick to this solution.
Besides, as far as I have understood our physiology and metabolism the starch in a mashed potato turns into blood glucose as fast as table sugar. But again, if you don’t have any problems with your blood glucose you probably don’t need to worry much though about 60 % of the world population should in my mind worry.
By the way, I don’t believe in the “overeating hypothesis” as the explanation behind the obesity epidemic, metabolic syndrome trap, insulin resistance, since the explanation violates the fundamental basis of the first law of thermodynamics but few seem to acknowledge this fact. Though , Gary Taubes does indeed but he is physicist by education.
Gary Taubes misled quite many people with his “all carbs are bad.” I do not think accepting nutritional advice from a physicist is a good idea.
Diana, I fail to see why taking nutritional advice from a physicist (Gary Taubes for example) is necessarily a bad idea, when you consider the abysmal lack of nutritional knowledge of most doctors and even nutritionists. Gary delves into the chemistry and biochemistry of nutrition, in his books ‘Why we get fat and what to do about it’ and ‘Good Calories Bad Calories’. He has clear and well documented information and arguments for his position, the fact that he is a physicist is neither here nor there. Have you read those books? I would think not or you wouldn’t have the impression that he believes ‘all carbs are bad’.
Diana,
Have you read his “difficult to read” book “Good Calories & Bad Calories”?
This reading though takes some effort and it doesn’t hurt to read the book a couple of times to my own experience if you are seriously interested in the connection between eating habits and the metabolic syndrome. . It is in Gary’s and my own eyes all about how the nutritional/medicine establishment have been violating (misunderstanding?) the basic thermodynamics for more than a hundred years now. We, disciples of the natural sciences, tend to believe in the “truth” of fundamental thermodynamics.
I am not entirely sure that these two are mutually exclusive: fundamental laws of thermodynamics and the fact that sweet potatoes are quite possibly good for you.
Check out this link:
http://www.rawfoodsos.com/2015/10/06/in-defense-of-low-fat-a-call-for-some-evolution-of-thought-part-1/
Denise Minger does know nutrition.
Thermodynamics? It is not about the energy content of food as measured before you eat it, what matters is microbial action / sensing / fermentation and epigenetic interaction with the host. Fermentable carbohydrates (for instance potatoes are full of resistant starch as you surely know) provide food for gut flora that changes fibre, such as starch into SCFAs (short chain fatty acids such as butyrate, propionate, actetate etc.). Each of these SCFAs with distinct effect on your metabolic pathways, influencing satiety, appetite control, glycemic response, insulin sensitivity, endothelial health etc. This symbiosis is very ancient and cannot be fooled.
Some reading if you are interested:
Dietary Gut Microbial Metabolites, Short-chain Fatty Acids, and Host Metabolic Regulation (Kasubuchi, 2015)
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4425176/
The role of short chain fatty acids in appetite regulation and energy homeostasis (Byrne, 2015)
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4564526/
What a pity that Gary Taubes found no way to integrate tons of recent research on the role of microbiome in nutrition (even when faced with evidence that his hypothesis is not correct). Understandably, he cannot.
Concerning potatoes: in addition to fermentable fibre, potatoes also contain high load of vitamin C, folate, potassium, magnesium, copper, beneficial polyphenols etc. The potato tuber has regenerating properties, it can heal itself when damaged and fight pathogens. Some of these properties are retained even after boiling, actually some additional antioxidants are formed during cooking.
Diana: Thank you very much for the information and the links. The more I learn about the gut microbiome the more it appears to me to be such a crucial regulator of physiological systems that this is where we should be focusing our attention and health research dollars (along with the toxic environmental insults blithely approved and promoted by our human regulators). So many downstream effects from this under-appreciated organ, based upon its composition, diversity, and the type of food we give it. Just finished off the Independence Day cold potato salad (with home-made avocado oil mayo). Mighty good.
Thank you Diana, this is fascinating! Is there a book (or books) you recommend that deal with these issues?
Thank you.
Sasha, I don’t know if there is a book translating all this into nutritional advice (if that is what you mean). I am mainly reading papers on various topics. For instance, quite a lot of research comes from the Sonneburg Lab: http://sonnenburglab.stanford.edu/research.html
Diana, thanks for the link! I will start reading.
Interestingly enough, Russian folk medicine uses a lot of potato remedies like having a child with an upper respiratory infection breathe the steam off boiling potatoes, for example. I’ve seen it work now I can begin to understand why after reading your post.
Sasha,
No serious individual will deny that if you enter more calories into a closed system than is consumed by the same system the system will internally store those calories. This is the most fundamental law of thermodynamics, the first law indeed.
But to use this law, as the nutritional/medicine establishment do to EXPLAIN why we get fat is in my eyes (and Gary’s) utter stupidity – tautology in fact! In addition it is stupid since we are no “closed systems”, from a thermodynamically point of view, where this tautology can be applied and further that the two parameters, calories in and calories out in our bodies, are not independent in the thermodynamic equation.
I have always wondered why this should be so very difficult to understand and in my world you cannot simply dismiss this fact just because people doesn’t seem to understand it. It is only scholastics who can dismiss these fundamental physical fact and “get away with it”.
It has nothing to do with potatoes per se.
Taubes over-complicated things. If you excrete or burn fewer calories than you absorb, you must put on weight. It’s as simple as that.
What Taubes never mentions is “appetite”. Eating a poor-quality diet filled with sugar and empty carbs does not satiate. Alternatively, it takes a massive amount of sugary carbs to satiate. So on this type of diet people ingest too many calories because they don’t feel that they’ve had their fill.
I refer again to the Twinkies Diet. http://edition.cnn.com/2010/HEALTH/11/08/twinkie.diet.professor/
“For 10 weeks, Mark Haub, a professor of human nutrition at Kansas State University, ate one of these sugary cakelets every three hours, instead of meals. To add variety in his steady stream of Hostess and Little Debbie snacks, Haub munched on Doritos chips, sugary cereals and Oreos, too.
His premise: That in weight loss, pure calorie counting is what matters most — not the nutritional value of the food.
The premise held up: On his “convenience store diet,” he shed 27 pounds in two months.
What more evidence do you need that it is the quantity of calories that controls weight gain or loss, not the quality and balance of the macronutrients? (We are not talking about health issues, palatability, ease of sticking to diet etc, which are important in real world diets.)
Diana
I dont recall reading Gary saying all carbs are bad. Can you indicate where it is written?
Thanks
Gary Taubes never wrote that all carbs are bad at all. I’ve read his books & he doesn’t say that. He advocates lowering carbs, particularly highly processed ones, if you want to lose weight.
“I dont recall reading Gary saying all carbs are bad. Can you indicate where it is written?”
“Gary Taubes never wrote that all carbs are bad at all. I’ve read his books & he doesn’t say that.”
I admit I should not have put this phrase into quotation mark. However, “fattening carbohydrates” is the subliminal message you get reading his work, repeated over and over!
Some quotes from “Why we get fat and what to do about it” (Taubes, 2011)
“So far, the message is that carbohydrates make us fat and keep us fat.”
“Carbohydrates are not required in a healthy human diet.”
“…the fewer carbohydrates we eat, the leaner we will be.”
The picture is clearly more complex then that. Taubes had to learn the hard way:
http://www.vox.com/2016/7/6/12105660/do-low-carb-diets-work
Excess carbs are bad.
So is excess fat.
So is excess protein.
What’s your point?
Wow. Both diets tested aren’t that good for your digestive tract, IMO.
Göran
Concerning potatoes: sadly, you are a bit misinformed. Warning: starch, oligosaccharides and polysaccharides, vitamins, minerals, antioxidants (this also includes sucrose), polyphenols and other nutrients in potato tuber are my favourite topic. Including BG levels after the potato meal. You might be surprised. Unfortunately, such a lecture is out of the scope of this blog.
I for one am very interested in what you’d have to say about potatoes and what winds up in our blood. Particularly since it’s your favorite topic.
There doesn’t seem to be a clearly defined boundary to the blog’s scope.
Go for it. Why not?
I am interested too.
JDPatten: I second that motion. Diana always has something sensible and interesting to say which is worth reading. I must say that at times my eyes glaze over with all the test result numbers, macronutrient ratios, and so forth. I’m convinced that metabolic health is mediated primarily by food, and that there is a very wide variety of foods traditionally consumed by healthy populations among whom heart disease is rare. The Andean potato is one of these. I, too, am here because I want to understand heart disease, which took my father 64 years ago. Good metabolic health reduces the risk. We’re all a bit different, so dietary choices are a personal matter. I live almost entirely without grain and legumes. That’s my personal choice. Others may do fine with them, but for me, this allows far more vegetables and fruit down the hatch. And this is what produced the disappearance of nearly all visceral fat. I do eat tubers whenever I please. Hold forth with abandon, please, Diana. This is very much on topic. And I hope Dr. Goran answers your question about wild Swedish mushrooms.
JDPatten,
Me too!
If you believe that high blood glucose levels are not healthy and where most people tend to agree it is interesting to understand how this is regulated physiologically.
That this regulation is very complex in its simplicity is an understatement.
Here I find Professor Roger Unger, University of Texas, prize lecture 2014 very rewarding in adding fuel for thought about insulin resistance for the inquisitive minded.
I also find interesting Dr. Kraft’s clinical hospital research work on those many thousands of patients were he measured the ‘incredible’ scatter among individuals men he measure both blood glucose and plasma insulin levels over time after a standard 100 g instant glucose load.
Dr. Kraft’s conclusion after 30 years was that about 60 % of the western population are ‘diabetic’ to some extend.
Given a normal blood sugar level of 90 mg/dl and a total blood volume of 5 litres, we have a grand total of 4.5 g of glucose circulating in our bloodstream.
A 100 g instant glucose load is twenty times normal. It must be a massive shock to the system. I’m impressed that the body can handle it without keeling over.
Mind you, that’s the amount of sugar in one litre of Coca Cola, easily consumed at a sitting by many people. If you take cane sugar as 50% glucose, then a 2 litre bottle of Coke would give you the same shock load, plus 100 g of fructose to deal with as well.
Hmmmm…. Fructose is processed like protein. Taking glucose and protein together elevates the subsequent insulin spike above glucose or protein alone. So does the fructose in cane sugar cause a higher insulin spike than glucose alone would cause?
Effect of protein ingestion on the glucose and insulin response to a standardized oral glucose load.
Sasha said, “…overall, I would say listen to
Dr Lustig rather than Wheat Belly people.”
Did you miss Dr. Lustig’s page 69 in his
book Fat Chance, where he states that he
hasn’t been able to lose the 45 pounds he
gained in his residency? He can’t seem to
figure out that carbs turn to sugar in the
bloodstream.
Too many confounders Bill. You can easily loose 45 lbs and more on a balanced diet with complex carbs and exercise.
“You can easily loose 45 lbs and more on a balanced diet with complex carbs and exercise.” Perhaps what you meant to say is “I can easily lose 45 lbs and more on a balanced diet with complex carbs and exercise”. Or not.
Some people don’t lose weight easily at all.
Yes, people who don’t put enough work into it. The amount of work necessary is in direct proportion to what they did prior. There are sometimes genetic abnormalities but those are rare, I think. For majority of people it is a question of discipline.
Dear Sasha Gary Tabes and Nina Teicholz in their respective books go into the question of why ” putting enough work into it” is not he answer, and they convinced me. You should habve a go at both books.
Sent from my diPad, excuse les tipos, fautes d’orthographe etc etc.
>
I will, Chris. They are both actually on my list. Thanks
Sasha, there is absolutely no evidence that exercising more and eating less to lose weight has any permanent effect whatsoever. The vast majority of people who attempt this over and over again regain the weight and then some. It has nothing to do with discipline and everything to do with eating a high carb diet. And by high carb I mean all forms of sugars whether from sucrose or grains or starchy veg. When carbs are reduced it becomes much easier to lose weight and keep it off long term, even without exercising. I know this from personal experience and that of many of my friends and family, and there is a ton of (admittedly anecdotal) evidence from thousands of people on the net as well as studies by such well known researchers/doctors as Drs. Jeff Volek and Stephen Phinney amongst others. Einstein famously said that the definition of insanity is doing the same thing over and over again and expecting a different result. And that has been the case for so many people who have attempted to lose weight this way ever since the first Food Pyramid was brought out fifty or sixty years ago with absolutely no scientific evidence behind it, but plenty of influence and pressure from Big Agriculture wanting an outlet for their grains. Obesity has skyrocketed since then. What is so sad is that so many people do try very very hard to lose weight following conventional advice and failing, then are accused of being non disciplined and lazy.
Maureen, I agree with you on the Food Pyramid but that’s not what I said. (That’s a straw man, by the way). There’s tons of evidence on the importance of both exercise and eating sensibly as a long strategy for health and weight loss. In fact, that’s the only thing that’s ever worked in contrast to all the various diets out there. You can do a simple google search on exercise and weight reduction and I’m sure lots of studies will come up. In addition, exercise has a lot of other beneficial effects besides weight loss. You’re the second person on this thread to say that once you reduce carbs, you can reduce weight even without exercising. That’s not a good thing!
The strategy should be greater health, not just weight reduction.
Sasha, I do agree that exercise has many benefits apart from weight loss, didn’t mean to imply that it isn’t necessary. (although looking at my post, I did). What I should have made clear is that for people like myself who are unable to exercise very much due to a health problem one can still lose weight by reducing carbs. I have IPF which causes oxygen saturations to plummet on even mild exercise, but I do manage several 15 min. walks each day at a moderate pace and some weights three or four times a week, keeping an eye on my O2 sat and resting when it goes below 90%. I have been able to remain stable for five years with this regime without supplemental oxygen, along with a mostly ketogenic diet, and have lost 30 lbs over this time. The weight loss was actually an unintended (but welcome) side effect of the diet, which I embarked on after learning of the physiologic benefits especially more efficient mitochondrial energy production.
Thanks Maureen, I hope your health continue to improve.
Sasha
I do agree with you, unless you are obese loosing weight for weights sake is probably a waste of time. I find, anecdotally, that reduced carbs but not exercising, does not do the trick, metabolism, self delusion?
If you want a real subject for discussion rather than carbs/no carbs, try reading the Shangri La diet and then explaining why it works.
As for me, I am a cycling man trying to get rid of the weight I put on, following injury-induced ildeness
Mr Chris,
I don’t think self delusion, but yes to metabolism. Lustig touches on it in his Sugar: The Bitter Truth. And in addition to metabolism, exercise has so many beneficial effects on health, it’s almost hard to overstate it’s importance: immune, cardiovascular, metabolic, musculoskeletal, etc.
I agree with you, focusing on weight is misguided, especially since muscle actually weighs more than fat.
I will read about Shangri-la diet, thanks.
Chris, I looked it into it, very interesting. Probably does have something to do with Pavlovian conditioning…
Another curious one is Walter Kempner Rice Diet. Denise Minger talks about it on her blog:
http://www.rawfoodsos.com
That one is really hard to understand. It’s a carb disaster and yet he treated T2D, kidney failures, etc with it. All well documented.
Sasha, you would listen to Dr. Lustig, an endo specializing in children obesity before you would listen to Dr. William Davis, a practicing cardiologist, the author of Wheat Belly? Actually, Dr. Perlmutter preaches the same mantra as Davis but for Alzheimers and Parkingson’s? It all boils down to insulin, which Gary Taubes wrote his book about. I’ve been on the lifestyle of Wheat Belly 5 years – no hunger, no exercise (when I don’t feel like it) eat tons of food and have not regained an ounce of it……oh, and weigh 99 lbs. @ 4’11”. I feel great and never hungry.
Neicee, I would listen to either one of them, provided I can verify what they’re saying. Incidentally, why would you choose a cardiologist over endocrinologist when we’re talking about what are essentially metabolic diseases?
I did just pick up Wheat Belly book to see what Davis is saying.
Yes, I guess you missed it. It’s there
on page 69. Don’t try to tell me how
to lose 45 pounds. I already know.
Tell Lustig.
I am not trying to tell you how to loose 45 lbs, I know nothing about you. I was responding to you saying that Dr. Lustig was having difficulty losing it while in residency. Do you know what their lifestyle is like in residency? How can you say that the reason he was having difficulty was because he can’t understand that carbs turn into sugar?
Sasha:
Now I know you haven’t read Lustig’s Fat Chance.
Lustig said he hasn’t figured out how to lose the 45
pounds (which he gained in his residency) even
NOW, decades later. I’m coming to the conclusion
that some in this discussion are talking out of their
hat.
Bill: I can tell you myself that I didn’t read his book. I only listened to his talk on YouTube.
It’s well established that ketogenic diets will help you loose weight. But that in itself doesn’t say anything in terms of their long term health outcomes nor the wisdom of eliminating complex carbs (grains, tubers) from your diet.
Also, you can loose weight and reverse diabetes, etc on Walter Kempner Rice Diet (a carb disaster), Dean Ornish’s diet and so forth.
With respect to Dr. Davis, I don’t see how a grain we humans have been eating for 10,000 years can turn out to have been harming us all that time.
My main source of carbs is sourdough wheat bread. I know how much I eat because I bake my own. I go through a 2.5 kg bag of flour in 20 days, on average. That’s 125 g of dry wheat per day, and I have no problem maintaining my weight of 62 kg @ 5’2″ with little exercise apart from walking. In addition during those 20 days I might have small quantities of rice, potatoes, chocolate, biscuits and buns.
Some people appear to be carb-intolerant. Clearly I’m not.
For completeness, I intermittent fast (eating only between 1:00 pm and 8:00 pm), eat plenty of green veggies, small amounts of meat, fish, cheese, or eggs each meal, and 1 kg of butter a month.
Dear Martin Back,
I think you will find that the cereals we eat today have little to do with todays cereals after all the cross breeding that has gone on, perhaps Spelt from Crete.
In some quarters, since our current wheats have existed for say thirty years, this fact is held to be the source of all our woes.
Grass was around before the mammalian lineage explosion. Dinosaurs ate grass too (I guess including seeds). Maybe that’s why they went extinct, cereals killed them! [end of irony]
@Martin Back: “… I don’t see how a grain we humans have been eating for 10,000 years can turn out to have been harming us all that time.”
What’s in the modern market is not heirloom organic einkorn or emmer, and most people aren’t consuming it in historical doses, or using ancestral prep. But if we mimic the ancient diet, we can expect the ancient results, which include evidence of sobering trends in dental and cardiovascular ailments.
«Some people appear to be carb-intolerant. Clearly I’m not.»
The diet you describe is frankly low carb compared to most moderns. The sourdough process does blunt some (but not all) wheat hazards. You also appear to be getting some great fats, avoiding added sugar, avoiding industrial grain and seed oils, and dodging an encyclopedia of other hazards in processed food-like substances. This all matters.
Carb tolerance does indeed vary, and for reasons not yet fully elucidated. Number of AMY1 copies might be part of it; ApoE phenotype and Lp(a) status surely are. Whilst we await a reliable exemption test, people need to pick some metrics predictive of outcomes, and let those inform diet. I could propose a number of them, but I prefer to wait for Dr. Kendrick to get ’round to the topic of “so what do we do about all this, then”.
@Maureen H: re: no evidence that exercising more and eating less to lose weight has any permanent effect whatsoever.
Agreed. To stay on topic, exercise also has only a modest role in CVD management, in my view.
As I often put it to people who think it’s the #1 thing (or even the only thing) for weight, exercise is spectacularly inefficient for weight loss per se:
• it requires a discouraging level of effort per calorie
• it promotes appetite
• it replaces fat with muscle, and muscle is denser than fat
• some exercises are dangerous to joints in the seriously overweight
• recent science says that conventional wisdom about TEE is incorrect
(http://www.cell.com/current-biology/abstract/S0960-9822%2815%2901577-8)
It would be on my list of things for CVD prevention; just not terribly near the top. It has some effect on weight, but that’s outweighed, so to speak, by its other benefits. As the sole tool for weight management, exercise is almost certain to be a disheartening fail.
The “hit the gym” meme needs to be replaced by the “you can’t outrun a bad diet” meme.
Bob Niland: while it’s true that exercise is inefficient when you simply look at calories spent, exercise does other things like improving insulin sensitivity in muscle cells and speeding up metabolism which accounts for its effects in weight loss. Lustig covers it in his talk. Exercise also has an effect on brain and immune system plasticity. Sensible levels of exercise have incredibly beneficial effects on cardiovascular system and bone density. Without it you rapidly start loose muscle mass and bones start thinning out.
And it doesn’t matter that muscles weigh more than fat because it’s not about what your bathroom scale says!
Overall, I am sorry to say it bluntly, but your advice on what constitutes health is extremely confused. In my opinion.
@Sasha: re: I did just pick up Wheat Belly book to see what Davis is saying.
If that’s the original 2011 book, do be aware that his latest comprehensive overview is Wheat Belly Total Health (2014). The original book overlooked microbiome entirely, the targets for net carbs were not very prominent, plus other evolved details.
Yes, that’s the one I got.
@Sasha: re: Overall, I am sorry to say it bluntly, but your advice on what constitutes health is extremely confused. In my opinion.
That’s to be expected as I’m endeavoring to stay narrowly on topic (CVD), not set out a comprehensive self-empowered health optimization program; so then, only parts of the elephant.
What we now call Western culture didn’t always have the CVD pandemic we see today. Many mostly unmodernized ancestral cultures still don’t. What changed? What’s different?
I would argue that the majority (but not the entirety) of the explanation lies in diet, and any corrective or prophylactic steps need to start there.
Oh my, this is completely wrong in my opinion: “Yes, people who don’t put enough work into it. The amount of work necessary is in direct proportion to what they did prior. There are sometimes genetic abnormalities but those are rare, I think. For majority of people it is a question of discipline.”
I have always exercised, many times spending 10+ hours per week on my bike, or lifting weights, playing tennis, jogging, walking hours per day, etc. Even now, I workout three times per week, about an hour each time. During this time, I continued to gain weight. If I exercised an extreme amount (say 10+ hours/week on the bike), I would lose a tiny bit of weight. Which I gained back immediately once I stopped exercising (due to injury/riding season being over/whatever).
The only thing that’s helped me is carb reduction. With LC, then LCHF + intermittent fasting, I’ve lost 50+ pounds. While DECREASING the amount and intensity of exercise I was doing. I’ve gone from 4+ hours/week to 3 hours per week, and I exercise much easier now (no HIIT now). In fact, the only reason I exercise AT ALL is because I like it. I do not feel it helps weight loss in any way whatsoever. And basically all of the scientific evidence is in accord with this — weight loss is incredibly poor for exercise.
And it’s hard to meet anyone more disciplined than I am. I have almost three years of blood pressure data, 6+ months of weight data from two different scales (at home and at the gym), several weeks of blood glucose and ketone readings (the ketones taken three different ways, blood, urine, and breath) (I’m starting a ketogenic diet), it goes on and on and on.
I really take umbrage with statements like that. It’s more of “blame the patient”, and I get sick of that.
BobM: My experience exactly. I’ve never in my life made any conscious effort to lose weight, and have never had much of a weight problem, but even my marathon pictures show a tummy under the singlet. That went away in a short time when I stopped eating grains. Exercise is of little value in weight loss. Actually, I think it is a big mistake to focus on weight loss, when we should be focusing on metabolic health. Weight loss, if one has excess, will follow from improvements in overall health, and the gut microbiome is key to this. So food choices absolutely matter (though they are a bit different for each of us). I still do HIIT, about once a week, and 2-3 hours of body weight exercise three times a week; the purpose being to rebuild the muscle mass I lost over the decades. Makes me feel mighty good.
Anecdotes.
To all out there who are self-satisfied with your notion that anectotal evidence is inferior evidence, consider that all that can be known about you and your health and well being – or lack of it – is in your collected and interrelated anecdotes. Tell the story of your annoying symptoms, your specific lab results and pictures, your family history and your own detailed personal history, your full genetic code, and the detailed make-up of your microbiome. . . etc. They all add up to who and what you are, and where you might be headed. No one else’s anecdotal profile is the same as yours. Guidelines and protocols are derived (hopefully) from well designed RCTs using great numbers of individuals to find what might be effective for the average. Average! Not one individual is average. Protocols and guidelines are only guesses about you, the individual. That’s all they can be. Perhaps most of the time that guess is close enough, having mostly worked for Mr. Average O’Masses. But, the degree to which Medicine can get down and sort each individual’s unique set of anecdotes is the degree to which Medicine will have moved forward. It’s the degree to which a physician will (again, hopefully) be able to treat the unique you. We’re nowhere near, but there is a growing awareness of the direction to head.
With 500 millions T2 diabetics worldwide who can reverse their diabetic “doom” and skip all medicine by going strict low-carb, interest from Big Pharma is limited or perhaps even hostile more safe guess I presume.
Pure simple physiology and metabolism in my world of understanding!
Nicely put
What is so sad and increasingly obvious is that we have an obesity epidemic among young families. I observe with alarm young mums filling the shopping trolley with utter rubbish. No fresh veg or meat, rather packets of things, pizzas, bread, I could go on. They are no doubt working hard to make ends meet and have not got a lot of time. I am not blaming them, I just wish they were informed. Decrease carbs, increase real food, including potatoes and bread in moderation, especially for active children. Good nutrition is more expensive but not vastly so, and a LCHF diet seems to do the trick, so much evidence now. Take your children to the park and walk everywhere to be fitter and oxygenate your blood. We have destroyed our soil and so are deficient in trace elements, potassium, magnesium and more. Need more worms and hedgerows, less plastic wrap, less rubbish tele. Sorry for the rant, not very scientific is it.
Sylvia
I do not see that as a rant, but as an eloquent setting forth of what I belive and try to practise.
Sylvia. You are absolutely right but remember that this situation is a direct consequence of Ancel Keys, his flawed research and his commercial and financial adherents and government advice on nutrition, Disease – high blood sugar – control – feed starch (pure glucose) and sucrose (50:50 glucose:fructose) as fruit&veg. After all plants store energy as starch and sucrose and if it is good for them it must be good for omnivores. Sorry but in my old age I am getting very cynical about medicine and politics – I am unsure which are the most prolific liars
Nicely put. A scene from the animation “Wall E” depicts nicely where we are heading: https://scifiinterfaces.files.wordpress.com/2014/01/walle-hoverchair10.jpg
I do not take meds for T2 diabetes. I lower my A1c by eating less Sugar / Carbs.
When I take Meds and have a reaction or sensitivity to it … I believe my body does not need it and I look for an alternative. If my A1c is under 7, I believe I am doing good but reading this Blog, I will try a whole lot harder getting the A1c lower on my own.
Sasha wrote: ” Whichever country you’re in, look back 80 years or so and you will see that you ancestors from that point and back to beginning of time didn’t have high BG levels.”
Do we have any way of knowing what the BG levels of our ancestors were back to the beginning of time? While diabetes was documented as early as 1552 BC,
http://www.everydayhealth.com/diabetes/understanding/diabetes-mellitus-through-time.aspx
testing, as we know it today, is very new on the scene. Even as late as 80 years ago (1936), any kind of testing was in its infancy:
Click to access Owens_1.pdf
Eighty years ago, my ancestors — my parents and grandparents — were eating all kind of healthful food from their farms, but they also were eating plenty of sugar and flour — breads, cakes, pies, jams, sugar-canned fruits, you name it. Who knows what their BG levels were? Nobody had diabetes.
We do not know that nobody had diabetes. In fact we do know that some people did. A french doctor made the distinction between ‘thin’ diabetes and ‘fat’ diabetes in the 1880s. Cannot remember his name. Filed the information somewhere. I am not sure how he knew that fat people with diabetes had diabetes, as blood sugar measurement was not possible at that time.
Diabetes mellitus is an old disease (described in Ancient Egypt etc). Galega officinallis (alkaloid biguanide ==> metformin) use to treat blood sugar is documented in the Middle Ages and perhaps even before. Alkaloids bring us to potatoes… later, no time for more comments at the moment.
I agree but I didn’t say that nobody had diabetes. Old Chinese books classify it as Wasting and Thirsting disease so it was definitely there.
I do think fewer people had diabetes than now but that wasn’t because they all were hunter gatherers on LCHF diet. (Not that you ever said it but it’s being said on some Paleo forums).
My main point is: Eskimos do not have radically different health profiles than Okinawans, Kitavans, etc.
Oh, sorry Dr Kendrick. I thought you were responding to me.
Diagnosed by sweet tasting urine?
http://blog.wellcomelibrary.org/2013/11/diagnosing-diabetes-a-wee-taste-of-honey/
Time for a Blackadder quote
[Not having a present for Melchett, Blackadder offers a bottle of Baldrick’s urine.]
Blackadder: There was one thing ma’am, a fine wine from the far east. A most delicious beverage.
Queenie: Have a taste boys; tell us what you think.
Sir Walter: It certainly has plenty of nose.
Melchett: Oh yes, this is very familiar.
Blackadder: You’ll be delighted to hear there’s an inexhaustable supply of the stuff.
I seem to recall reading that astute doctors tested a patient’s urine for a particular smell, and sometimes by a sweet taste!
My Scottish gt gt Grandmother’s death certificate from the 1880s noted the cause of death as ‘diabetes mellitus’. One of her sons had the same cod some time later on. They were solid middle class folk and probably ate far too much sugar – this was a time when sugar was also getting very affordable and popular in the British Empire!
You’re right, I should have said: majority of them didn’t suffer from the metabolic diseases to the extent that we do. I think it had to do with lots of factors but not with LCHF. Most cultures ate carbs.
Trigger warning: TMI about my bodily functions.
You can monitor your own urine by tasting it. I’ve been doing it for months now, after reading an article that said, don’t think of it as consuming food, think of it as feedback on what your body is doing. As an engineer, the idea of feedback appealed to me. It’s not unpleasant once you get over the initial squeamishness. Urine is sterile if you are healthy. But taste it immediately, while it’s still warm, otherwise ewwww.
Healthy urine for me is a darker golden yellow colour with a full-bodied ‘meaty’ taste. (It’s hard to describe exactly.) If I go on a carb binge, 24 hours later my urine will turn a paler, more straw coloured yellow, and have a blander taste.
I got a huge fright when I bought a 2 litre sugary cool drink one day. I drank one litre that afternoon, and the second litre the next afternoon. Soon after finishing the 2nd litre my urine was a watery yellow and tasted as sweet as lemonade. I immediately started drinking lots of water to flush the sugar out of my system. It took a few hours of drinking and urinating before the sweetness was gone. I’ve never touched a sugary drink again.
Presumably, dumping sugar into urine is one of the body’s coping mechanisms for excess sugar consumption, along with increasing insulin production. Is it ever considered when testing the body’s response to sugar? I’ve never seen it mentioned.
Martin, in the days before the convenient blood glucose meters we now have, most self testing was via means of urine glucose test strips. The urine ketone test strips now available often also give a glucose reading. Glucose leaking out of a non-diabetic kidney during normal consumption sounds a bit dodgy though. Might need to test which exact sugar it is if you want to subject yourself to fizzy pop again. And i am wondering if some artificial sweeteners travel through unchanged?
Some may be interested in the following:
http://www.anh-usa.org/microsite/fda-deathmeter/
Your guess is as good as mine but the true number is probably between Starbridge’s 100,000 ( JAMA, July 26, 2000—Vol 284, No. 4) and this figure
And the authorities continue to ignore this number but concentrate on the 1 in 300 p.a. life saving properties of statins. BEWARE of Experts advice and thank Dr Kendrick for introducing some truth into the system
Mike,
I have one problem with statistics of this sort. It is never clear to me what these statistics include. For example, someone on drastic chemotherapy might die of the side effects of the treatment, but is this is, I suppose, a calculated risk in such situations.
How exactly do you define a death caused by drug treatments?
This is not, however, meant to belittle the problem of drug side effects – far from it.
David,
You are indeed right. Medical data unfortunately is so manipulated to produce the “right answer” that, as JP Ioannidis has shown (JAMA. 2005;294:218-228; PLoS Med 2(8): e 124; Arch Gen Psychiatry. 2011 Apr 4.; J Clin Epidemiol. 2011 Mar 29), one has to be extremely careful in assessing the truth. As an example it was claimed that 800,000 died because a guideline advised the use of flawed data involving the use of beta-blockers pre-surgery (you may remember Polderman) but the actual letter?? was taken down for “review” never to be seen again. We are now left with a number but no means checking it. My own attempts to check it suggested that 800,000 was credible but was probably a risk of less than 1%.
There are many references of deaths due to x, y, or z in the medical refereed literature and publshed attempts to collate the data into one figure ranging from Starfield to the cited website. As I wrote – your choice. Mine is Starfield’s as the most conservative but even that is horrifying and even more horrifying is the absence of any apparent attempt by the Big Pharma/medical establishment to correct or research the problem.
There was a question about Swedish mushrooms which I evidently have missed. So what was the question?
I pick some mushrooms myself in the wilderness and most of them blends well wild game. But you have to know which ones you are picking.
So, um . . . Dr. Kendrick, we’ve been on XVII more than two weeks. Longer than usual.
Is it your work-a-day schedule? The comments are still active? Having trouble with Subbotin?
Just wondering how this works and where we all stand.
Anticipatorially yours,
JD
Dr. Kendrick:
A complementary article to the Subbotin paper:
http://high-fat-nutrition.blogspot.com/2016/07/arteriosclerosis-6-and-subbotin.html
Not too long and worth your time.
Great post by Peter!
In my case … after a Heart Attack and one week later a blood clot in the middle of the heart … the report stated ” sensitive to many Drugs” . I do have a sensitivity to many drugs and at the time, before the Heart Attack, I told each Doctor and Hospital I was sensitive to the Ace Inhibitor Drug I was taking. The Doctors and Hospital seem to ignore it or admit that it was indeed possible. I am off all blood pressure pills and I am keeping it normal on my own.
Hi, how are you controlling it yourself. Did you stop the meds by yourself or with your doctors help. I would like to come off mine but am struggling to do so.
I follow the guidelines set forth by Dr. Bruce West in California. He heals his patients with Good Nutrition. Google him for details. You follow your own Doctors orders but you imporve your health with nutrition. When your nutrition heals your body … you ask your Doctor to take you off your meds. My Doctor sees my better test results and he takes me off the Meds. That’s a good Doctor / Patient relationship. I hope this helps.
Article in press today saying that statins reduce death from cancer: http://ecancer.org/news/9727-statins-may-be-associated-with-reduced-mortality-in-four-common-cancers.php
“A diagnosis of high cholesterol is associated with reduced mortality and improved survival in the four most common cancers, according to research presented today at Frontiers in CardioVascular Biology (FCVB) 2016.
“The 14 year study from nearly one million patients found that a high cholesterol diagnosis was associated with lower risk of death in lung, breast, prostate and bowel cancers……….
“Dr Carter said: “Our research suggests that there’s something about having a high cholesterol diagnosis that improves survival and the extent to which it did that was quite striking in the four cancers studied. Based on previous research we think there’s a very strong possibility that statins are producing this effect.”
How do they know that it’s not the high cholesterol that helps cut death from cancer ?
I just have to draw to your attention this article on page 18 of today’s (09/07/16) Times newspaper. It is headlined “Statins may cut the risk of cancer by half”. The second paragraph reads: ” Patients with …most common cancers were much less likely to die if they were being treated for high cholesterol, an analysis of more than 22000 people found.” That sounds clear and conclusive enough – until you read on and begin to think you are living in a parallel universe where things mean the exact opposite of what they say. I have to quote it in full: “…scientists used admissions to seven English hospitals a decade to look at the link between cancer survival and diagnosis of high cholesterol. FOR PATIENTS WITH SUCH A DIAGNOSIS, (my caps) the risk of death was cut by 47% in prostate cancer, 43% in breast cancer, 32% in bowel cancer and 22% in lung cancer” Note that the improvements in death risk were experience by people diagnosed with high cholesterol – not patients who were taking statins! We don’t even need to work this out for ourselves, as the final paragraph reads: “Paul Carter of Aston University, lead author of the study, conceded that he could not be sure if the patients were taking statins and that the effect could even be explained by high cholesterol itself!!!!”
(my exclamation marks)
Thought I’d slip this interesting article in while quietly waiting for XVIII:
Eat fish; live.
http://www.medscape.com/viewarticle/865835?nlid=107950_2981&src=wnl_dne_160708_mscpedit&uac=25547DG&impID=1150113&faf=1
Semin Thromb Hemost. 2015 Apr;41(3):315-22. doi: 10.1055/s-0034-1395352. Epub 2015 Feb 19.
The effect of omega-3 polyunsaturated fatty acids on fibrin and thrombin generation in healthy subjects and subjects with cardiovascular disease.
McEwen BJ1, Morel-Kopp MC1, Tofler GH2, Ward CM1.
Author information
Abstract
Hypercoagulability plays a key role in the progression of cardiovascular disease (CVD). Although omega-3 polyunsaturated fatty acid (PUFA) intake has been inversely related to the risk of cardiovascular events, the mechanisms are not fully understood. The aim of this study was to investigate the effects of omega-3 on novel markers of global coagulation. The generation of fibrin and thrombin, measured via overall hemostasis potential (OHP) assay and calibrated automated thrombography, respectively, was determined in 40 healthy subjects and 16 patients with CVD at baseline and after 4 weeks of 640 mg/day omega-3 PUFA. In healthy subjects, fibrin generation was significantly reduced, as measured by overall coagulation potential (p = 0.013), OHP (p < 0.001), velocity of fibrin polymerization (p = 0.002), and significant increase in delay to fibrin generation (p = 0.002). The peak of generated thrombin was significantly reduced (p = 0.043). In subjects with CVD, omega-3 PUFA significantly reduced OHP and significantly increased the lag time to thrombin generation (both p < 0.001). Treatment with omega-3 PUFA had no effect on other fibrin and thrombin generation parameters in CVD patients. Four-week omega-3 PUFA supplementation reduced thrombotic potential in healthy subjects, as shown by reduced fibrin generation and peak thrombin. There was a greater effect on fibrin generation in healthy subjects compared with those with CVD
@JDPatten: Eat fish; live.
Which advice they then sabotage with ritual chants from the canon: “But of course we want to encourage people to also eat their … and … and whole grains,” she said. This and other studies “all suggest that … and … and healthy oils should be emphasized…”
Whole grains (wheat, let’s be honest) even with the with germ and bran, is still an all-purpose human toxin. Since they fouled on that, it raises suspicion on what they think is a healthy oil.
Anyone who adds more fish to their diet (and/or ω3 DHA&EPA supplements), but doesn’t dial the grains to nil, and also fails to do something about our seriously high modern exposure to ω6 linoleic acid (from seed and grain oils), may be disappointed in their CVD outcome.
Another interesting article, sure to inspire ire. Fats vs. other fats vs. carbs:
http://www.medpagetoday.com/PrimaryCare/DietNutrition/58926
JDPatten: Another example of rubbish from the Harvard School of Public Health. The massaging of exceedingly unreliable data into an outcome the authors dearly wished for. Means nothing.
You would think that by this time people would be cautious on lowering cholesterol reducing risk of heart attack and stroke.
But this article on the bad neurological effects of Statins:
http://www.scientificamerican.com/article/do-statins-produce-neurological-effects/
starts, “These drugs are typically prescribed to lower cholesterol and thereby reduce the risk of heart attack and stroke.”
re: You might further believe that that what is written on death certificates is an accurate record of cause of death
And, no real surprise, it’s still iffy today; just published:
Neurology: Sudden neurologic death masquerading as out-of-hospital sudden cardiac death
http://www.neurology.org/content/early/2016/09/16/WNL.0000000000003238